


Abstract
Objectives:A mass casualty disaster drill involving the simulated explosion of a radiation dispersal device (dirty bomb) was performed with the participation of multiple hospitals, emergency responders, and governmental agencies. The exercise was designed to stress trauma service capacities, communications, safety, and logistic functions. We report our experience and critique of the planning, training, and execution of the exercise, with special attention to the integrated response of the Departments of Nuclear Medicine, Health Physics, and Emergency Medicine.
Methods:The Health Physics Department presented multiple training sessions to the Emergency Medicine Department, Operating Room, and ancillary staff; reviewing basics of radiation biology and risk, protection standards, and detection of radiocontamination. Competency-based simulations using Geiger–Müller detectors and sealed sources were performed. Two nuclear medicine technologists played an important role in radiation discrimination—that is, assessment of radioactive contamination with survey meters and radionuclide identification based on γ-spectroscopy of wipe smears from patients’ clothing, skin, and orifices. Three Health Physics personnel and one senior Nuclear Medicine staff member were designated the radiation control officers for assigned teams triaging or treating patients. Patients were triaged and, when indicated, decontaminated.
Results:Within a 2-h period, 21 simulated victims arrived at our institution’s Emergency Room. Of these, 11 were randomized as noncontaminated, with 10 as contaminated. Decontamination procedures were implemented in a hazardous materials (HAZMAT) decontamination trailer and, for the 5 patients with simulated serious injuries, in a designated trauma room. A full debriefing took place at the conclusion of the exercise. Staff largely complied with appropriate radiation protection protocols, although decontamination areas were not effectively controlled. The encountered limitations included significant lapses in communications and logistics, lack of coordination in the flow of patients through the HAZMAT trailer, insufficient staff to treat acute patients in a radiation control area, additional personnel needed for transport, and insufficient radiation safety personnel to control each decontamination room.
Conclusion:Nuclear Medicine personnel are particularly well qualified to assist Health Physics and Emergency Medicine personnel in the preparation for, and management of, mass casualty radiation emergencies. Simulation exercises, though resource intensive, are essential to an institution’s determination of response capability, performance, and coordination with outside agencies.
Much of the medical literature on radiation accidents focuses on incidents involving relatively small numbers of individuals injured or contaminated after nuclear power plant or transportation accidents (1,2). More recently, various agencies and health care providers have reported response plans for acts of terrorism, which may involve casualties from chemical, biologic, and radiologic weapons (3–5). The Council of Boston Teaching Hospitals participated in a multiagency exercise involving the simulated detonation of a 60Co radiation dispersal device (dirty bomb) on an airport tarmac, resulting in mass casualties complicated by radiation contamination. The scenario required on-site responders to acknowledge the presence of radiation, set up control zones, implement contamination control measures, institute personnel monitoring, communicate radiologic conditions, and demonstrate mass casualty processing of contaminated patients. This simulated exercise involved members of the Federal Aviation Agency, Emergency Medical System, Fire and Police Departments, Centers for Disease Control and Prevention, Federal Bureau of Investigation, and several hospitals throughout Boston. The exercise was also designed to “stress” Emergency Department (ED) and Operating Room capacities, communications, safety, and logistic support functions. Approximately 120 simulated victims were recruited from area educational institutions to present at various hospitals—some as ambulatory “worried well” and others with simulated wounds with or without radiocontamination. The simulation did not include actual radioactive sources. This article expands on the integrated efforts of the Departments of Health Physics, Emergency Medicine, and Nuclear Medicine in the planning, training, and execution of a mass casualty radiation exercise. Limitations and improvement needs are also reported.
MATERIALS AND METHODS
Training and Roles: Medical and Ancillary Staff
A cadre of environmental safety officers, ED nurses, and physicians had previously completed hazardous materials (HAZMAT) training and were thus familiar with chemical and biologic decontamination procedures. Competency-based HAZMAT training requirements are codified in 29 CFR 1910.120 and available from the Occupational Safety and Health Administration (6). At each participating hospital, decontamination staff underwent a minimum of 8 h of hazardous materials training, which is the minimal requirement for first responders. Health Physics personnel, supervising the radiation detection and decontamination, had not yet completed chemical and biologic hazard training, though a mixed hazard scenario compels all members of the response team to undergo training and competency assessments.
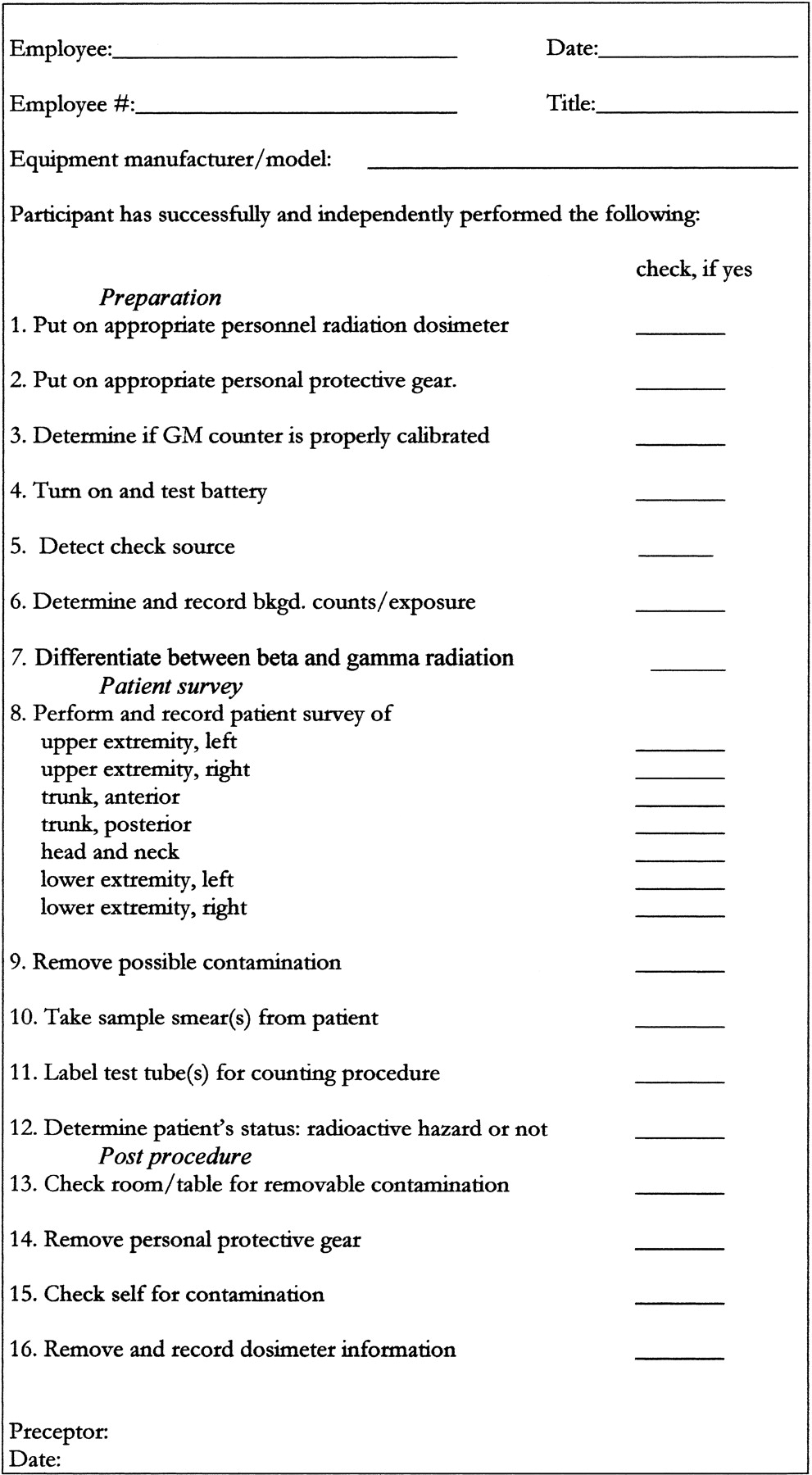
The diverse backgrounds of the participants determined the radiation protection training needs. In fact, several of the trainees were familiar with pocket dosimeters and decontamination procedures from prior military service. Under the direction of the Health Physics Department, multiple training sessions were presented to the ED, Operating Room, and ancillary staff, reviewing basics of radiation biology and risk, radiation protection standards, and detection of radiocontamination. Staff also reviewed publicly available materials on radiation disaster management prepared by both the American College of Radiology and the U.S. Military (7,8). “Hands-on” simulations using Geiger–Müller (GM) detectors, sealed sources, and manikins were performed. The simulations included a GM survey competency assessment using β- and γ-emitters (Fig. 1). Training modules from the Radiation Emergency Assistance Training Site of the Oak Ridge Associated Universities were also used (9).
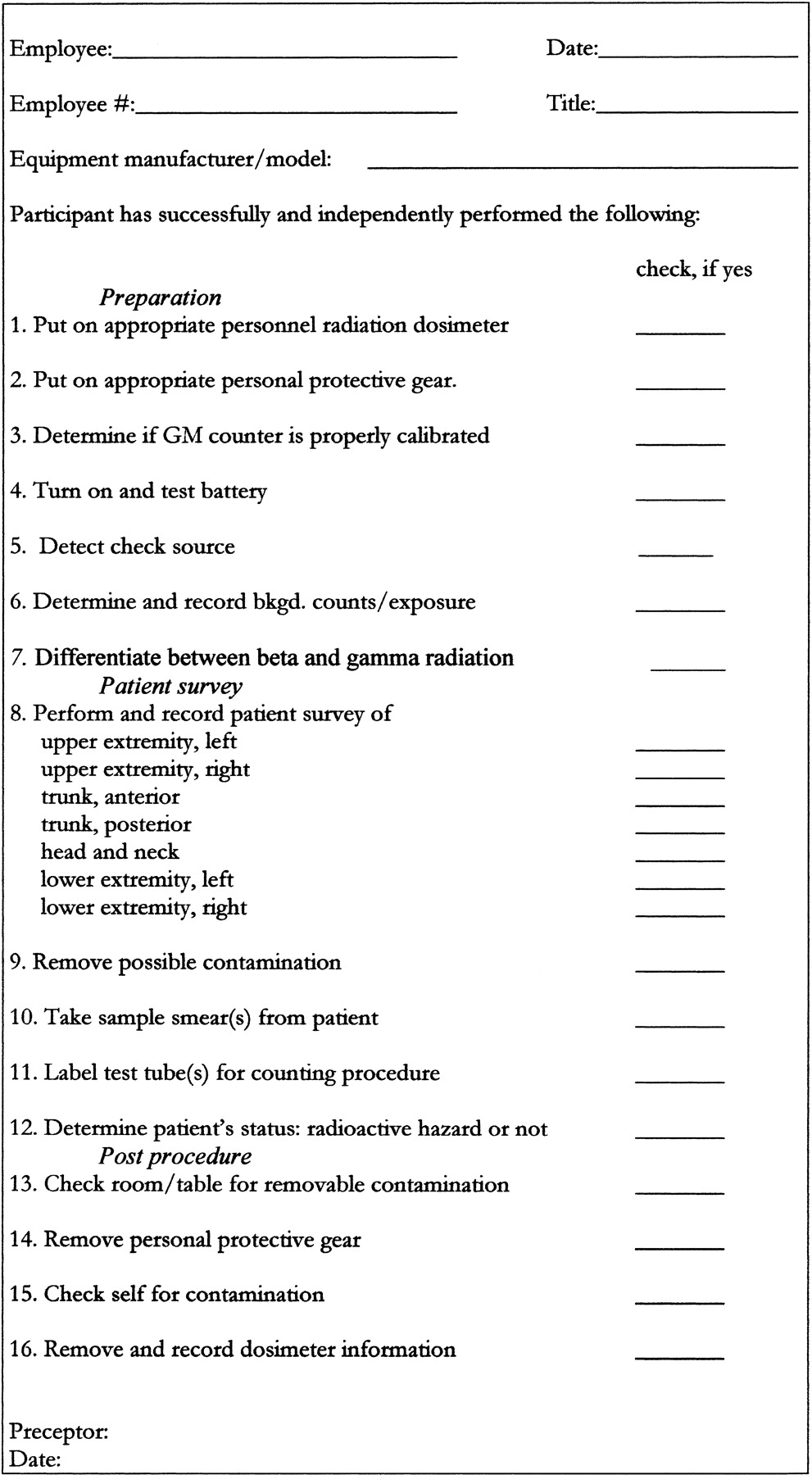
Radiation Detection/Decontamination Competency Assessment Form. bkgd. = background.
Training and Roles: Nuclear Medicine Staff
Members of the Health Physics Department provided tutorials on radiation hazards, counting methods, decontamination protocols, and triage procedures to the Nuclear Medicine technical staff. Staff also demonstrated GM detector competencies. A γ-well counter (Cobra II; Packard Instrument Co. Inc.) was programmed to count wipe smears from patients’ clothing, skin, and orifices as well as blood and urine samples. The detector is capable of resolving γ-emissions from 0.015 to 2.00 MeV. Two nuclear medicine technologists were assigned responsibility to accept and process samples, interpret and report spectroscopy results, and hold samples for additional forensic investigations. A senior nuclear medicine staff member conferred with Health Physics personnel, in preparation for functioning as the radiation safety leader within the trauma suite—monitoring patients and personnel and directing decontamination procedures.
Supervision/Communications
Disaster management was directed by a Hospital Emergency Incident Command System (HEICS), based on the Incident Command System (ICS) model, found in NCRP 138 (10). The Incident Commander had also received the same tutorials and training as the response team. The HEICS assigned and provided specific job action sheets, flow of command, reporting duties, and communications for key functions such as logistics, safety, and treatment areas. The HEICS was also responsible for communicating with the media and external agencies. At our institution, HEICS operates from a command center equipped with emergency power generators, dedicated computers, telecommunications equipment, and assigned scribes, functioning as backup to electronic systems in the event of telecommunication system failures.
Security
In mass casualty disasters, many uninjured persons may transport themselves to the hospital with unfounded concerns of exposure or injury, thus inundating emergency rooms and potentially causing widespread contamination within the hospital setting. The Security Department reviewed procedures to maintain access and control to the designated areas and practiced job tasks while wearing personal protection equipment. Members of the Security Department were well-versed in “lockdown” procedures that protect the facility from unwanted incursions, though were less evident or effective in securing radiation control lines within the trauma areas. Subsequent drills have addressed this shortcoming.
Triage
For triage purposes, mass casualty patients fall into 1 of 4 distinct color-coded categories:
III Green: Nonurgent, no ambulance or prehospital treatment required
II Yellow: Injured, though not gravely, can be put in holding area
I Red: Urgent, life support or immediate intervention indicated
0 Black: Impending death, reserve resources for other patients
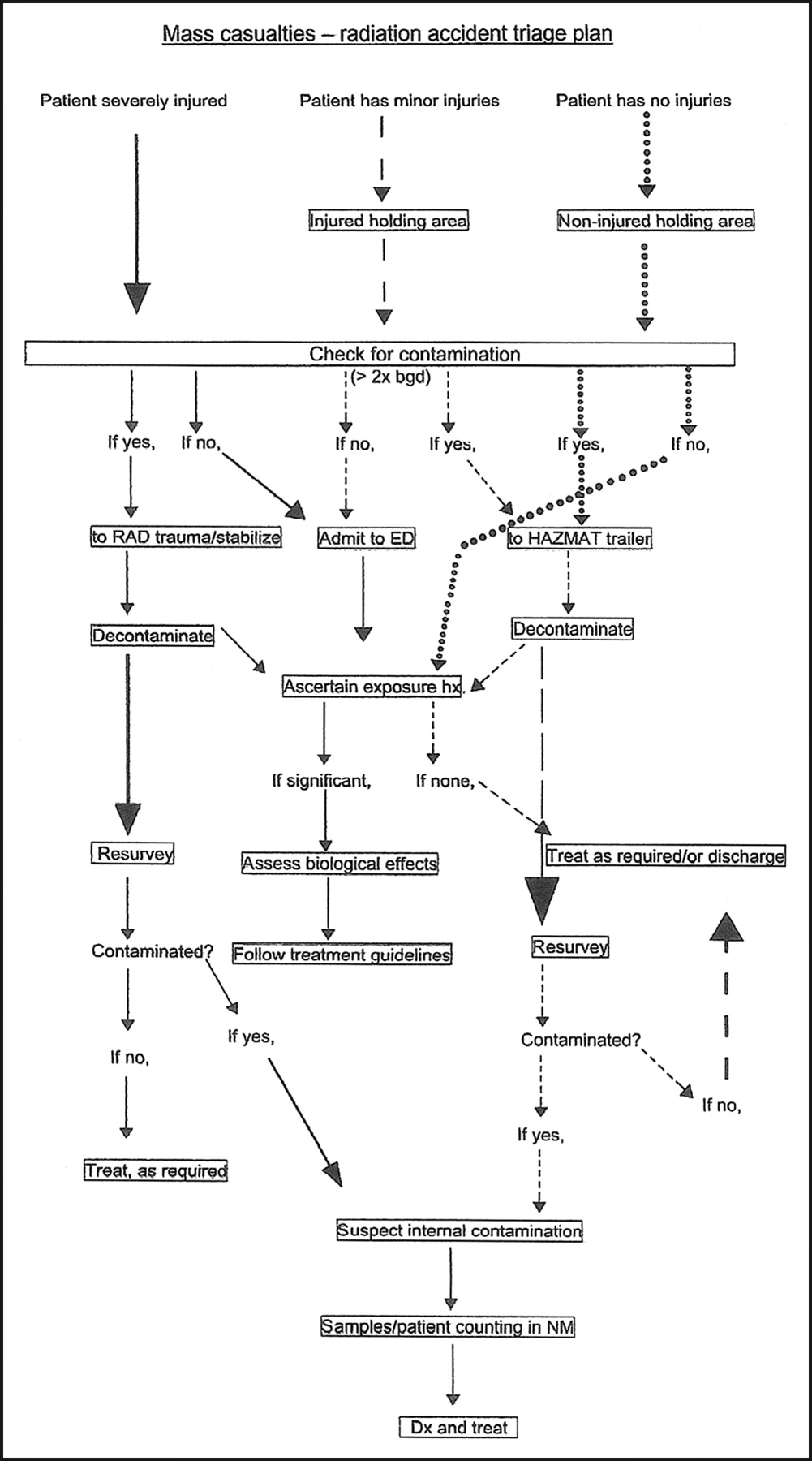
A flow chart, decontamination plan, and treatment admission scheme were established for levels I–III (Fig. 2). Triage areas included a primary station in the ambulance bay; a hazardous materials (HAZMAT) decontamination trailer; a radiation control area/trauma suite; and a holding area for nonacute, uncontaminated patients (Figs. 3 and 4). Four senior Nuclear Medicine and Health Physics staff members were designated as radiation control officers to each team triaging or treating patients. This was reassuring to novice users of radiation detection equipment and provided expertise (interpretation of exposure values, radiation control line integrity, assignment of safe time limits) at each site.
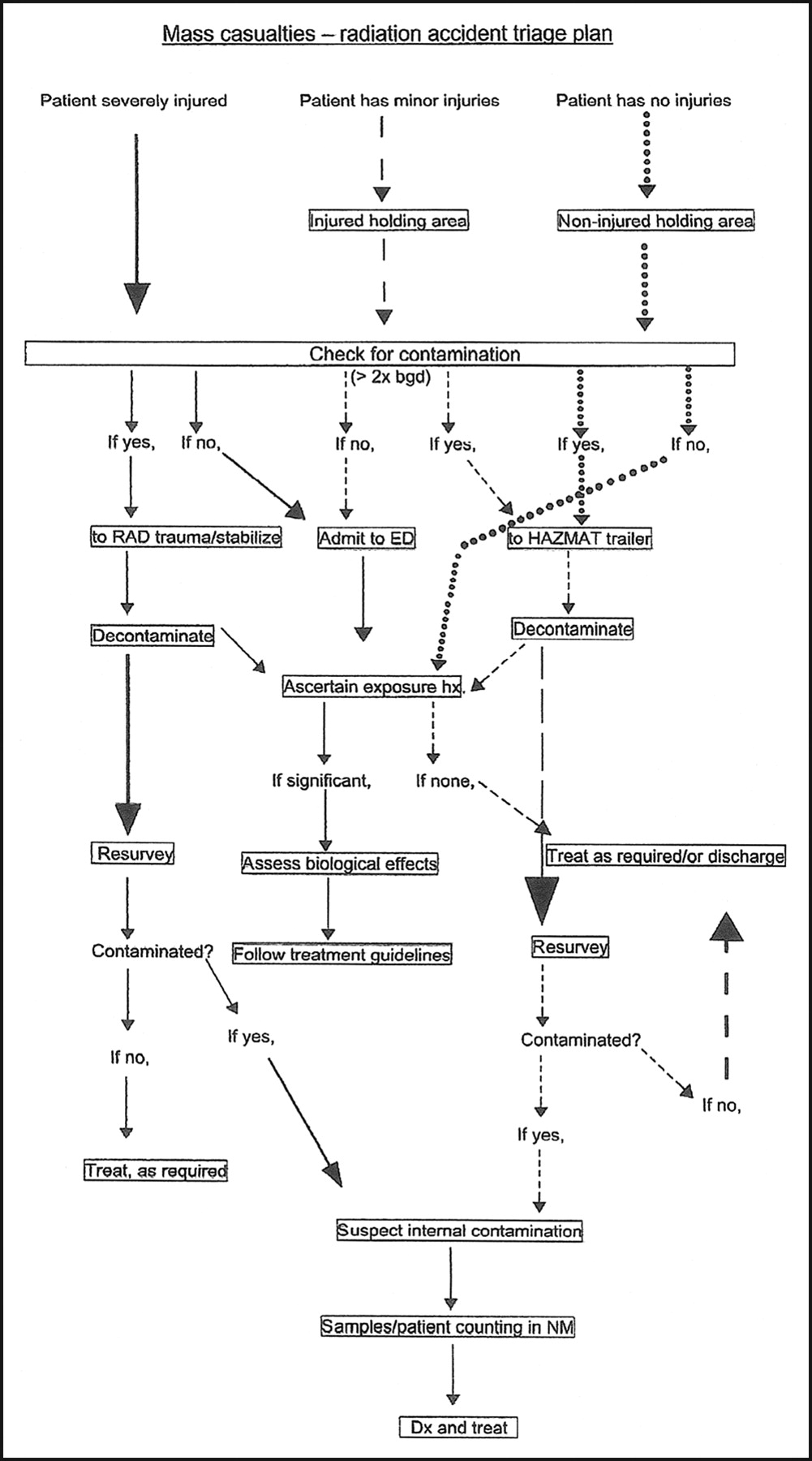
Decontamination and triage algorithm for processing of mass casualty victims. bgd = background; RAD = radiation control area; hx = history; NM = nuclear medicine; Dx = diagnose.

Emergency room receiving and triage entrance, protected against radiation contaminants.

One of 2 rooms within the decontamination (HAZMAT) trailer.
Personal Protection or Decontamination Procedures
By definition, personal protection equipment varies by classification levels A–D (11). Level A requirements are the most stringent and include a self-contained breathing apparatus (SCBA), fully encapsulated suit, and chemical-resistant boots and gloves. Level B offers the same level of respiratory protection but less skin protection. Level C is used when air concentrations are much lower and does not require a SCBA or encapsulated suit. Level D calls for coveralls and safety goggles, which can be used when there is no known chemical hazard. Chemical protection suits vary widely in their effectiveness, ease of use, and durability (12). The suggested HAZMAT response for each facility required (a) the ability to decontaminate at least 8–10 patients per hour, (b) availability of multiple warm water showerheads, and (c) level C protection for the participating staff members. At our institution, impermeable chemical suits, surgical masks, face shields, double latex gloves, and shoe covers were worn by all decontamination, triage, and trauma team members.
Plastic sheets covering flooring and equipment, radiation signs, and demarcation ropes were positioned, and mobile lead containers for shrapnel or material evidence were placed in the trauma and decontamination areas. Ion chambers (Inovision 451P; MicroVision, Ltd.) and GM detectors (Ludlum model 3) were distributed to triage and treatment stations, as were standard optically stimulated luminescence dosimeters (Landauer, Inc.) as well as rechargeable pocket ion chamber dosimeters (Biodex, Inc.).
Nishiyama et al. described their experience in detecting and quantifying in vivo contamination with uncollimated γ-cameras (13). Using point sources, the authors determined minimal detection activities for radionuclides emitting γ-energies between 0.035 and 1.30 MeV. Although this approach is helpful in determining organ and whole-body exposures, our immediate goals were simply to locate, identify, and remove external contamination before surgical or other treatments and to devise ad hoc protection plans (e.g., time–distance requirements for staff) for each patient with internal or nonremovable external contaminants. For this purpose, we used the ion chambers (operating range, 5 μSv/h to 50 mSv/h for γ-rays > 0.025 MeV) and GM detectors with efficiencies ranging from 7% (for 137Cs) and 9% (for 131I and 60Co) to 13% (for 32P).
An acceptable background radiation level under these circumstances was established at 0.5 μSv/h (0.05 mR/h). The original protocol previously mandated decontamination of patients to within 2× background, an impractical value in a crowded space with multiple sources of radioactivity. We have since adjusted that limit to 5× background, equaling 2.5 μSv/h (0.25 mR/h). For personnel, a threshold effective dose of 3.75 mSv (375 mrem), the ALARA II (as low as reasonably achievable) quarterly whole-body exposure value for occupationally exposed individuals at our institution, was targeted as a limit for hospital personnel. The National Commission on Radiation Protection and Measurements (NCRP) offers wider discretion, stating, “Normally, only actions involving life saving justify acute exposures that are significantly in excess of the annual effective dose limit…. Exposures during emergency operations that do not involve life saving should, to the extent possible, be controlled to the occupational dose limits. Where this cannot be accomplished, it is recommended that a limit of 0.5 Sv effective dose and an equivalent dose of 5 Sv to the skin be applied, which is consistent with ICRP recommendations.” (14). Clearly, there is a great difference between our conservative target (0.00375 Sv), the annual permissible (United States) occupational dose limit (0.05 Sv), and a “life-saving” limit of 0.5 Sv, suggesting that individual institutions may vary in setting their safe threshold for emergency procedures. No pregnant personnel were permitted to take part in the initial triage of patients or the decontamination and treatment of radiocontaminated patients.
RESULTS
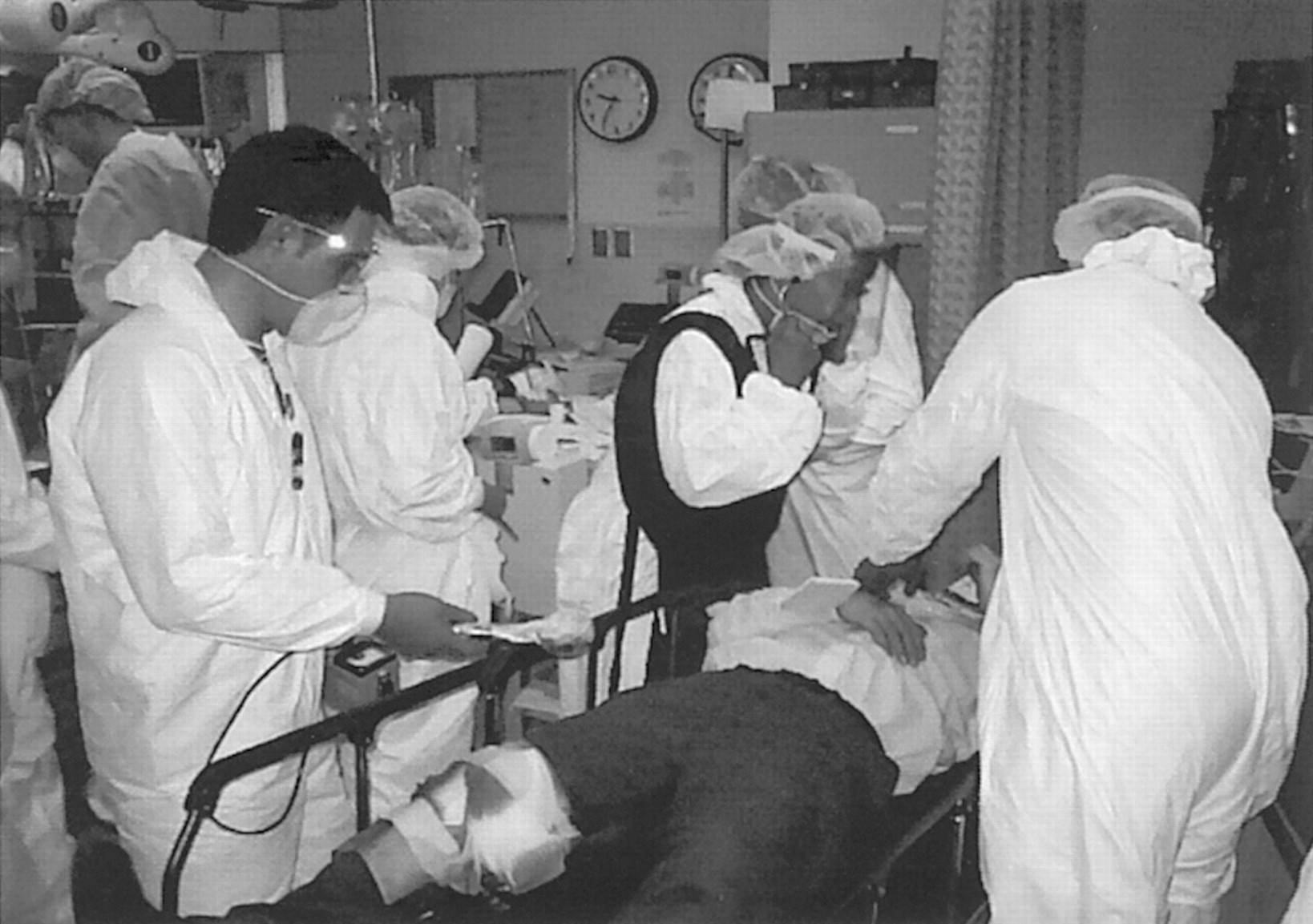
Within a 2-h period, 21 simulated victims presented to our institution’s Emergency Room. Eleven patients were randomized as noncontaminated and 10 as contaminated. Results of body surveys (before and after decontamination) were recorded on a standardized form that accompanied the patient. Five of the radiocontaminated patients were brought to the HAZMAT trailer for decontamination procedures. This rapid influx of patients quickly exceeded the throughput capacity of the HAZMAT trailer, as this involved (for each patient) transport up a steep ramp into the trailer, removal of personal effects and clothing, transfer to the decontamination table, thorough decontamination and resurvey, and transport down a steep ramp. The 5 patients with simulated serious injuries were consecutively decontaminated and stabilized in the trauma suite (Fig. 5). We experienced numerous breaches of the radiation control line, principally by staff attempting to participate in patient resuscitations and other critical care activities. An exercise participant, playing the role of a member of the media, also easily infiltrated the triage area, simply by wearing a labo-ratory coat. The Security Department could have played an increased role here and will work more closely with the response team in the future. It was also difficult for a single radiation safety officer to monitor and communicate survey findings while also directing decontamination and radiation protection measures within the trauma suite. Cellular phones and pagers did not work at all locations and were difficult to operate during decontamination procedures, thus necessitating the need for “runners.” Radio headsets would have been ideal.

Radiation control and treatment of patients within the designated trauma room.
DISCUSSION
Emergency rooms fully engaged with multiple trauma cases are often chaotic and noisy. Within that setting, identifying and communicating with staff wearing chemical protective suits further complicates operations. Color-coded vests or large identification tags (function specific—e.g., Anesthesiology, Respiratory Therapy, X-ray, etc.) would be helpful. We found we were critically understaffed in triage and treatment areas, requiring additional personnel to function as runners—transporting documents, supplies, patient tissue samples, and patients themselves. At least 3 additional radiation safety personnel were needed to assist in the treatment areas, and an additional 2 would have been required to accompany and monitor surgical teams during intraoperative removal of radioactive shrapnel or tissues.
As an added stressor, 90 min into the drill only some of the staff were informed that 131I had also been found at the bomb site. The implications of this were not fully understood by the team leader and thus were not communicated to Health Physics personnel. In the absence of that information, we had not performed preemptive thyroid blocking with potassium iodide. This underscores the necessity of the detection equipment (and team) to be able to discriminate and identify various radiocontaminants.
The U.S. Food and Drug Administration has previously issued guidance and suggested dosing regimens for the use of potassium iodide in radiation emergencies (15).
In a worsened disaster scenario, many more contaminated patients would have quickly exhausted our safe time limits for individual responders, requiring back-up teams in triage, treatment, and holding areas—a luxury few institutions have in place, particularly during off-shift hours.
CONCLUSION
Despite the above-mentioned findings, most of the participants complied with appropriate radiation protection protocols and triage algorithms. Patients were cared for and advised of radiation risks and protective measures. Nuclear medicine staff members are generally available on a 24-h basis and are well trained to assist in radiation monitoring, energy discrimination and analysis of contaminants, and basic patient care. They can play an important role in radiation disaster response, augmenting meagerly staffed Health Physics Departments. Preparedness planning and simulation drills require a significant commitment of time and resources. Critical analysis of these exercises assists in identifying limitations and weaknesses to the institution’s response, which, if corrected, may contribute to improved outcomes for any real event.
Acknowledgments
The authors gratefully acknowledge the assistance of Charles Mauceri, CNMT, and James Fitzgerald, CNMT, Department of Nuclear Medicine; and also thank Jean Hickey, RN, and Corinne Miller-Foster, RN (Emergency Medicine, Brigham and Women’s Hospital), for their review and comments; and John J. O’Reilly, III, RN (Emergency Medicine, Brigham and Women’s Hospital), for photographs of the radiation disaster exercise.
Footnotes
For correspondence or reprints contact: Robert Schleipman, MA, RT, CNMT, Department of Health Physics and Radiopharmacology, Brigham and Women’s Hospital, 75 Francis St., Boston MA 02115.
E-mail: aschleipman{at}partners.org





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}