


Article Figures & Data
Figures
- FIGURE 1.
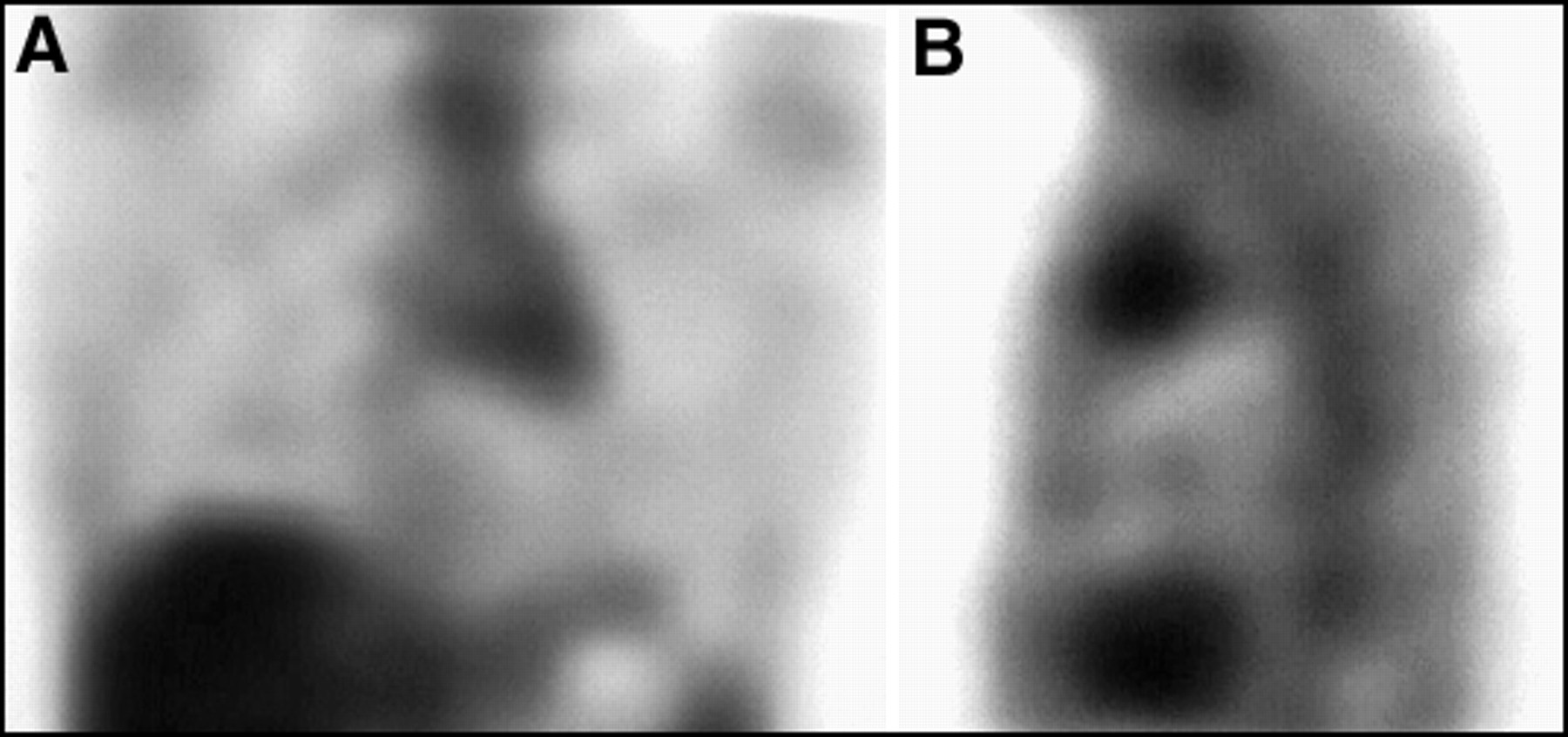
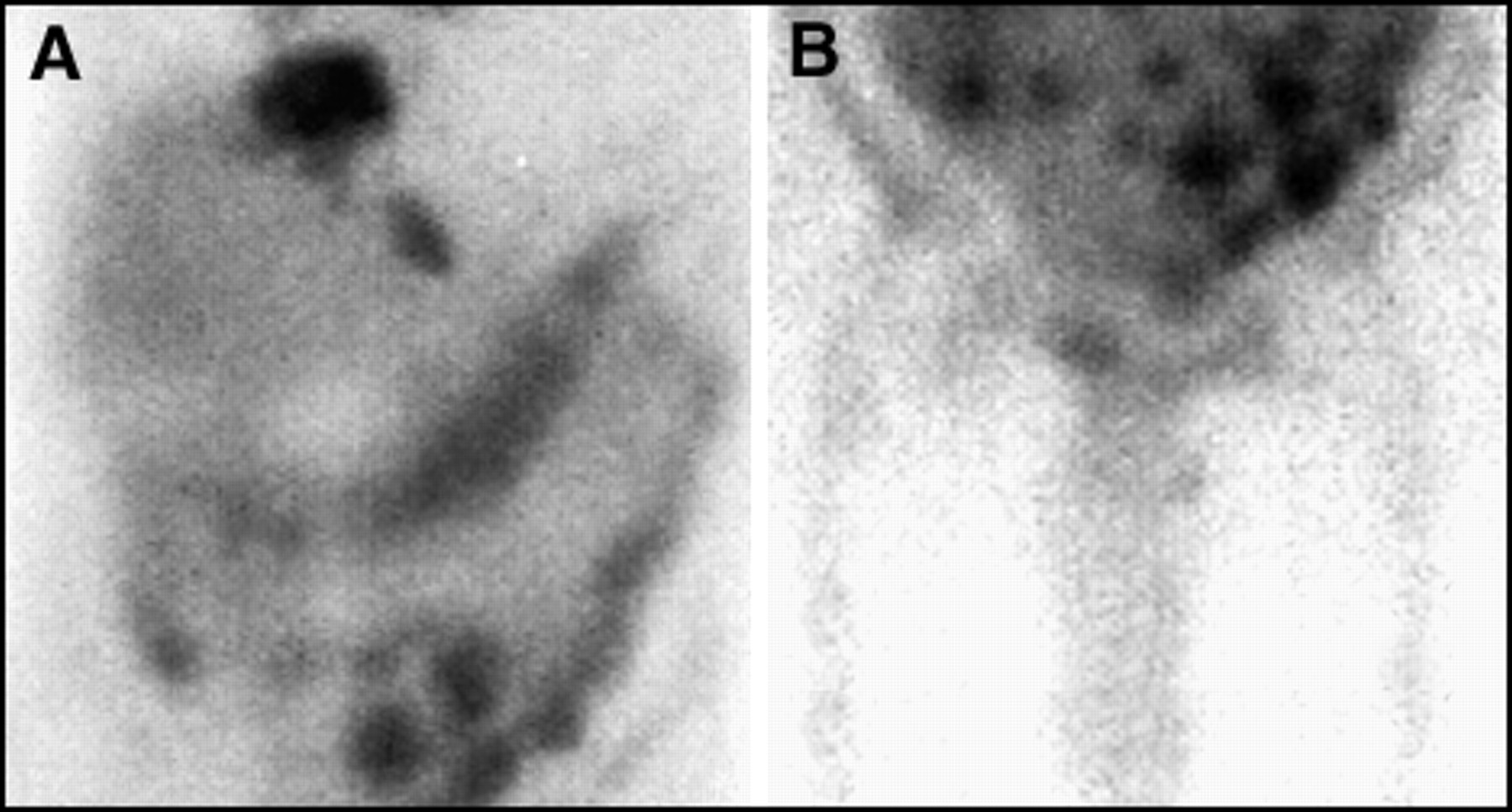
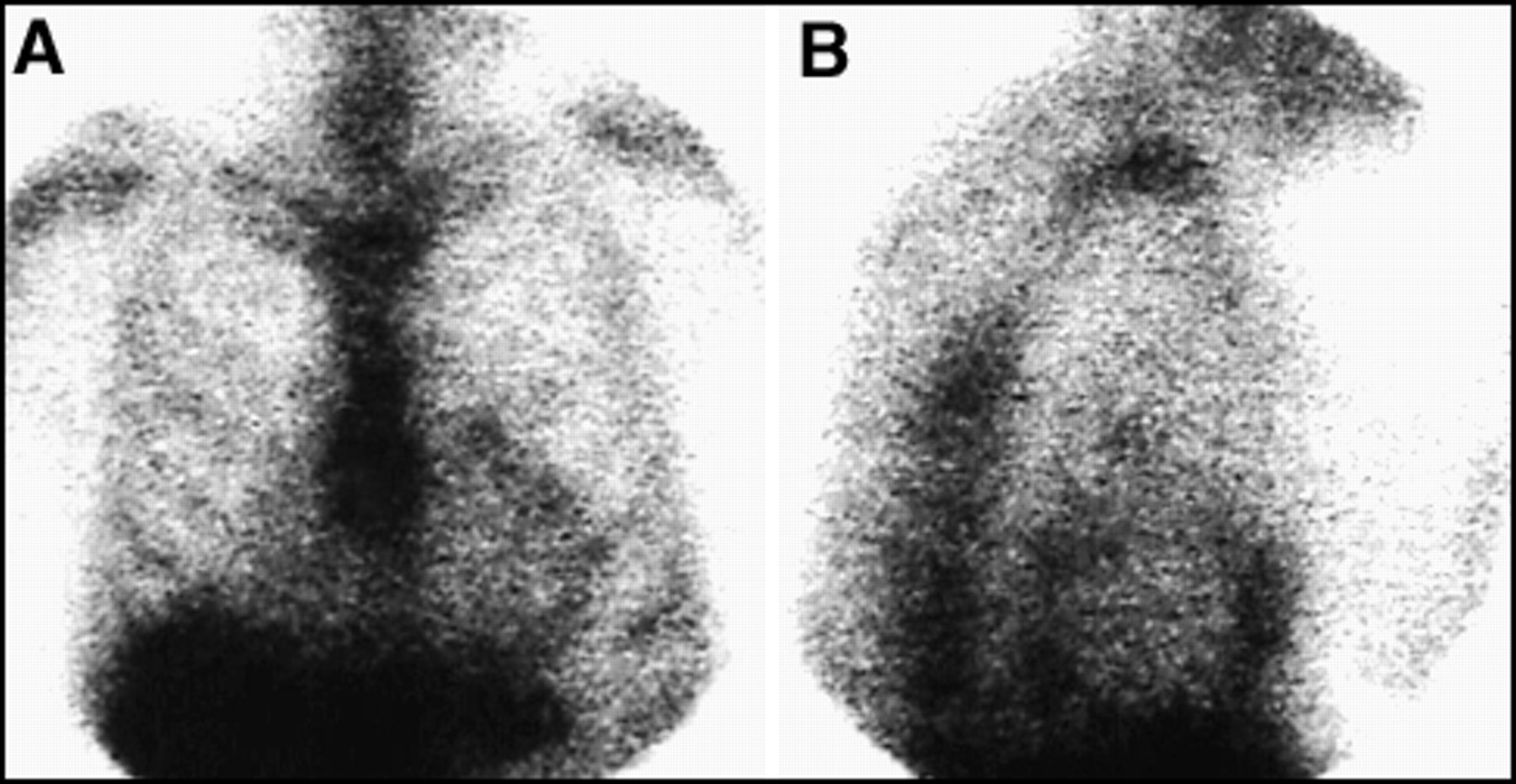
The 67Ga scan can be useful as an adjunct to staging. Two hilar nodal groups were suspected in this patient with Hodgkin's disease, who would have been assigned a stage II classification. Gallium-67 images of the chest, (A) anterior planar and (B) posterior planar, also reveal additional nodal groups and the presence of multiple bony mets, placing this patient in a stage IV category.
- FIGURE 2.
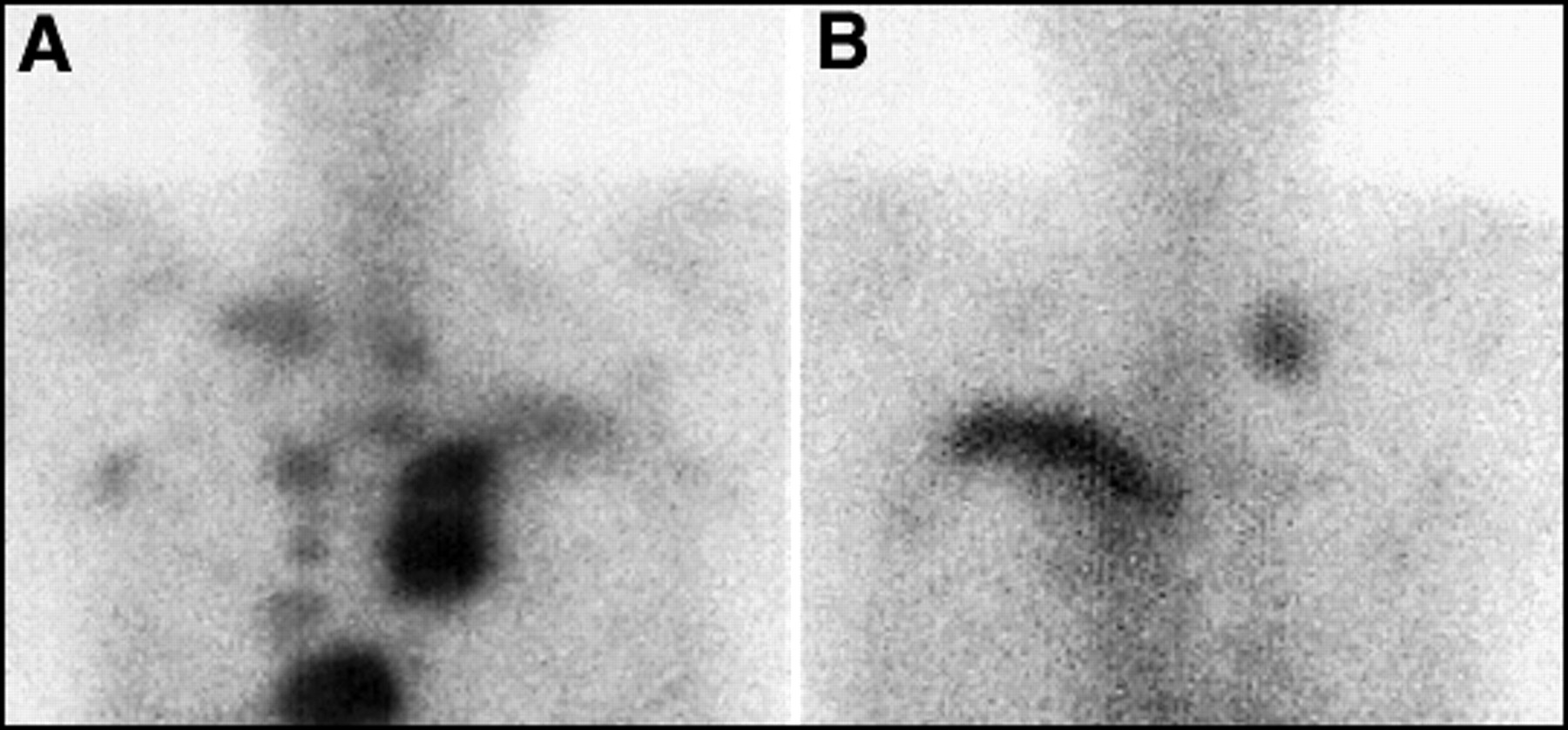
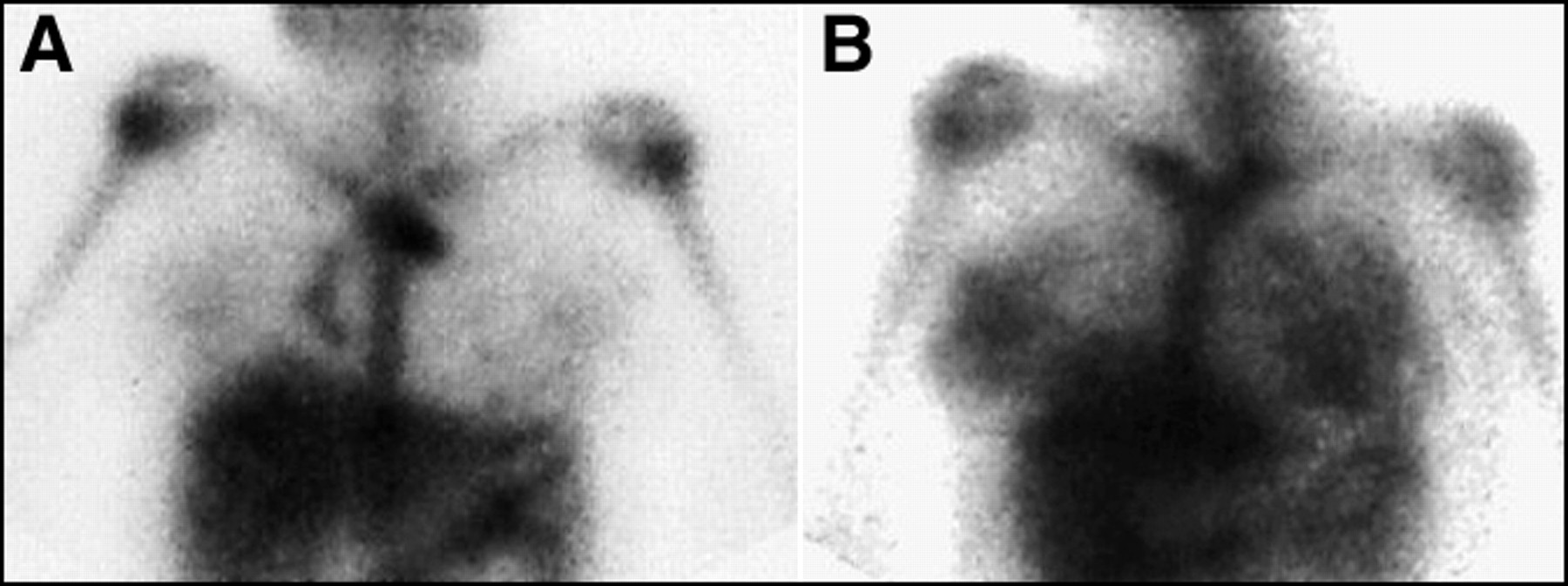
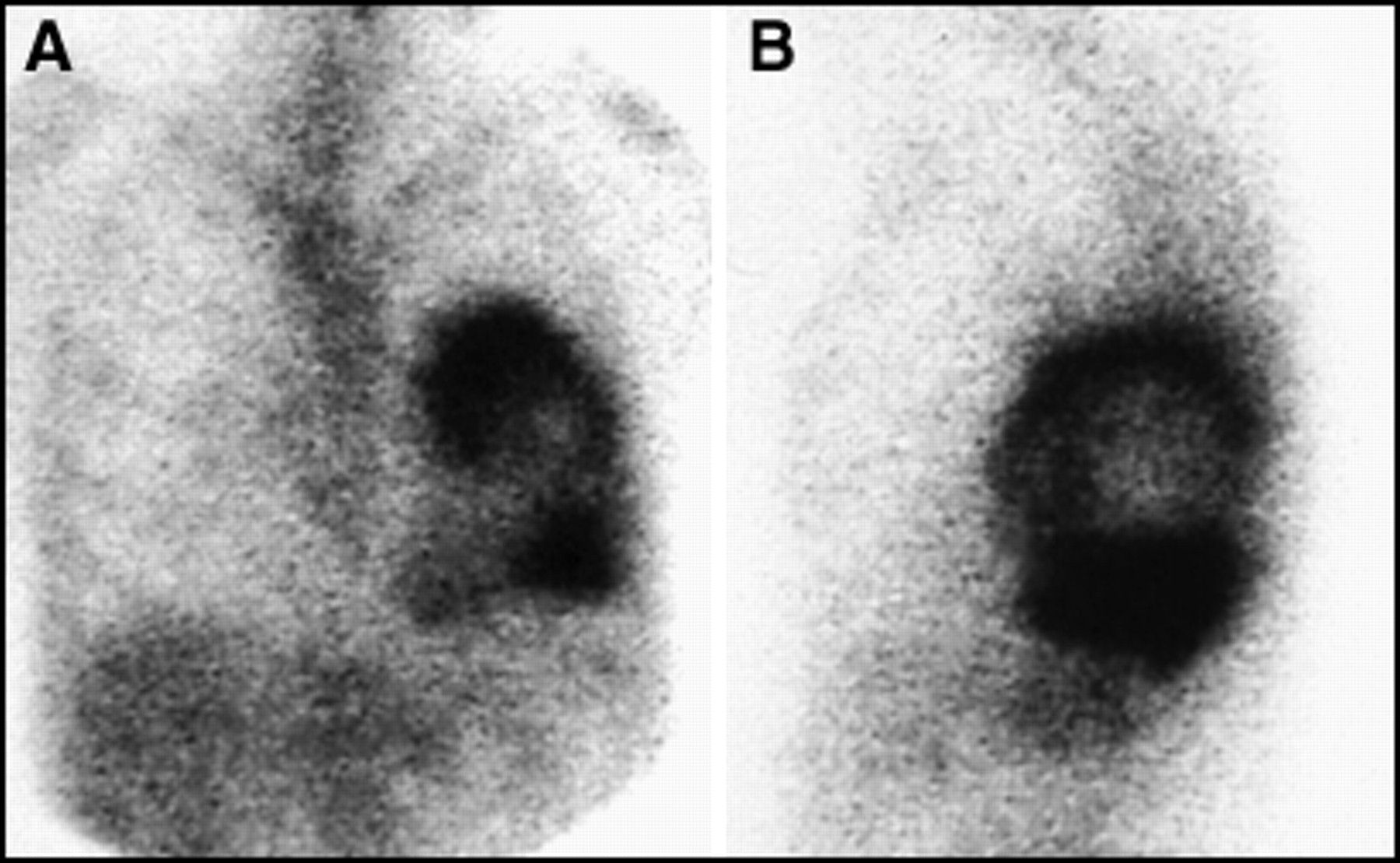
Successful treatment of lymphoma is demonstrated by 67Ga scan. (A) This patient had bulky mediastinal and supraclavicular disease before therapy. (B) After therapy no residual disease is found.
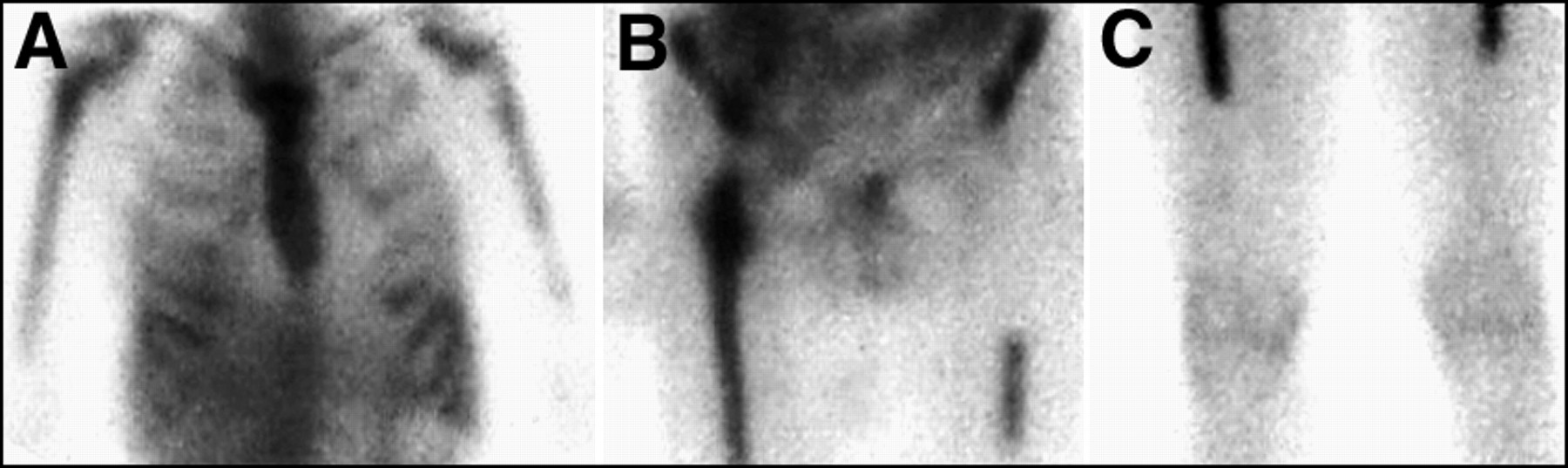
- FIGURE 3.
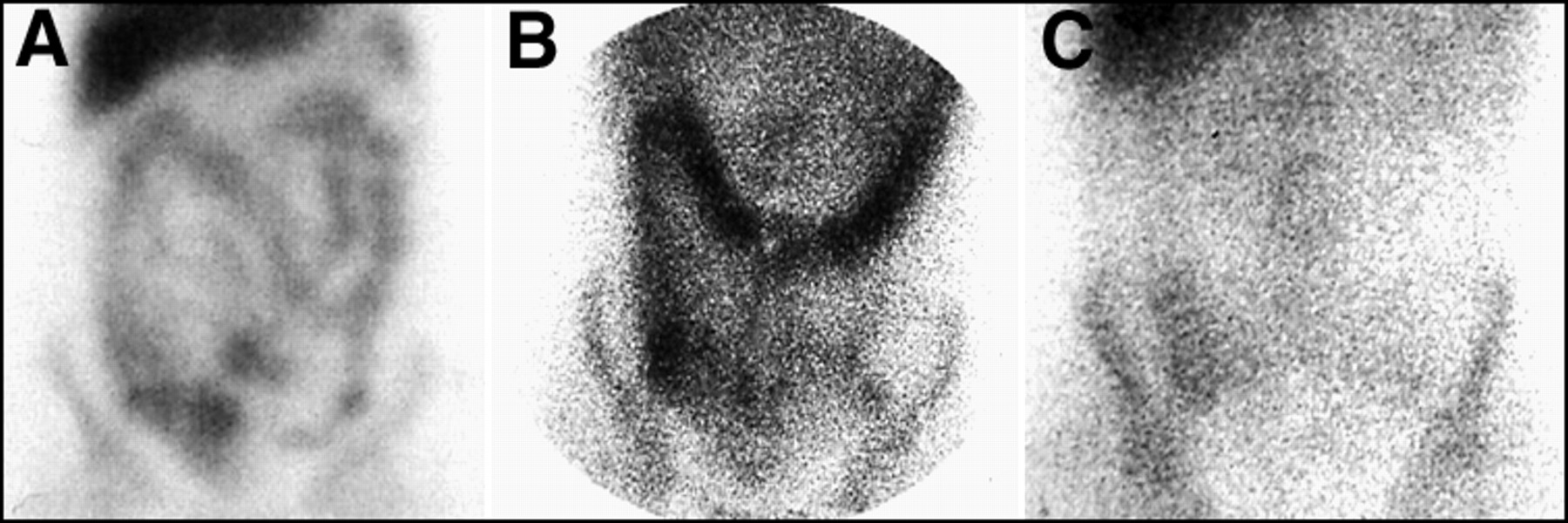
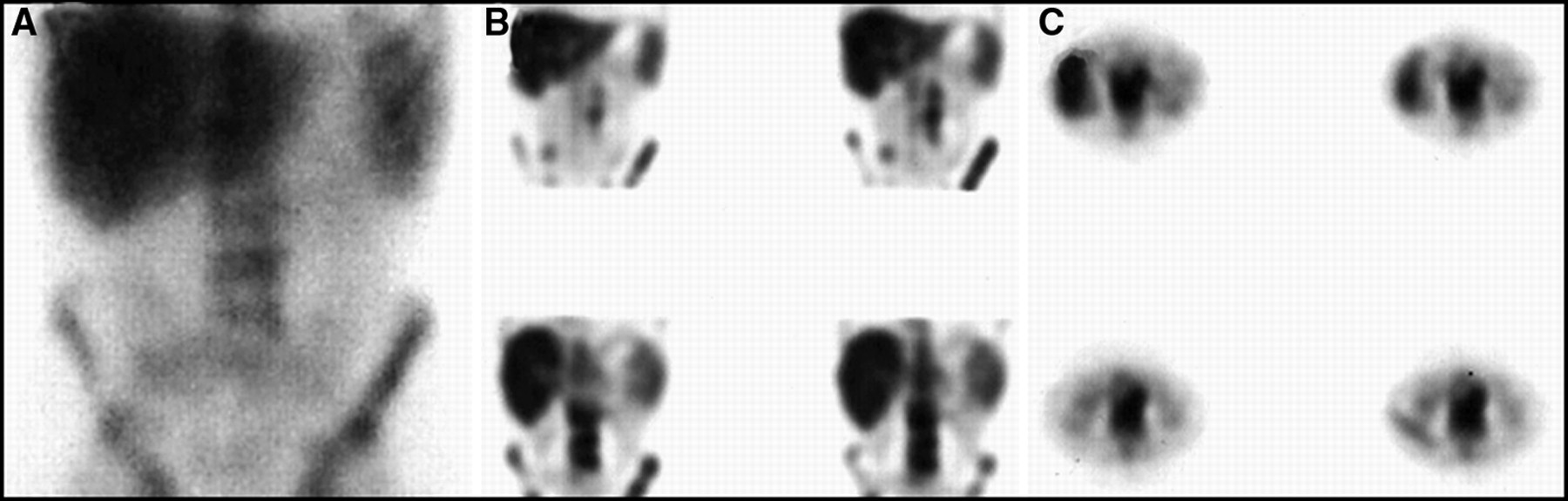
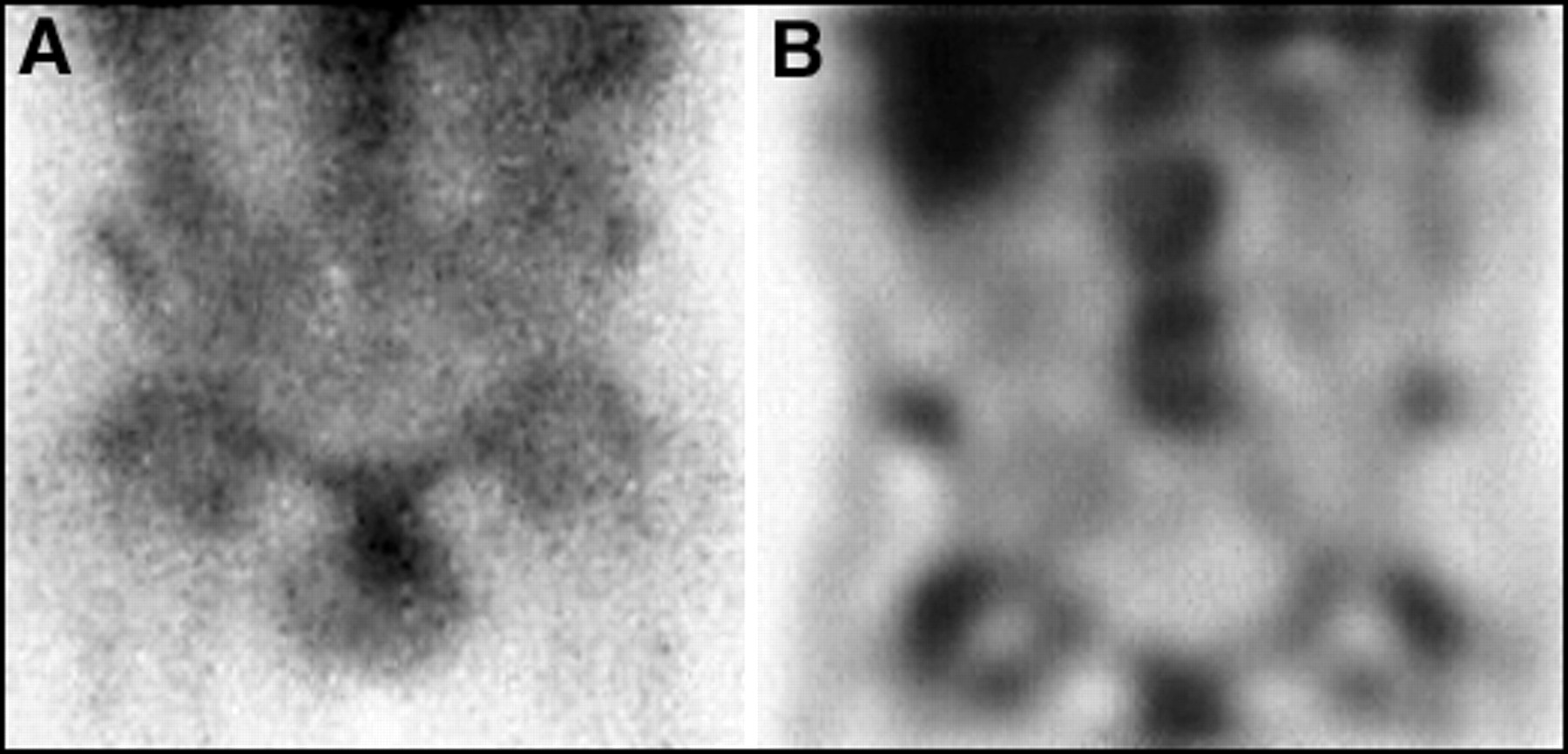
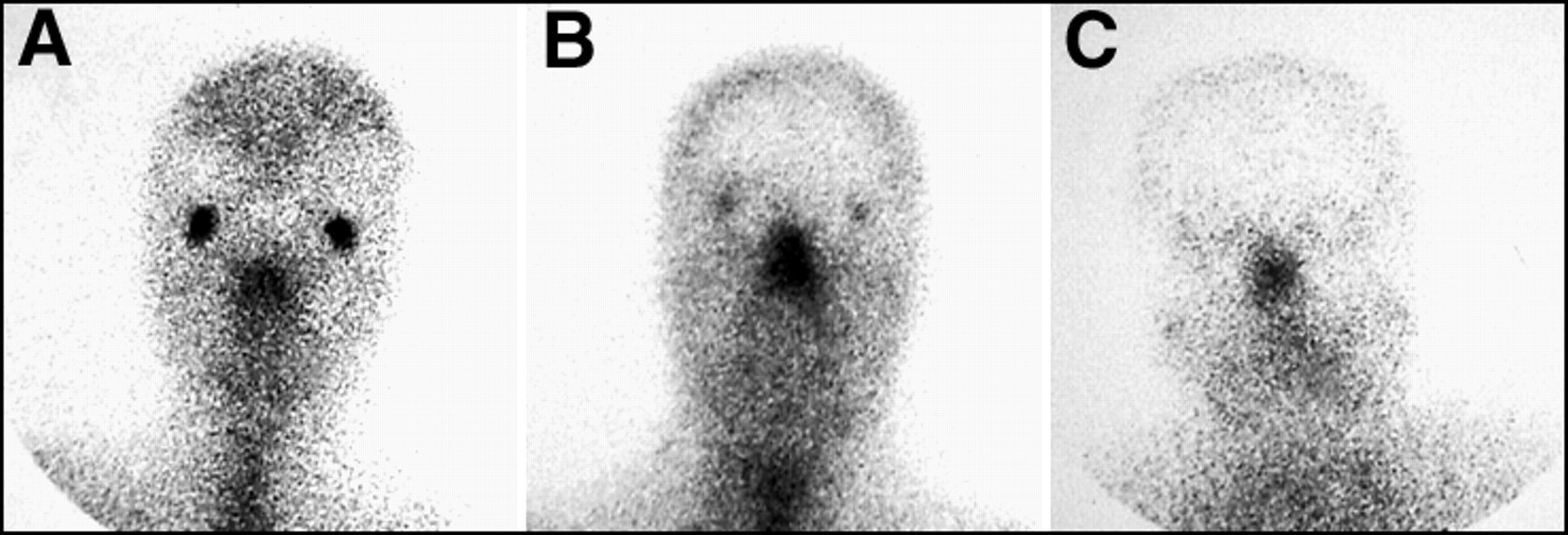
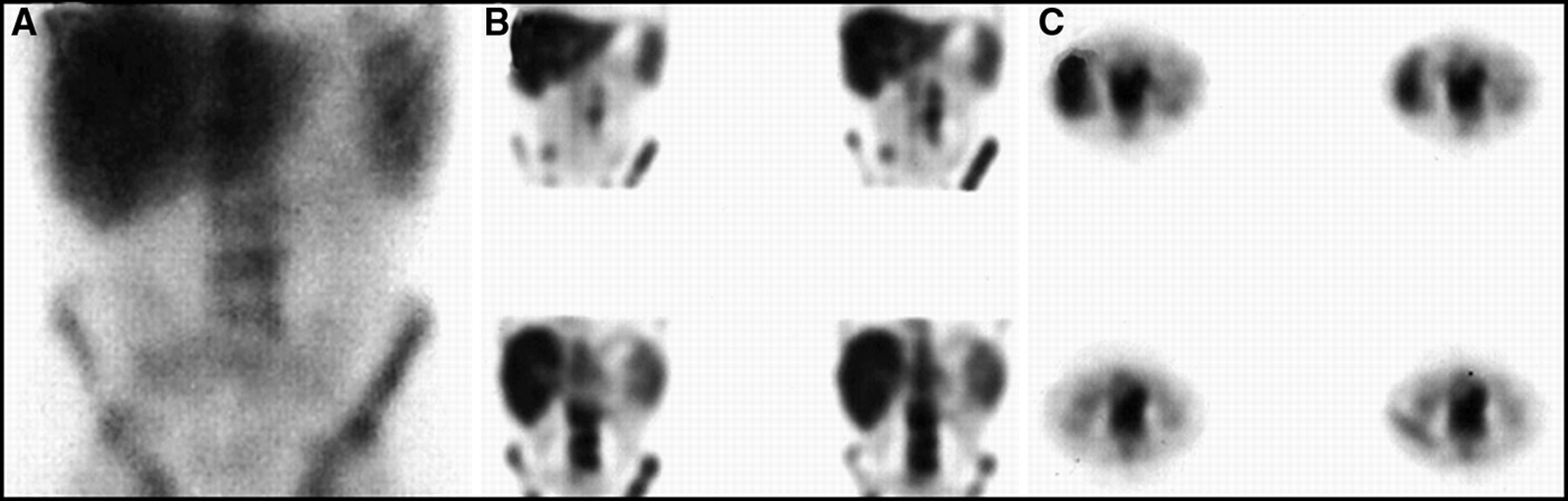
Normal patterns of facial uptake of 67Ga are variable. Activity in the lacrimal glands can range from (A) intense to (B) moderate to (C) absent.
- FIGURE 4.
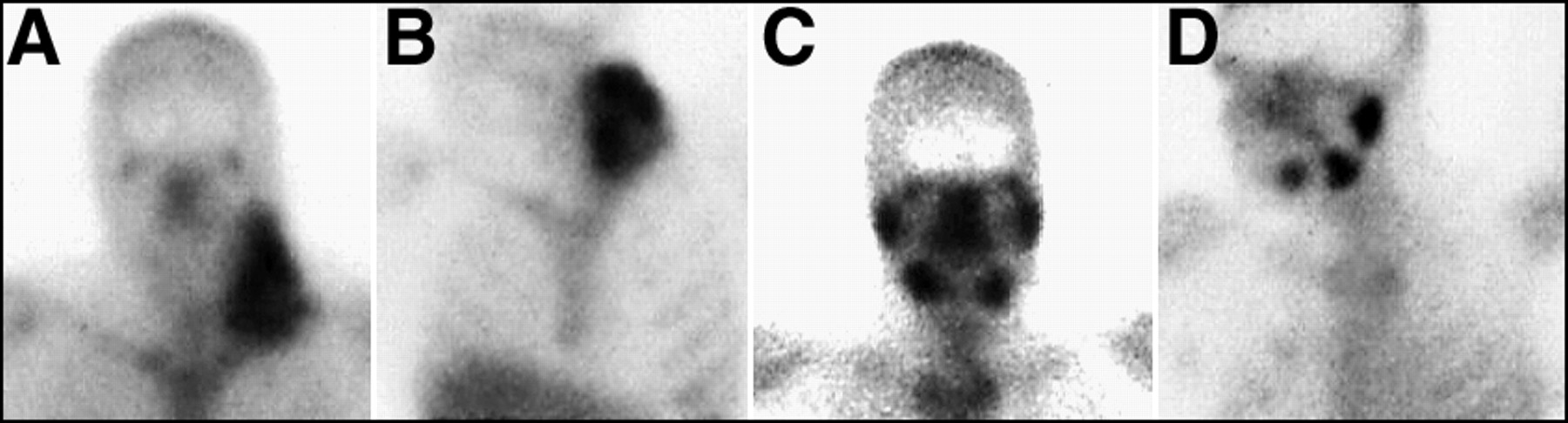
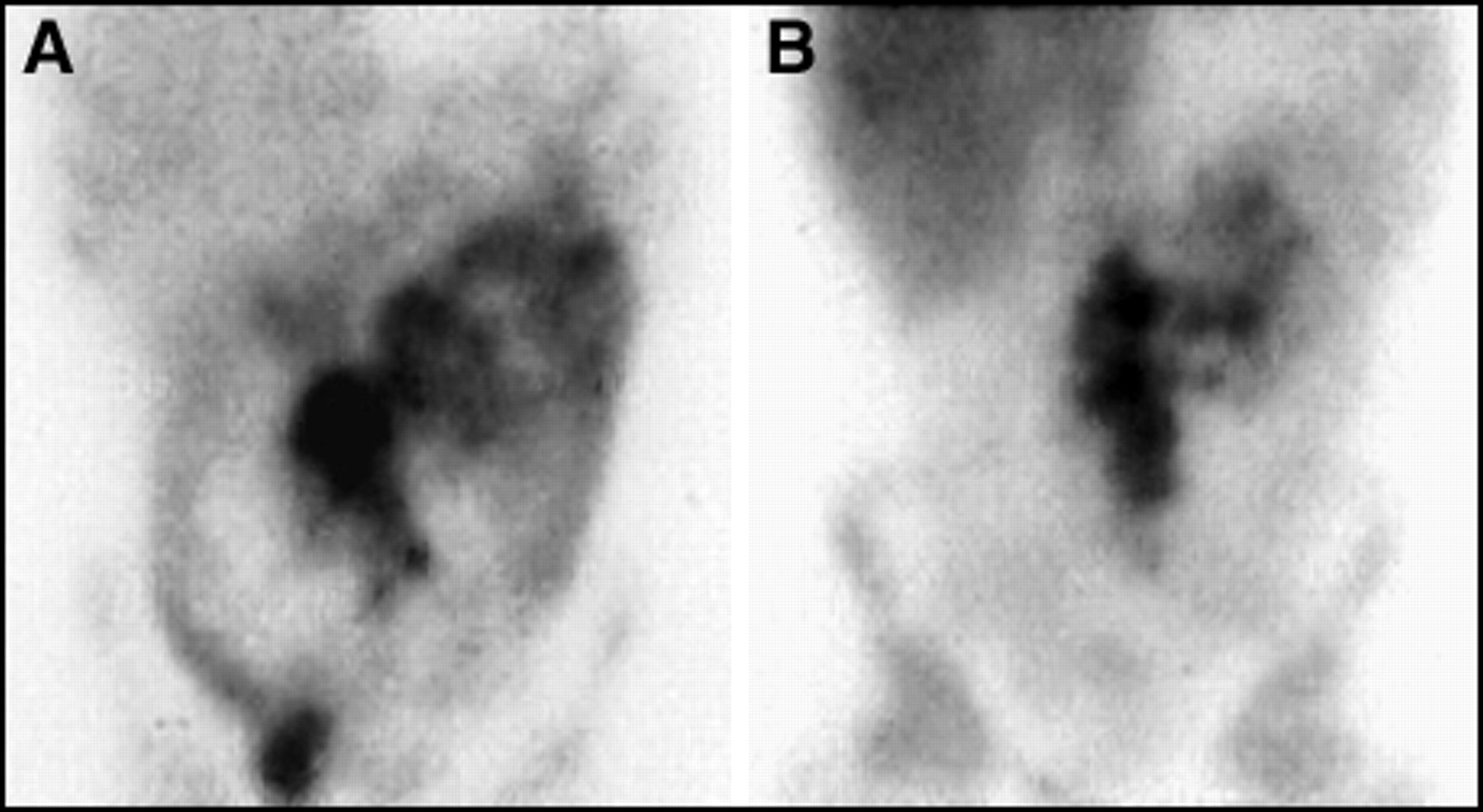
Sialadenitis is a common complication after chemotherapy and radiation. (A) Anterior and (B) lateral planar views of the head and neck before therapy demonstrate a large left neck tumor. After therapy, the tumor is eradicated but there is intense activity seen on both the (C) anterior and (D) lateral planar images in the parotid and submandibular glands. This is not lymph node activity.
- FIGURE 5.
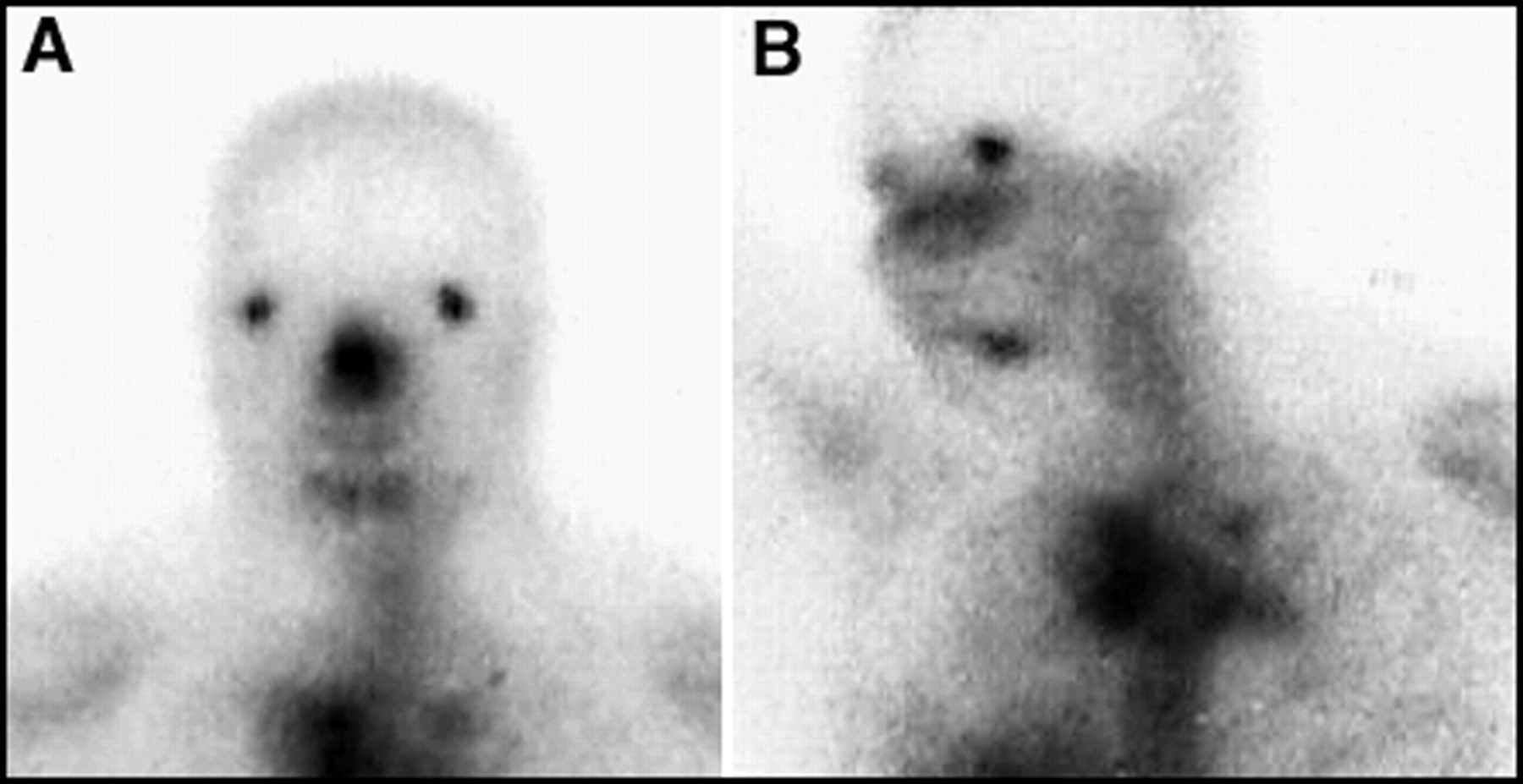
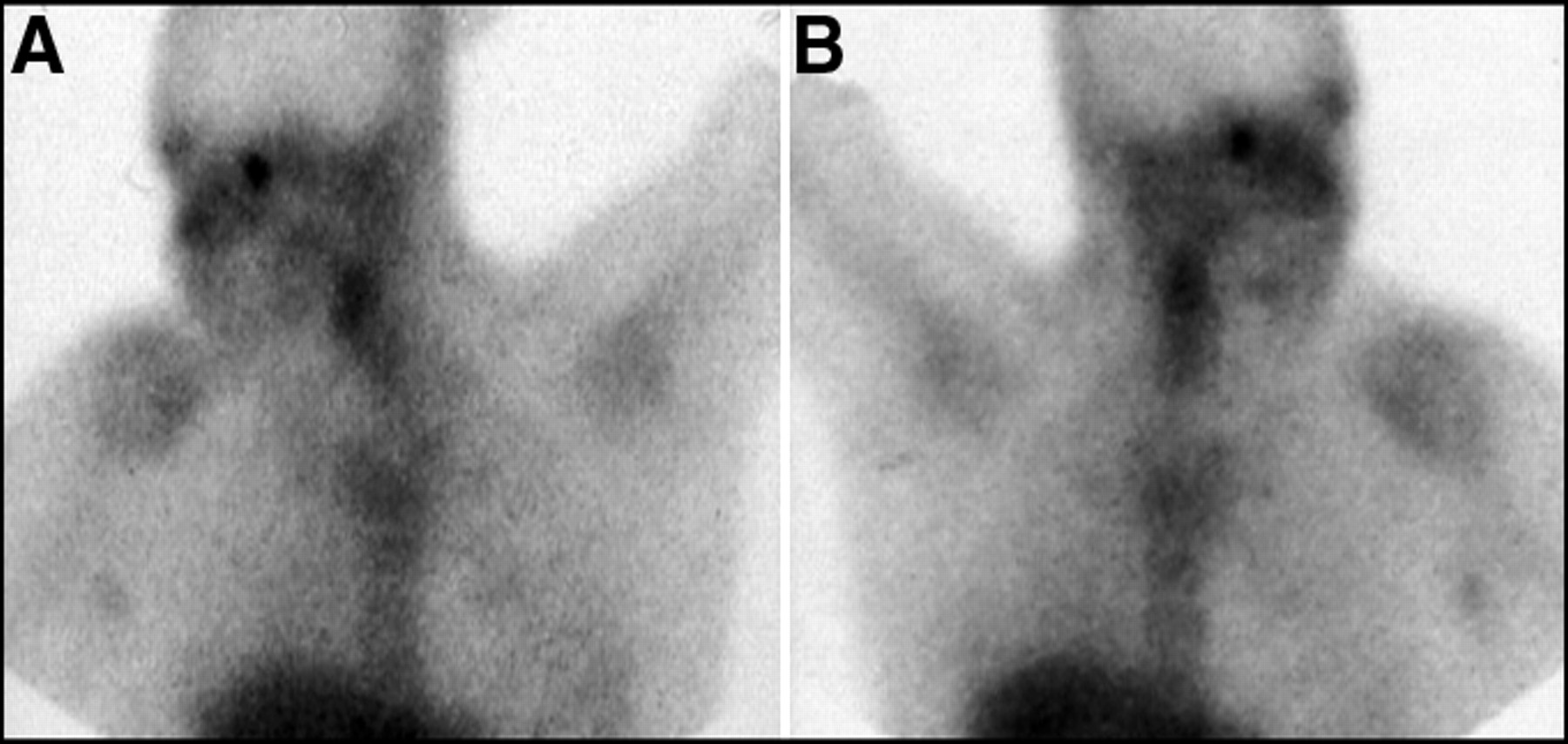
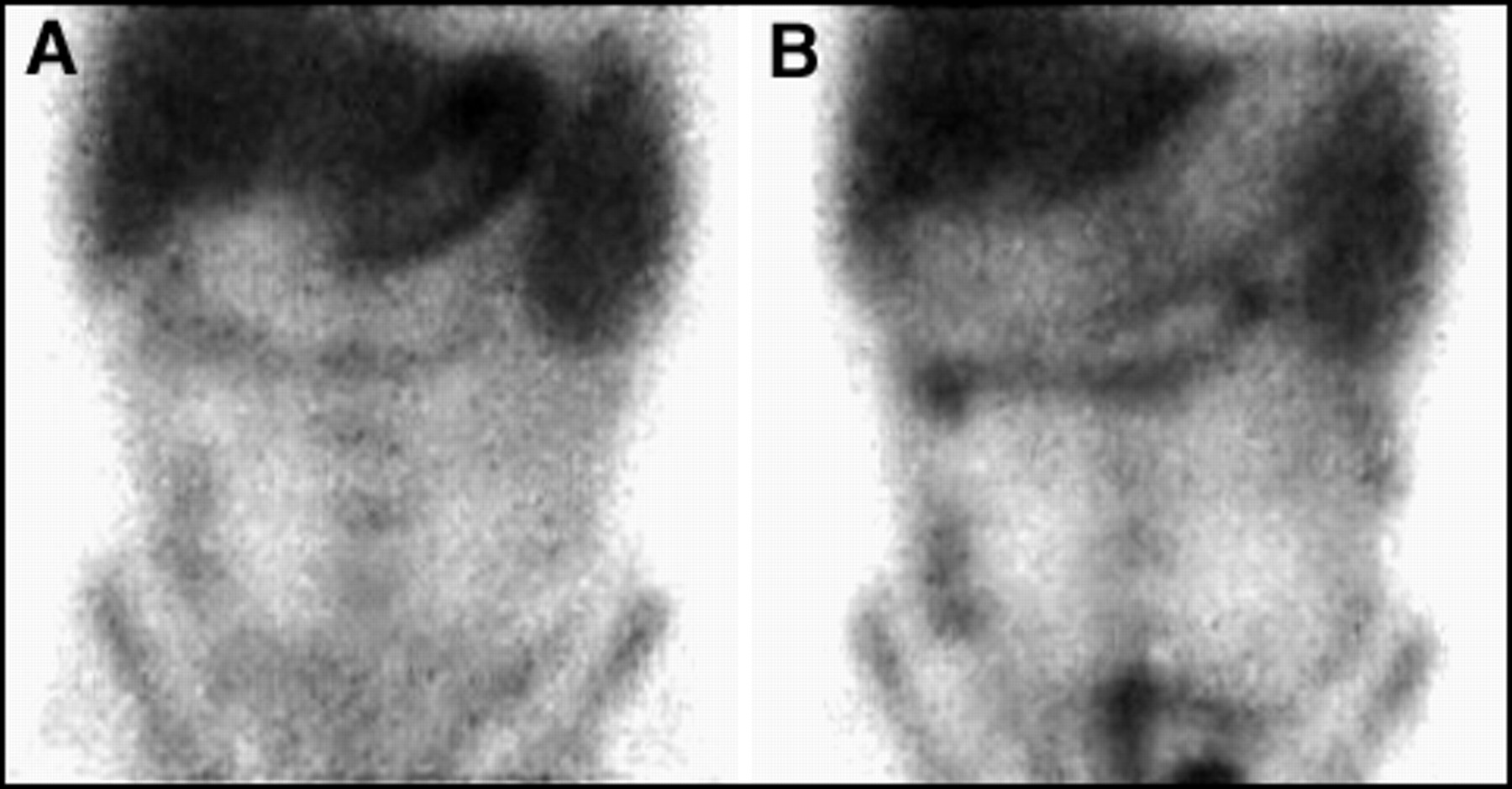
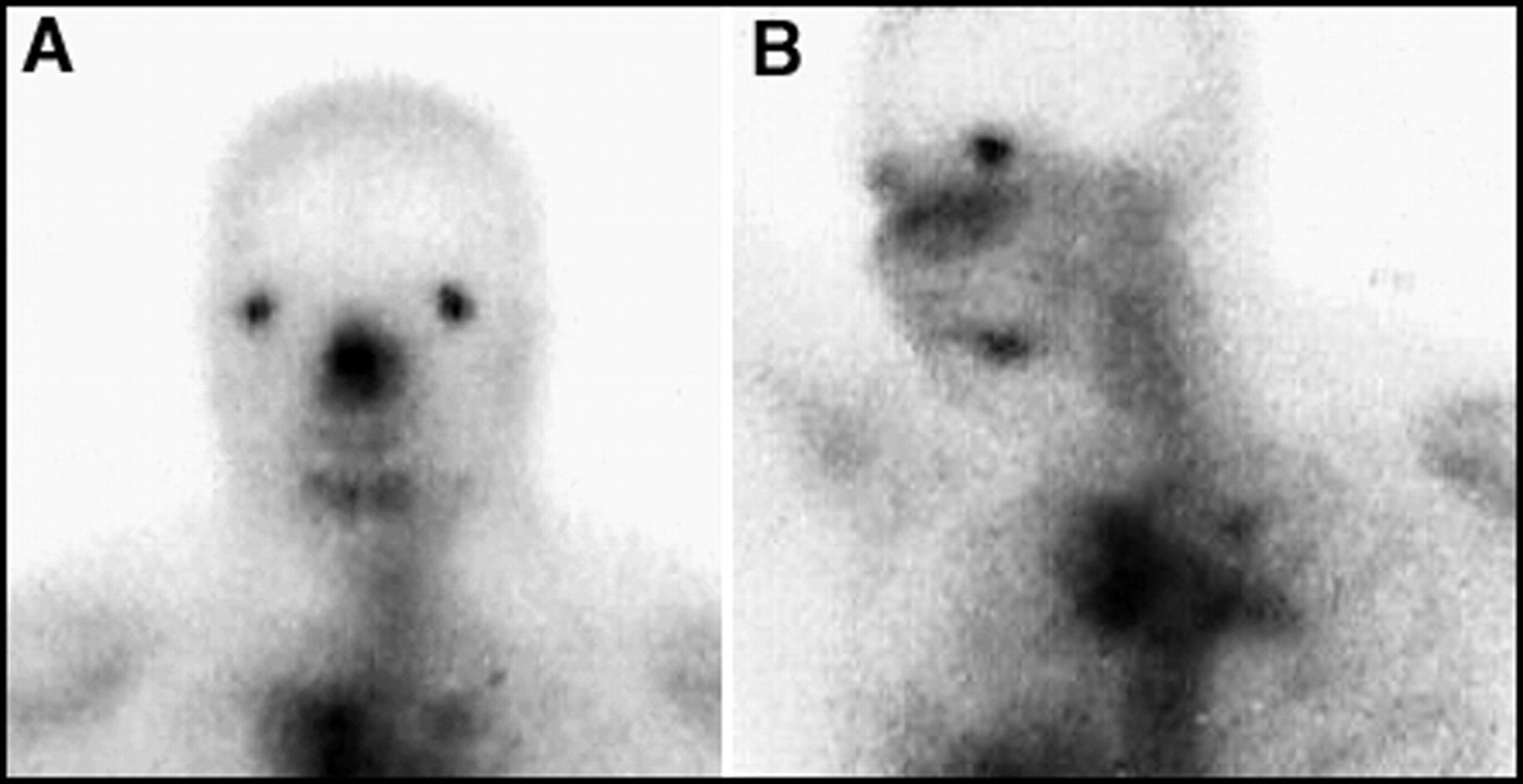
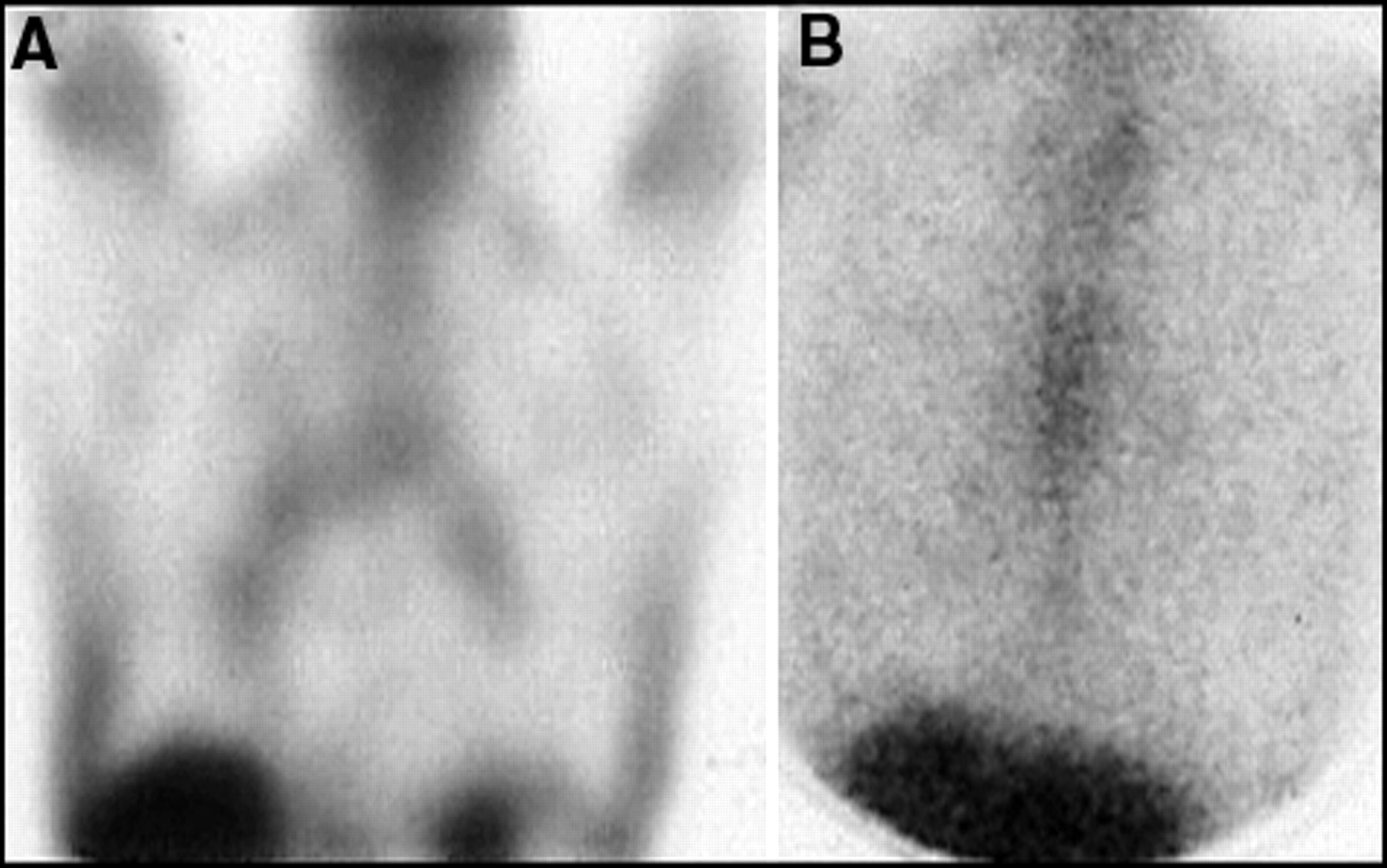
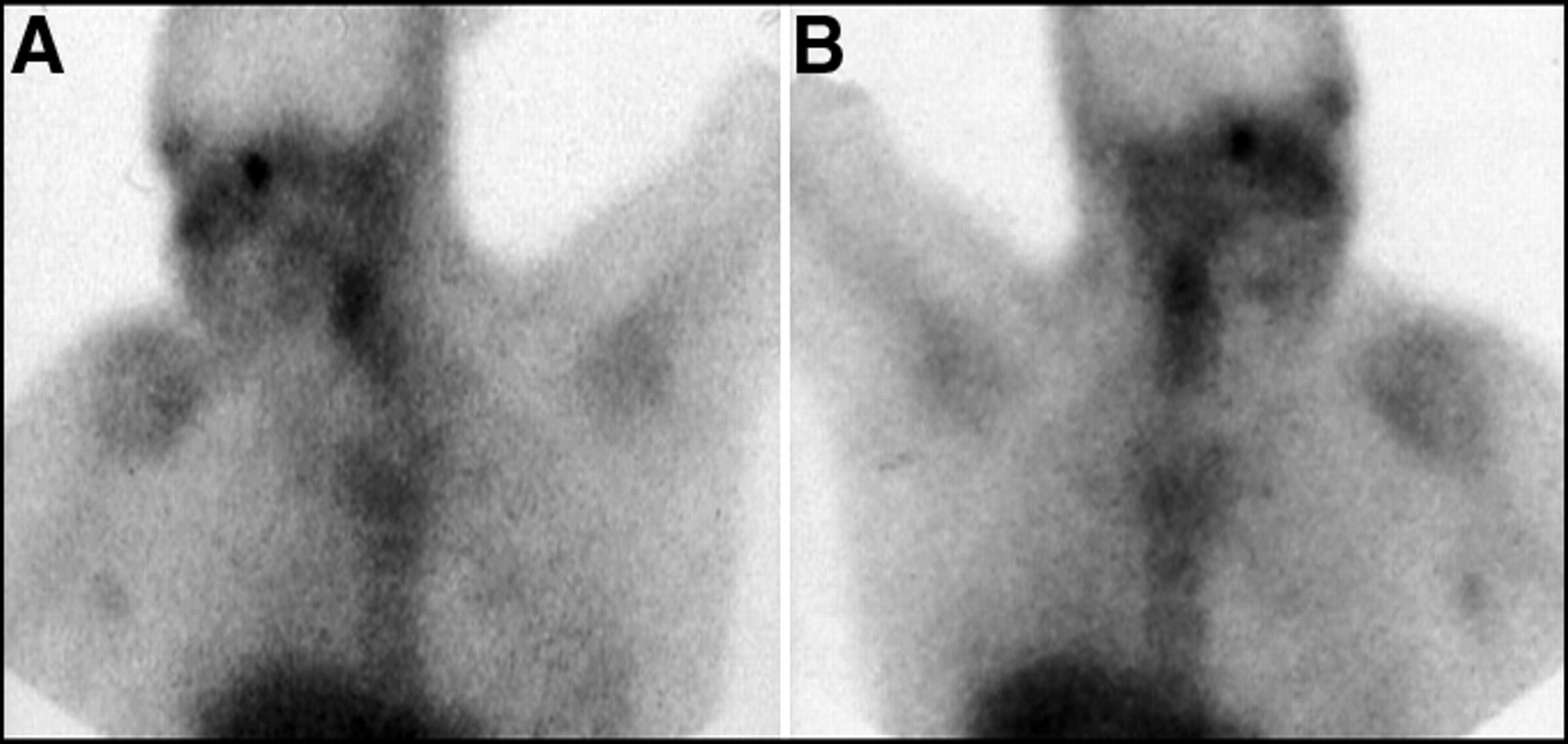
Submental lymph nodes or high cervical lymph nodes containing lymphoma can often be mistaken for salivary gland activity. Shown here, in a patient with a superior mediastinal tumor, is lymphoma in submental lymph nodes seen on both the (A) anterior and (B) lateral planar images.
- FIGURE 6.
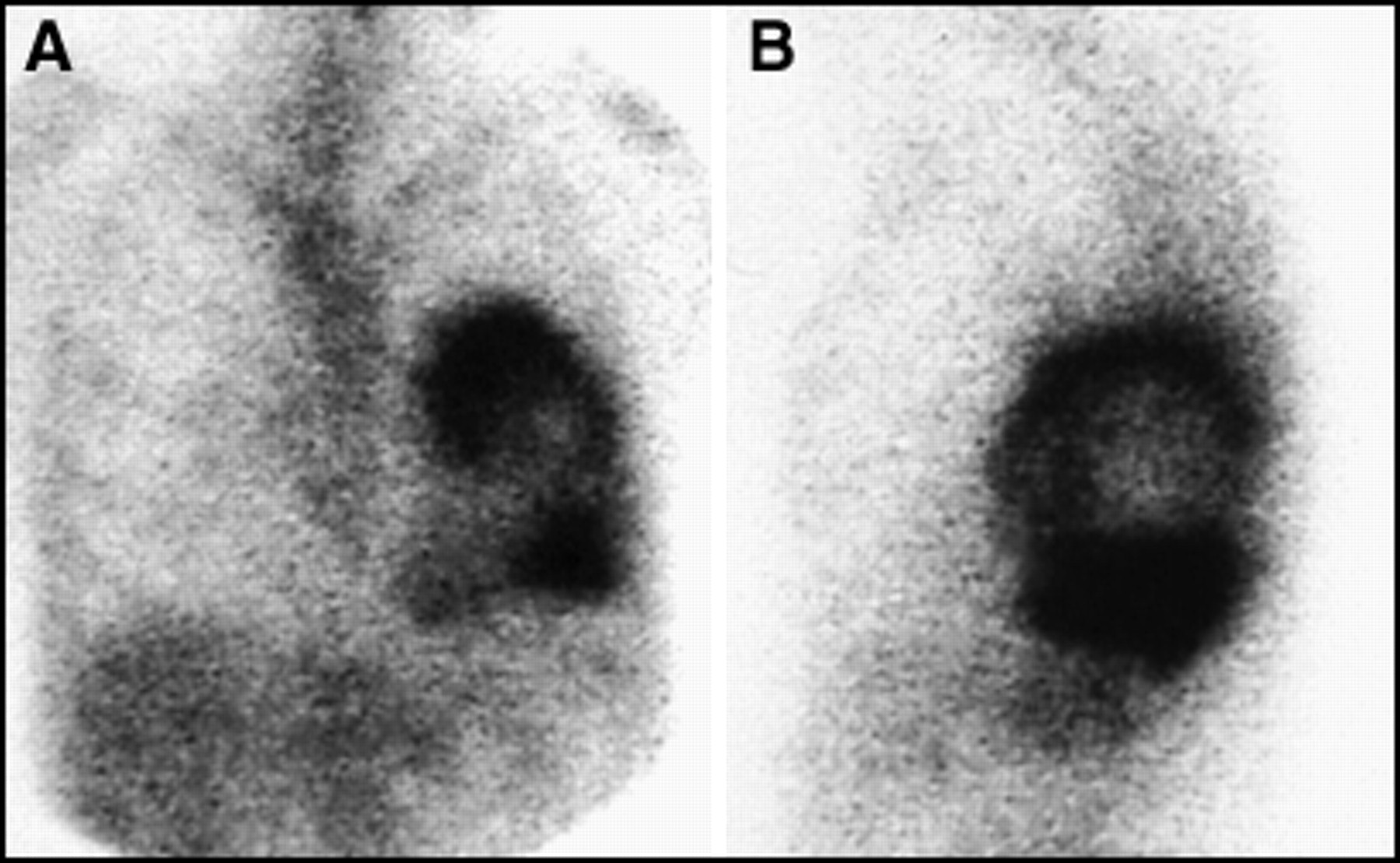
No cardiac activity should be seen on a 67Ga scan. Shown here, in both (A) anterior planar and (B) lateral planar views is activity around the heart, consistent with a malignant effusion of the pericardium.
- FIGURE 7.
(A) A normal 67Ga scan of the chest should reveal no lung uptake. (B) However, mild diffuse activity in the lungs is common and normal after chemotherapy. If activity is intense or the patient is immunocompromised, other inflammatory or infectious conditions should be considered. An example shown here is PCP pneumonia, shown (C) before treatment and (D) after treatment.
- FIGURE 8.
Focal lung uptake should always be regarded as abnormal, but can be from either tumor or infection. Shown here in (A) anterior and (B) lateral planar images is a left lower lobe lung abscess. Note the air:gallium level.
- FIGURE 9.
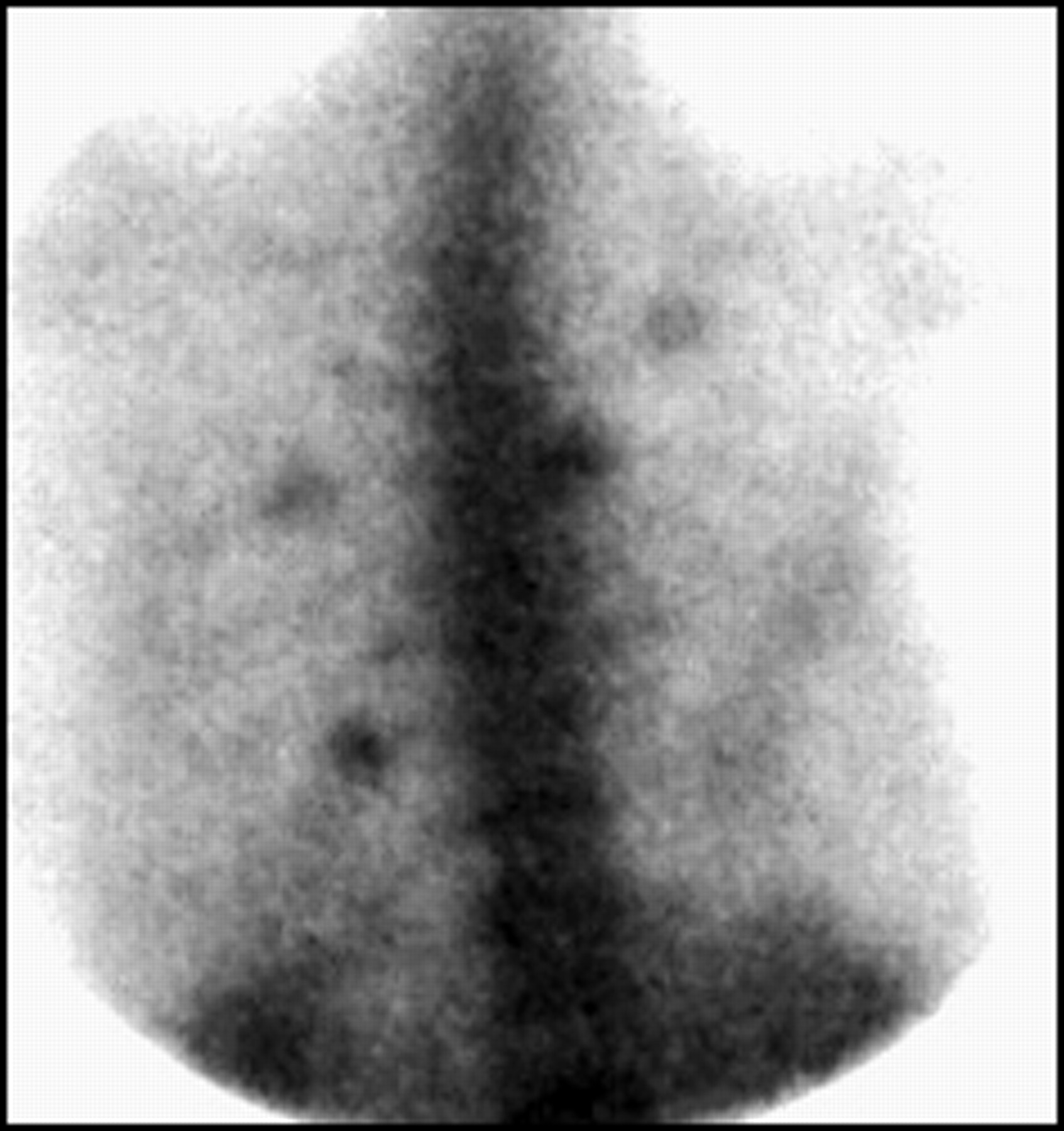
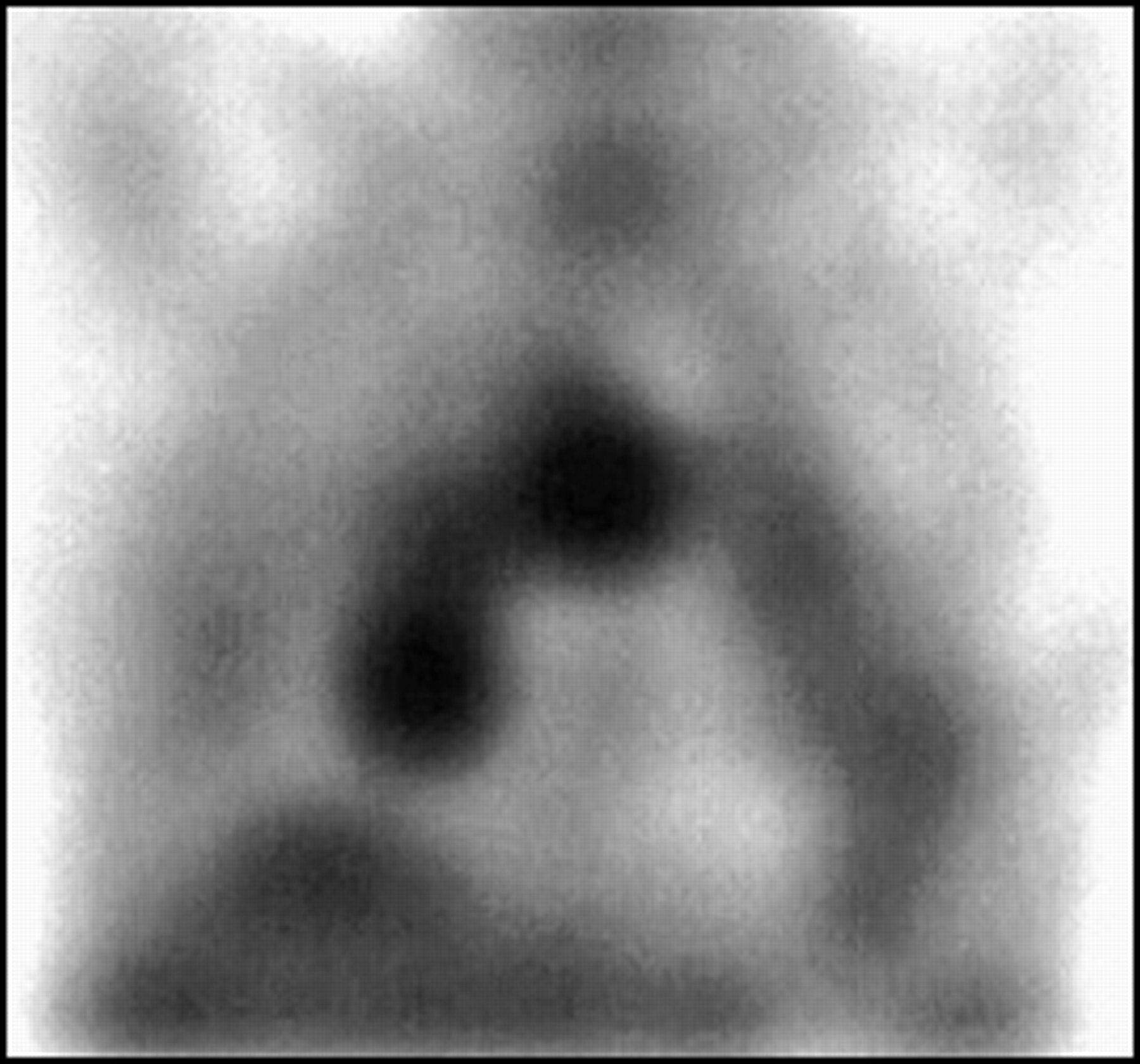
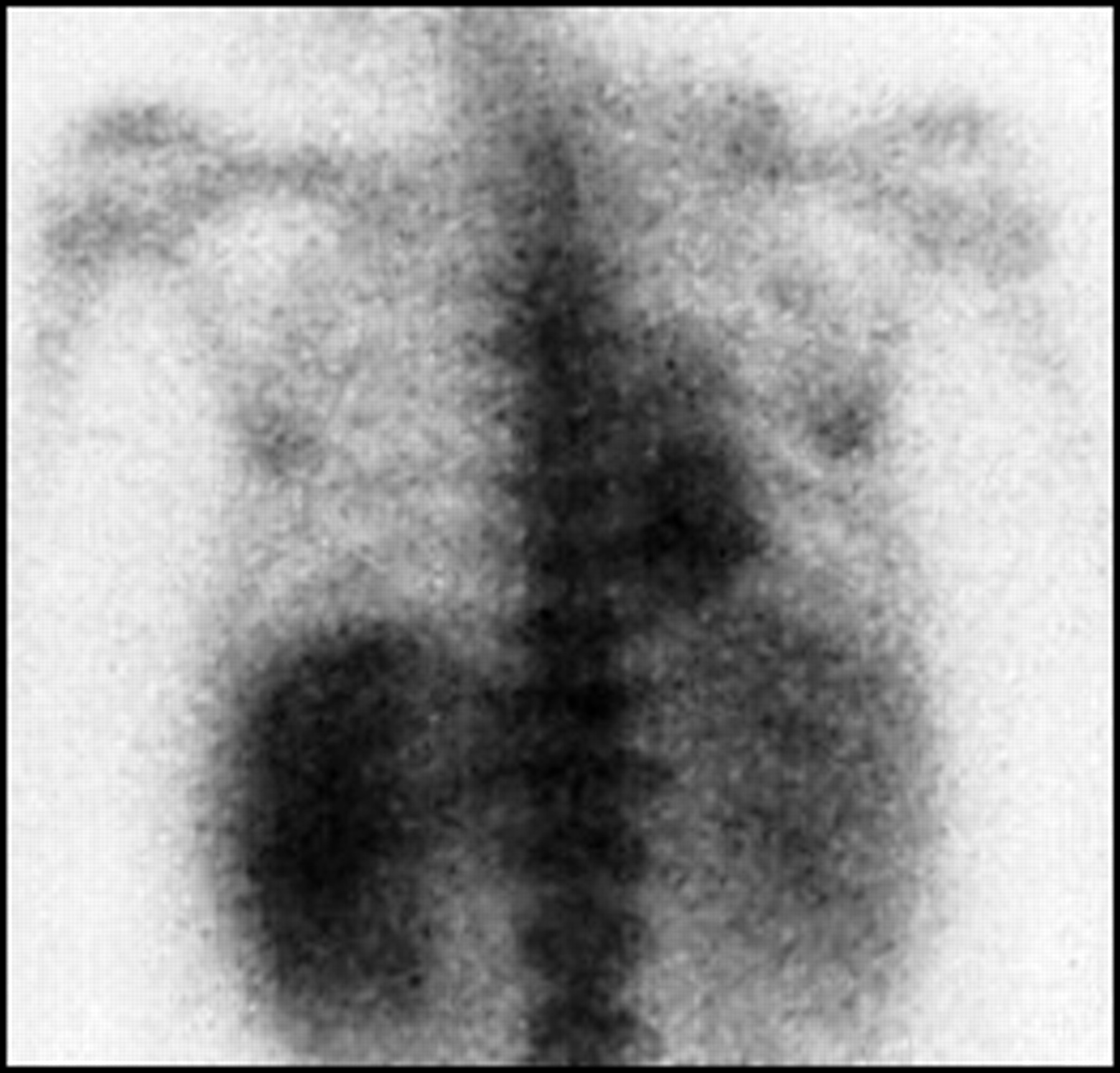
Focal, asymmetrical or intense hilar uptake is consistent with lymphoma, as shown in this coronal SPECT view.
- FIGURE 10.
Normal mild symmetrical hilar uptake can be normal in smokers, or in many patients after chemotherapy and radiation, as shown here in (A) coronal SPECT and (B) planar views. The intensity of uptake on the SPECT views may overestimate the magnitude of uptake and reference to the planar view should always be made.
- FIGURE 11.
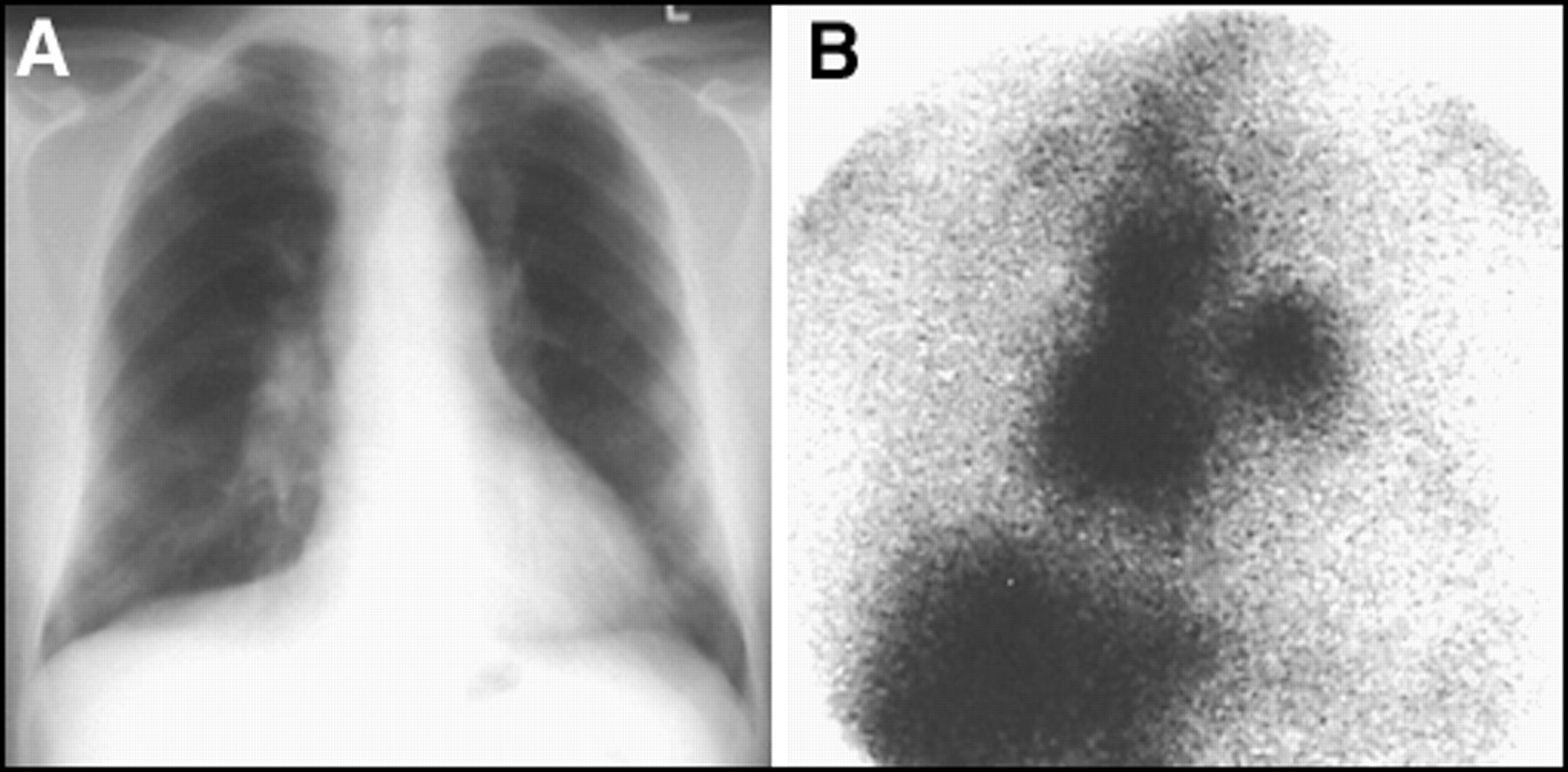
Many diseases may mimic lymphoma, including other tumors and both infectious and noninfectious granulomatous disease. (A) Shown here is a chest radiograph of a patient with hilar and mediastinal fullness, (B) with uptake on 67Ga scan in the same regions. The diagnosis here was sarcoidosis.
- FIGURE 12.
Rebound thymic hyperplasia can occur after chemotherapy in children and young adults and can result in uptake on 67Ga scan in the anterior, superior mediastinum, as shown here in both (A) coronal and (B) sagittal SPECT views. A follow-up scan in 2–3 mo will show regression of activity in “thymic rebound.”
- FIGURE 13.
Mild breast activity can be normal on 67Gan scintigraphy. However, intense breast activity can occur in developing girls after chemotherapy, possibly from hormonal rebound. Shown here is a girl with mediastinal lymphoma (A) before and (B) after chemotherapy. Also note the suppression of activity in the epiphyseal plates after chemotherapy. This is also a common finding.
- FIGURE 14.
Skin folds in the axilla can mimic abnormal lymph nodes. An anterior view of the chest with the arm extended will abolish the finding if activity is due to superimposed tissue from axillary skin folds, shown here for both the (A) right and (B) left axilla.
- FIGURE 15.
(A) Diffuse bowel activity can often compromise interpretation of the 67Ga scan. (B) The typical distribution of activity should be confined to the large intestine. (C) Delayed imaging at 5–7 d postinjection usually will result in clearing of most of the activity from the bowel.
- FIGURE 16.
(A) Activity that is centrally located, and not typical of the distribution of the colon, should be regarded as suspicious for lymphoma. (B) Delayed imaging should result in clearing of normal bowel activity, but not that in the tumor, as is shown in this patient with a large mesenteric nodal mass.
- FIGURE 17.
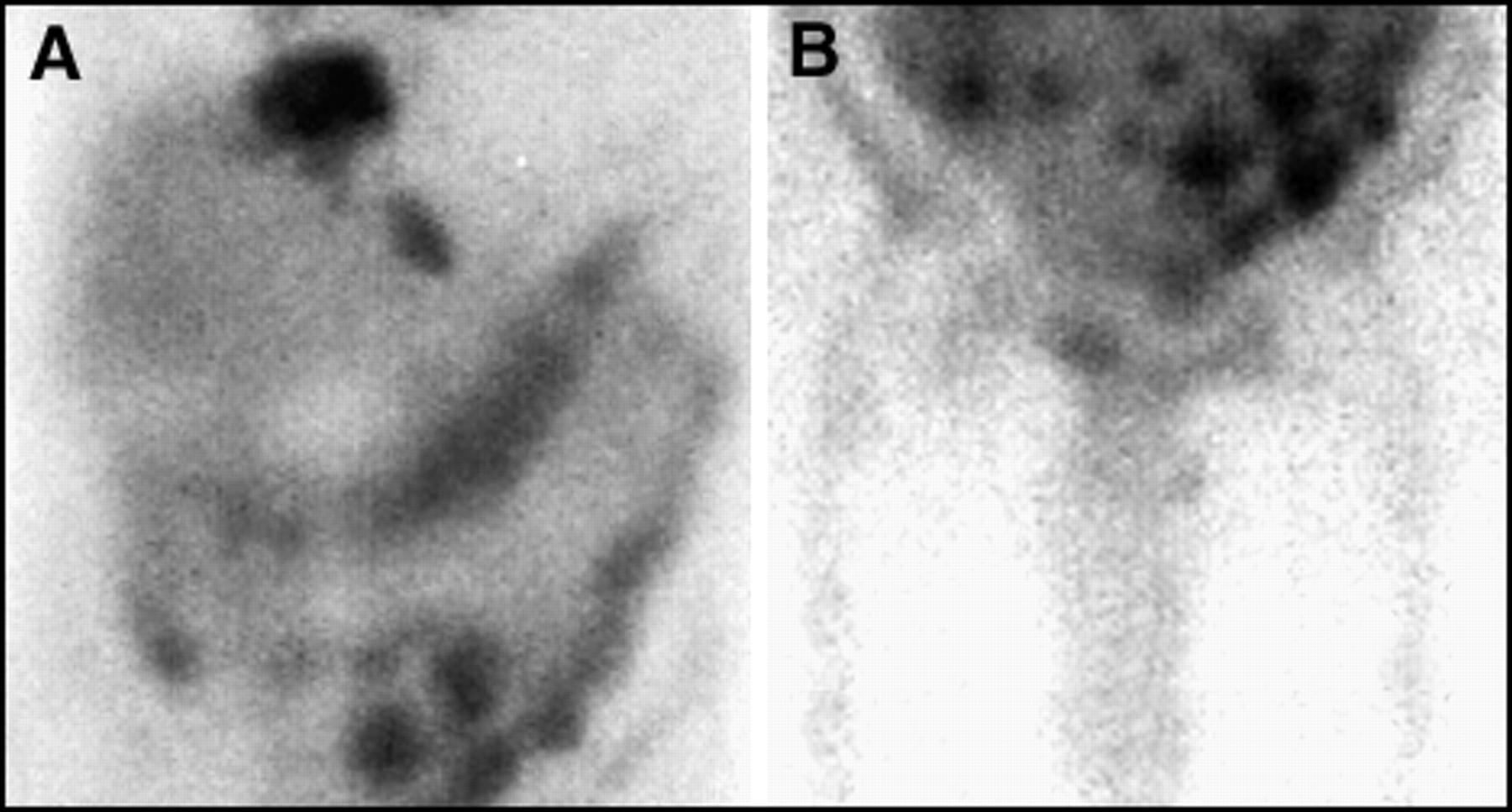
Lymphoma-containing nodes may stud the mesentery, producing focal areas of uptake that are atypical for the appearance of bowel, as is shown in planar views of the (A) upper and (B) lower abdomen in this patient who had multiple areas of tumor.
- FIGURE 18.
Periaortic lymph nodes may be difficult to identify on planar views (A) because they are closely applied to the anterior aspect of the vertebral bodies. (B, C) SPECT imaging in multiple planes may help identify the nodes as being distinct from the vertebrae. It is important to correlate with radiographs to exclude the presence of large anterior osteophytes, which can mimic periaortic lymph nodes.
- FIGURE 19.
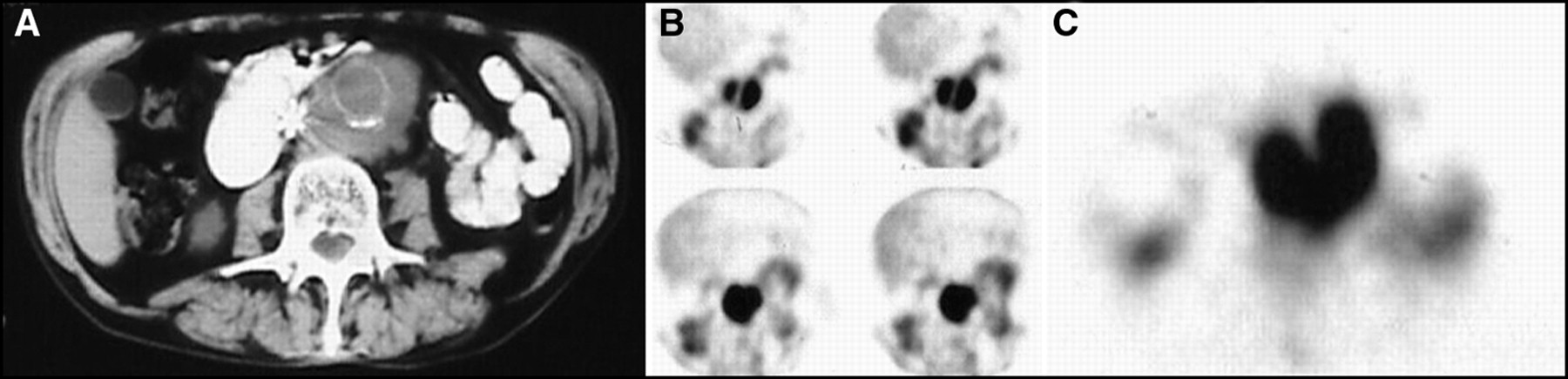
This patient had a vena caval filter and a history of an aortic graft as well as lymphoma. He was asymptomatic and hemodynamically stable. (A) CT scan showed a large periaortic mass, which was 67Ga-avid, as shown on SPECT (B) coronal and (C) transaxial images. The mass was recurrent lymphoma.
- FIGURE 20.
(A) Mild diffuse renal activity is normal after chemotherapy, as in this patient who also had a prior splenectomy. (B) However, if renal activity is intense or there is enlargement of the kidney, as in this coronal SPECT image, lymphoma should be suspected. (C) It is important to ensure that renal activity is not related to pyelonephritis, which can result in uptake on the 67Ga scan.
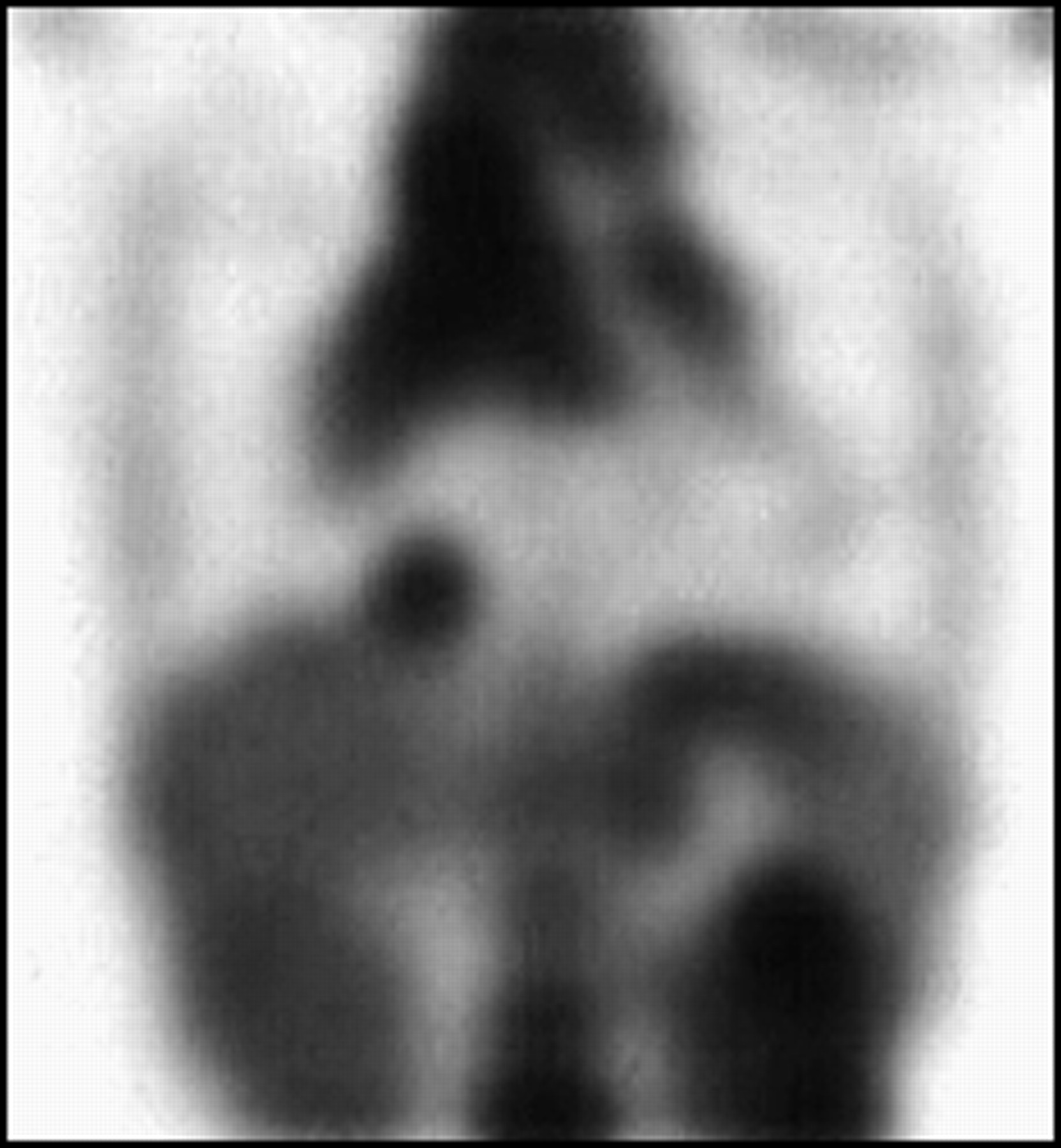
- FIGURE 21.
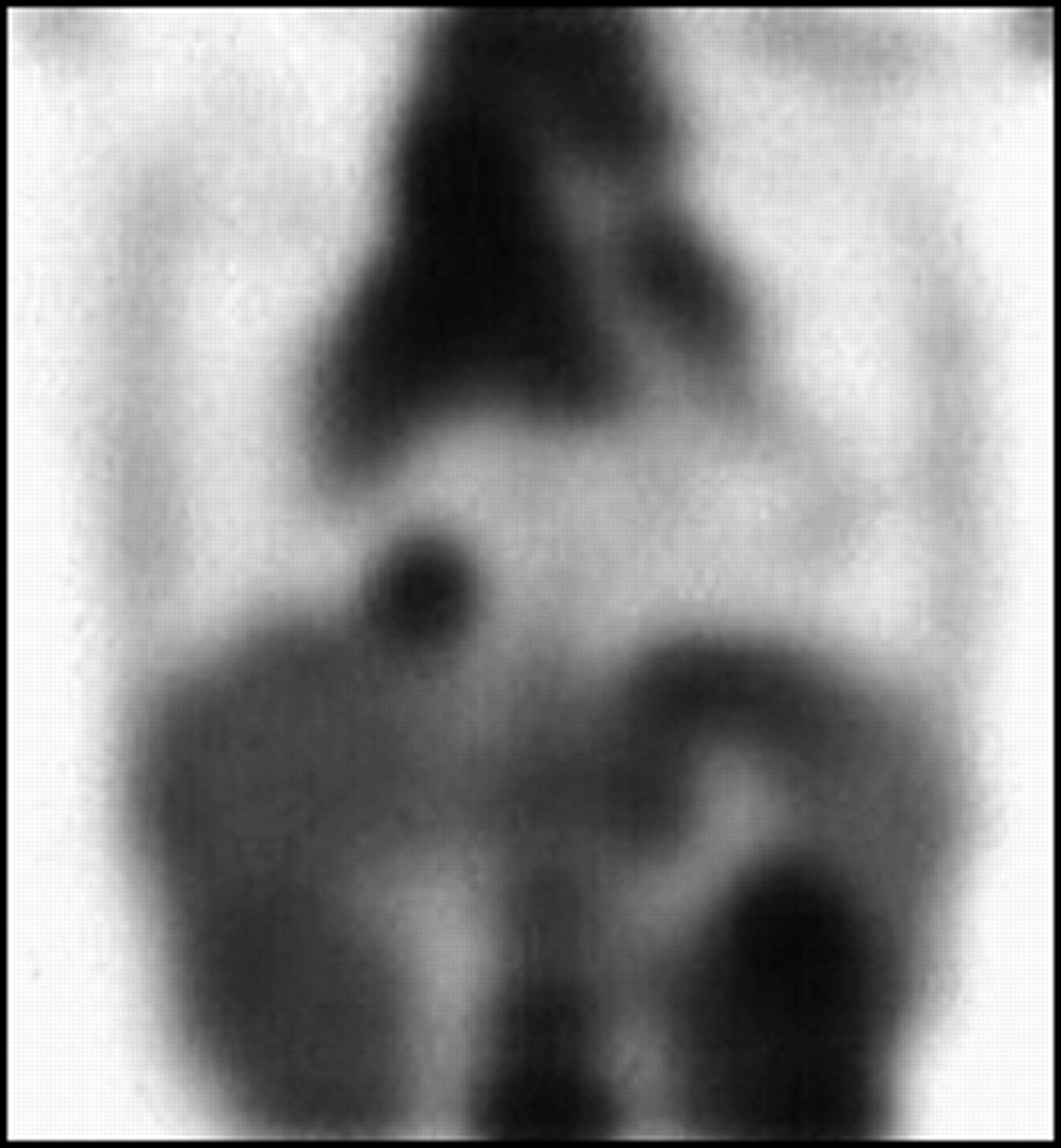
It is often difficult to determine if the spleen and liver are involved with lymphoma because of its typically diffusely infiltrating nature. If the spleen is “hotter” than the liver 3 d postinjection of 67Ga, as shown in this patient who also has mediastinal lymphoma, splenic involvement should be suspected. However, any cause of hypersplenism also can cause increased splenic uptake.
- FIGURE 22.
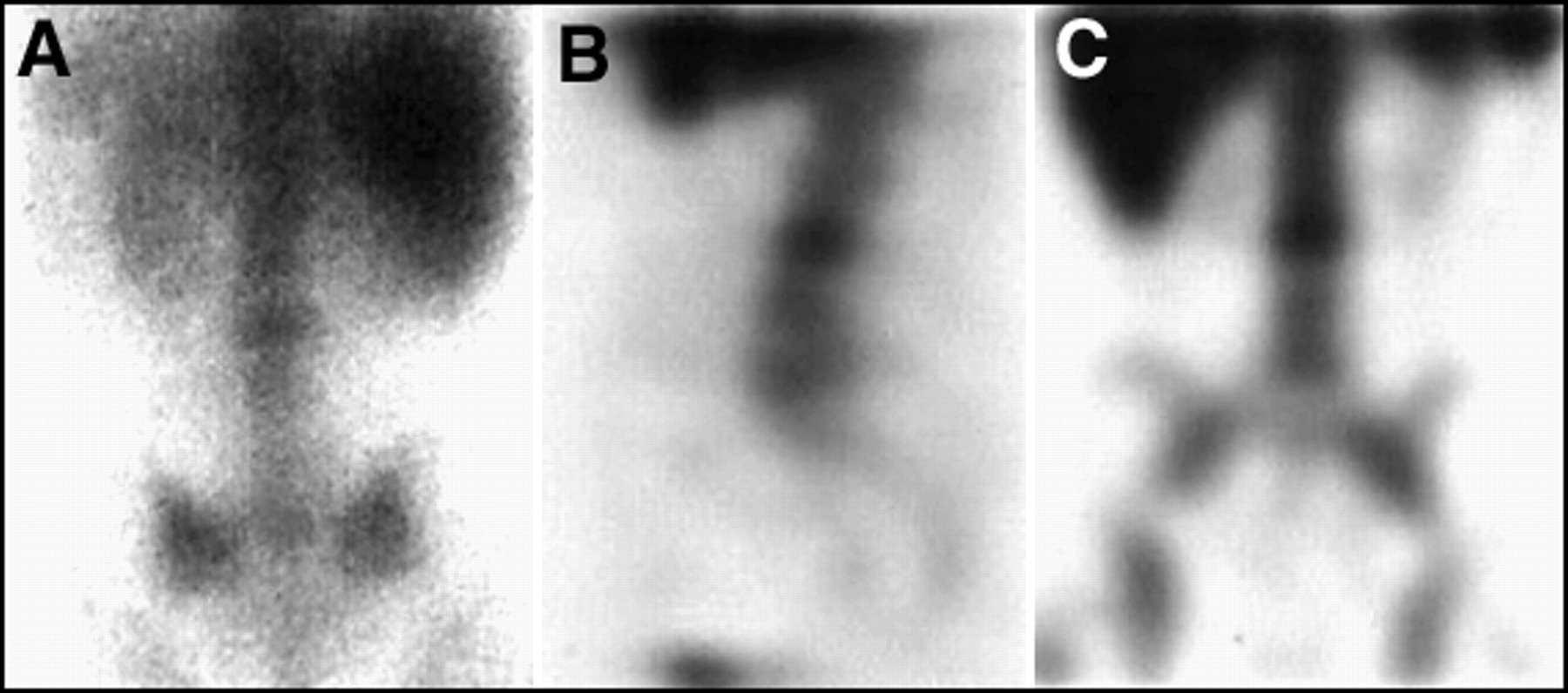
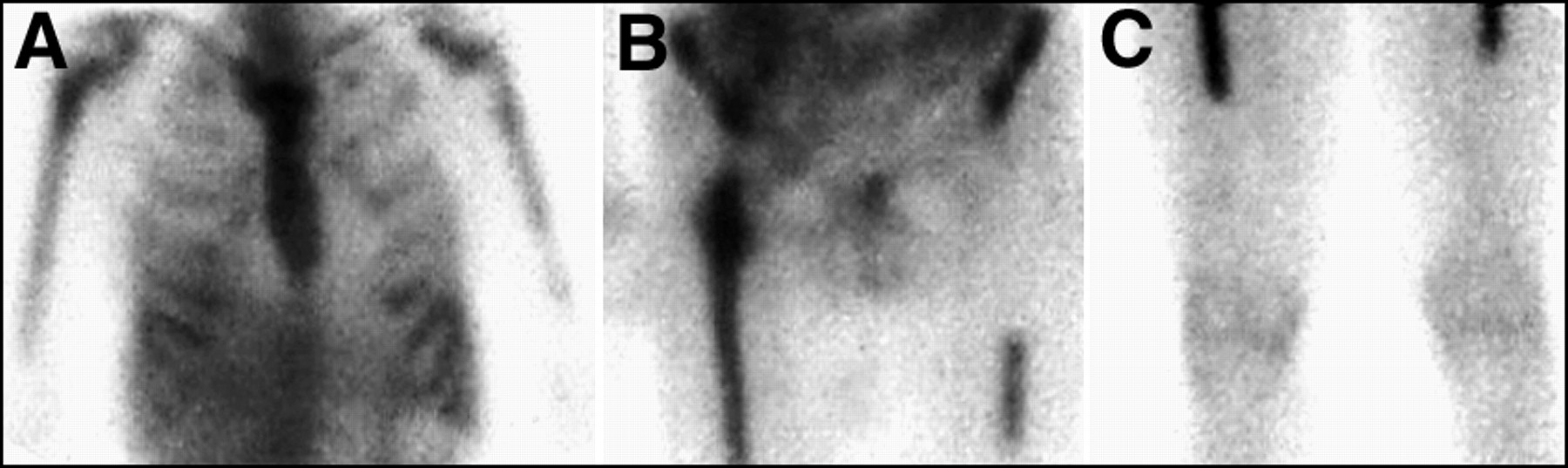
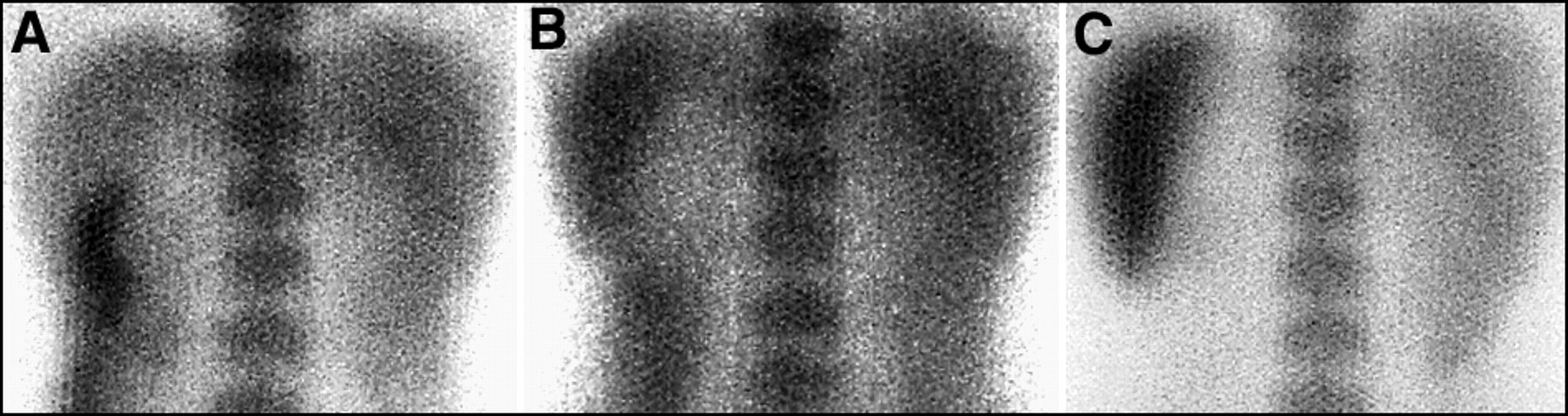
If imaging is extended beyond 3 d postinjection of 67Ga, the spleen normally becomes progressively “hotter” with time, relative to the liver, as shown here at (A) 3, (B) 5, and (C) 7 days postinjection. This is a normal finding.
- FIGURE 23.
Diffuse gastric uptake can be normal after chemotherapy and can be seen in up to 10% of patients. Anterior planar views of the abdomen (A) before and (B) after administration of a carbonated beverage illustrate this finding. Endoscopy is indicated only if the patient is symptomatic.
- FIGURE 24.
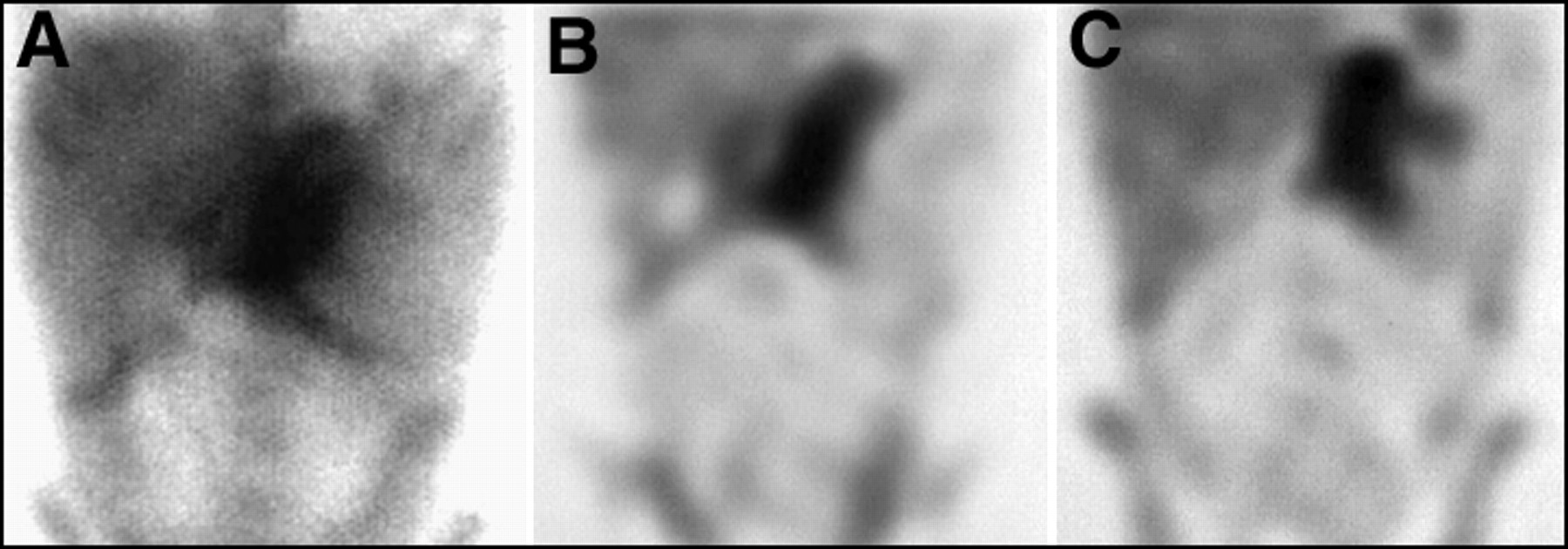
Focal gastric uptake should be regarded as suspicious for lymphoma, as illustrated in this patient with Burkitt's lymphoma of the stomach. Shown here are (A) planar anterior and (B, C) SPECT coronal views of the abdomen with a large 67Ga-avid mass in the stomach region.
- FIGURE 25.
Focal gastric uptake involving cardia of the stomach in a patient with stage IV lymphoma. There is also extensive tumor involving the mediastinum, a right cardiophrenic node, and the kidneys.
- FIGURE 26.
Degenerative arthritis, both of the joints and spine, can result in enhanced uptake of 67Ga, as shown by (A) planar and (B) coronal SPECT imaging of this patient with arthritic changes of the hips and lumbar spine (shown by radiographs).
- FIGURE 27.
The lumbosacral spine can be difficult to evaluate by SPECT. Typical normal patterns may include (A) segmental attenuation of activity by the liver and (B) patchy uptake due to poor counting statistics or obesity.
- FIGURE 28.
Focal abnormal uptake of the lumbosacral spine should be seen both on (A) planar and (B, C) SPECT views, as is demonstrated in this patient with lymphoma involving a midlumbar vertebra.
- FIGURE 29.
Focal rib uptake due to fractures, as seen in this patient, can mimic lymphoma involving the ribs.
- FIGURE 30.
Infection can mimic lymphoma on a 67Ga scan, as is shown in this patient with an osteomyelitis and abscess of the sacroiliac region, due to a prior bone marrow biopsy.
- FIGURE 31.
Lymphoma of the bone often involves the marrow before extending to the bony cortex. (A) 67Ga scan is often more sensitive for detecting lymphoma of the bone than is (B) conventional 99mTc bone scan.
- FIGURE 32.
Diffuse marrow uptake of 67Ga can be seen in patients with diffuse lymphoma of the bone marrow. However, diffuse marrow uptake is a common finding in patients who have previously received chemotherapy that included granulocyte colony stimulating factor (GCSF) or erythropoietin. An example of a patient treated with GCSF is shown here. (A) Planar thoracic, (B) pelvis, and (C) femur views of this patient demonstrate bony activity confined to regions typical of those for red marrow, as illustrated by (C) where activity extends only to the mid-femur. Areas of previous and successfully treated lymphoma involving the skeleton, or areas of prior radiation, will often appear as cold defects, as in (B), where the patient had been irradiated for a large left inguinal mass with associated bony involvement of the left ischium.















Tables
Stage Criteria Stage I Single lymph node region or extra-lymphatic site Stage II ≥2 lymph node regions on same side of diaphragm Stage III Lymph node regions on both sides of diaphragm Stage IV Disseminated disease >1 extra-lymphatic organ ± lymph node involvement Substages: A Asymptomatic B Fever, night sweats, ≥10% weight loss - TABLE 2.
Predictive Value of a Gallium-67 Scan After Therapy: Survival at 24 Mo Post-Therapy*
Lymphoma type 67Ga scan results Survival at 24 mo after therapy No lymphoma Total survival** Hodgkins Negative 85–95% 100% Hodgkins Positive ≤45% 60–80% Non-Hodgkins Negative 85–95% 90% Non-Hodgkins Positive ≤50% 35% * Assuming a pretherapy 67Ga scan demonstrated gallium-avid tumor.
↵** With or without evidence of lymphoma.
Adult activity: 8–10 mCi Pediatric activity: 75 uCi/kg Total body planar images 3 days postinjection SPECT chest/neck 3 days postinjection Repeat planar and SPECT abdomen 5–7+ days postinjection Medium- or high-energy collimator 3 photo peaks (93, 185, 300)—20% windows 512 matrix 10-min images Upright AP/Post/Lat chest ≥1000 K counts if no SPECT 128 matrix For 2 heads: 3-degree stops × 60 (180 degrees each) 35 s per stop (35 min total) Increase time to 40 s/stop for delayed (>3 d) SPECT RAMP type filter 3-D postfilter, low-pass (Butterworth), order of 6, adjust cut-off to adjust image presentation Software attentuation correction Display transaxial, sagittal, and coronal images Slice thickness: 14 mm (3 pixel)/slice Adjust intensity to be within linear range of contrast curve ↵* Example provided for dual-head SPECT camera.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.