


Abstract
Our purpose was to validate a semiautomatic quantification of the skeletal tumor burden on 18F-fluoride PET/CT using manual quantification as a reference. Methods: We quantified 51 18F-fluoride PET/CT examinations performed on female breast cancer patients. Clinical information (age; time of disease presentation; presence of visceral metastases; and time to death, progression, or a bone event) was recorded. The total volume of 18F-fluoride–avid skeletal metastases and the total activity of 18F-fluoride–avid metastases were calculated manually and semiautomatically. Results: Manual and semiautomatic metrics correlated strongly (P < 0.0001; 95% confidence interval, 0.9300–0.9769). On multivariable analysis, the semiautomatic measures of total activity for 18F-fluoride–avid metastasis correlated significantly with overall survival (P = 0.0001) and progression-free survival (P = 0.0006). Approximate times for calculating skeletal tumor burden (semiautomatic vs. manual) were, respectively, 30 s versus 321 s in patients with fewer than 5 metastases, 120 s versus 640 s in patients with 5–10 metastases, and 240 s versus 1207s in patients with more than 10 metastases. Conclusion: Semiautomatic quantification of whole-body 18F-fluoride PET/CT skeletal tumor burden can replace manual quantification in breast cancer patients and is a strong independent biomarker of prognosis.
Compared with conventional bone scintigraphy or SPECT/CT, 18F-fluoride PET/CT is more sensitive and specific in the detection of osteoblastic metastases because it detects a greater number of potentially metastatic lesions (1–3). Because of the clear benefits of 18F-fluoride PET/CT imaging, it seems logical to take maximum advantage of this novel tracer when evaluating patients with breast and prostate cancer. For example, the determination of 18F-fluoride PET/CT whole-body skeletal tumor burden is able to objectively assess response to treatment and is a better prognostic indicator than visual analysis (4,5). Investigators have demonstrated a prognostic role for 18F-fluoride PET/CT in breast (6) and prostate (7) cancers. Therefore, quantitative parameters with 18F-fluoride PET/CT can be important for clinical evaluation of patient outcome and for clinical trials, by eliminating subjectivity and assessing response to therapy. Despite these important benefits, manual calculation of 18F-fluoride PET/CT skeletal tumor burden can be time-consuming. To routinely implement semiautomatic quantification of 18F-fluoride PET/CT skeletal tumor burden, this tool must be validated by comparison to manual quantification.
The aim of this investigation was to validate semiautomatic quantification of skeletal tumor burden on 18F-fluoride PET/CT against manual quantification.
MATERIALS AND METHODS
Patients
We reviewed all 18F-fluoride PET/CT examinations performed on 51 female patients with breast cancer and suspected bone metastases.
The local Institutional Review Board approved this retrospective study (approval 46/2016), and the requirement to obtain informed consent was waived. Clinical information (age; time of disease presentation; presence of visceral metastases; and time to death, progression, or a bone event) for each patient was also recorded.
The median follow-up time starting from the 18F-fluoride PET/CT study was 15.4 mo (range, 1.6–83 mo). The mean age of the 51 patients was 56.7 y (range, 30–82 y).
18F-Fluoride PET/CT Acquisition
The studies were performed on 2 PET/CT scanners (Biograph True-Point 64 and Biograph 16; Siemens Healthcare) 45 min after a 3.7 MBq/kg intravenous injection of 18F-sodium fluoride. PET whole-body images (from the skull to the feet) were acquired in 3-dimensional mode at a rate of 90 s/bed position and then underwent iterative reconstruction (2 iterations of 8 subsets and a gaussian filter) or TrueX (Siemens) reconstruction plus time-of-flight reconstruction (2 iterations of 21 subsets with a gaussian filter). The CT acquisition parameters included a slice thickness of 5 mm, 120 kV, or CARE Dose4D (Siemens), with no intravenous CT contrast administration.
Image Analysis and Quantification Parameters
Two experienced observers visually analyzed all images.
Two forms of volumetric quantification were undertaken in all patients to determine whole-body skeletal tumor burden: a manual quantification using syngo.via (Siemens Medical Solutions) and a semiautomatic quantification using Multi-Foci Segmentation in syngo.via.
To standardize quantification in both methods, we established an SUVmax cutoff of 10. We were able to calculate the skeletal tumor burden with this cutoff because it has been shown to exclude normal bone in 98% of patients (8).
Using this SUVmax cutoff, we calculated 2 whole-body skeletal tumor burden metrics for the manual and semiautomatic quantifications: FTV10, or the total volume of 18F-fluoride–avid skeletal metastases (mL), and TLF10, or the total activity of 18F-fluoride–avid metastases determined by the equation FTV10 × the average of all the SUVmax (g) (8).
18F-Fluoride PET/CT Manual Quantification
To perform manual quantification, we first delineated FTV10 as a 3-dimensional ellipsoid volume of interest (VOI) that included all metastatic 18F-fluoride–avid skeletal lesions having an SUVmax above 10, with an isocontour threshold set at 41% of the SUVmax as recommended by guidelines (9). Subsequently, this FTV10 was multiplied by the average SUVmax (g/mL) (10) to obtain TLF10. The lesion with the highest SUVmax was also determined. Figure 1 shows an example of the manual quantification method.
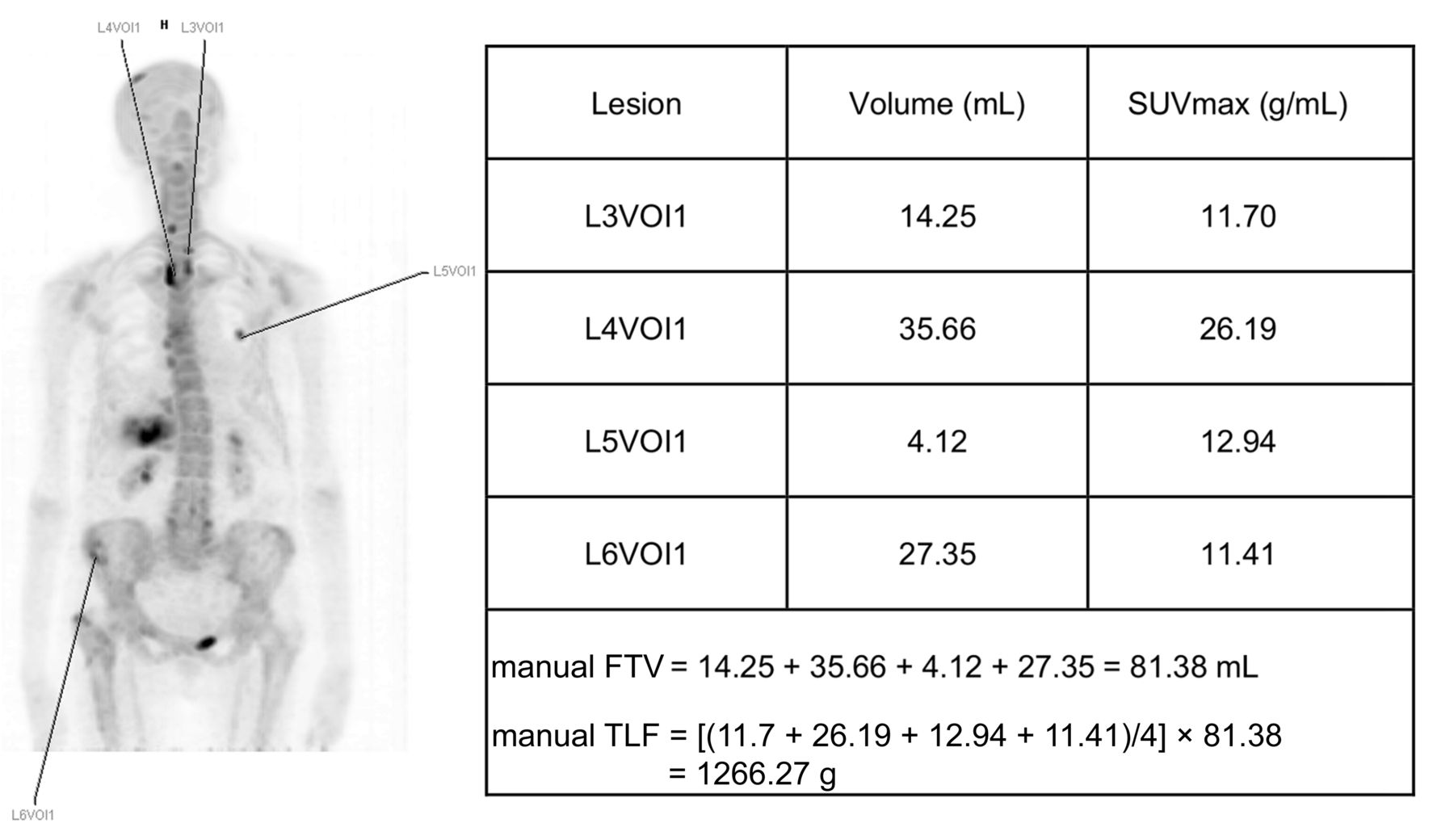
Example of manual quantification for one patient, with mFTV10 corresponding to sum of all VOIs (81.38 mL) and mTLF10 corresponding to mFTV10 multiplied by average of all SUVmax (1,266.27 g).
The time spent on manual quantification was defined as the interval from the manual designation of the VOI surrounding the bone metastasis (including the time to annotate all necessary data) through calculation of the manual FTV and TLF (mFTV10 and mTLF10).
18F-Fluoride PET/CT Semiautomatic Quantification
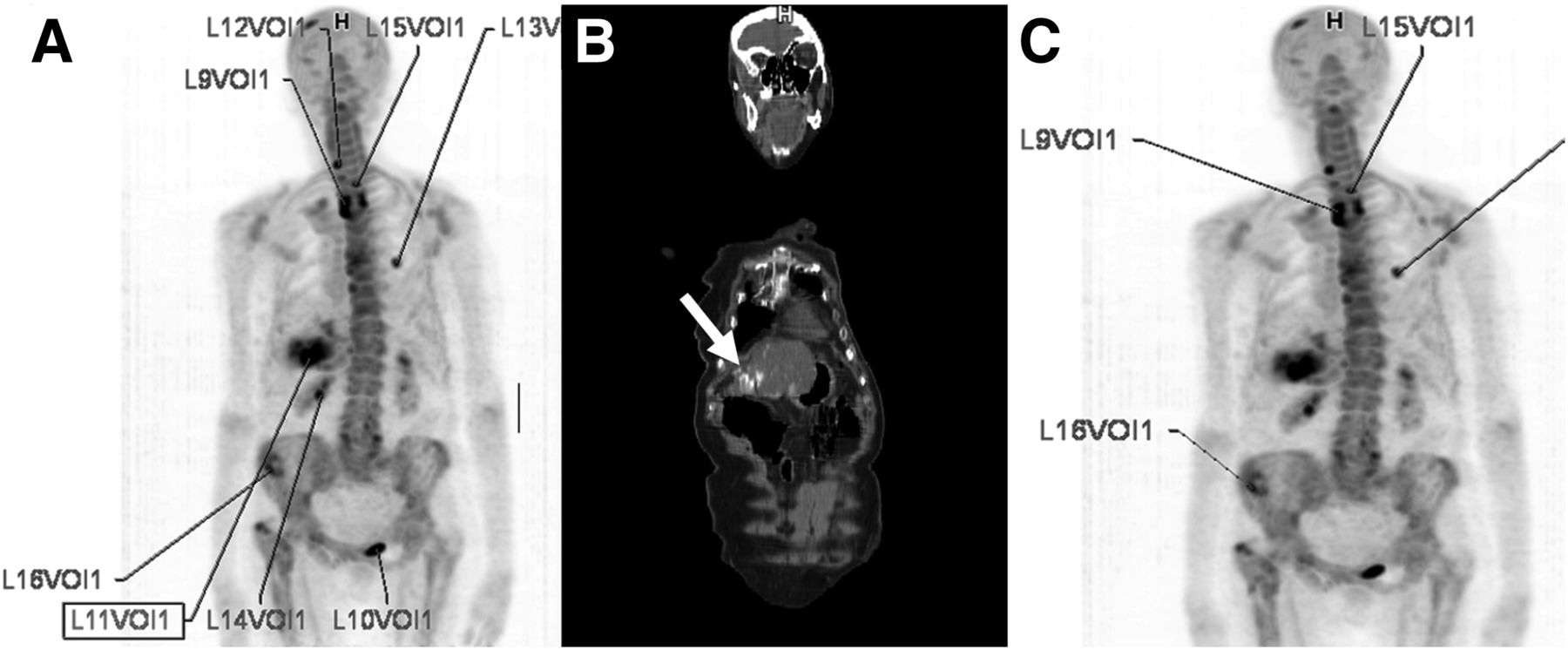
Semiautomatic quantification with the Multi-Foci Segmentation tool in syngo.via is feasible using any SUV cutoff. After we had determined that a cutoff SUVmax of 10 would be used, the software automatically generated VOIs surrounding all bone lesions with an SUV greater than 10. It was important, at that point, to verify that all delineated VOIs actually corresponded to bone metastases; if any did not, we manually excluded them. Subsequently, the skeletal tumor burden was determined according to the selected tumor-related areas (Fig. 2), and the software automatically provided the TLF10 and FTV10 parameters.
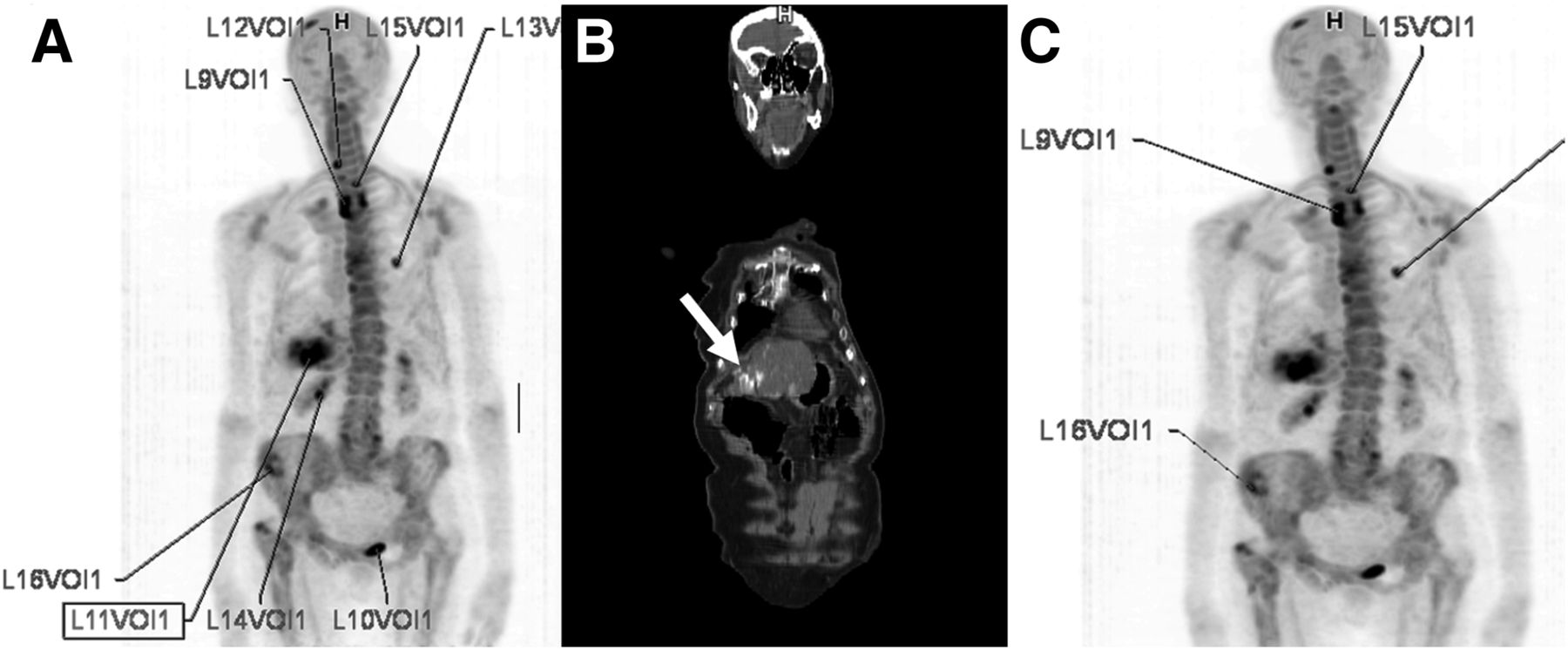
(A) After threshold selection (SUVmax of 10), several VOIs are automatically created. (B) On visual inspection, VOIs not related to metastases are deleted. In this patient, as indicated by white arrow in coronal section on CT scan, uptake was noted in calcified portion of liver, which was a sequela of radioablation (L11VOI1); this lesion was manually excluded. (C) Patient’s final saTLF10 was 3,969 g.
The time spent on semiautomatic quantification was defined as the interval from the automatic designation of the VOI surrounding the bone metastasis (including the time to manually exclude all nontumor areas) through calculation of the semiautomatic FTV and TLF (saFTV10 and saTLF10).
Statistical Analysis
The Pearson test, the Bland–Altman test (11,12), and mountain plots (13) were used to test the similarity between the 2 quantification methods. The Bland–Altman test was the default method to compare the 2 measurements; mountain plots were used as a complementary tool because they better visualize the differences.
Cox proportional hazards regression was used to evaluate the relationship between the whole-body skeletal tumor burden metrics and the following variables: outcome, age, time of disease onset, highest SUVmax, and presence of visceral metastases.
We studied the following outcome measures: overall survival, time to progression, and time to a bone event. Overall survival was defined as the interval from the 18F-fluoride PET/CT acquisition until death. Time to progression was defined as the interval from the 18F-fluoride PET/CT acquisition until any evidence of disease progression. Time to a bone event was defined as the interval from the 18F-fluoride PET/CT acquisition until the occurrence of any bone event. Even though bone events indicate progression of the disease, these events were calculated separately because of morbidity and mortality.
All statistical analyses were performed using MedCalc software. The level of significance was set at 5%.
RESULTS
During follow-up, 21 patients died (41.2%) and 29 progressed (56.9%). Nine patients who progressed had bone events (17.6%). One patient had no progression and remained alive throughout the follow-up.
18F-Fluoride PET/CT Manual and Semiautomatic Quantifications
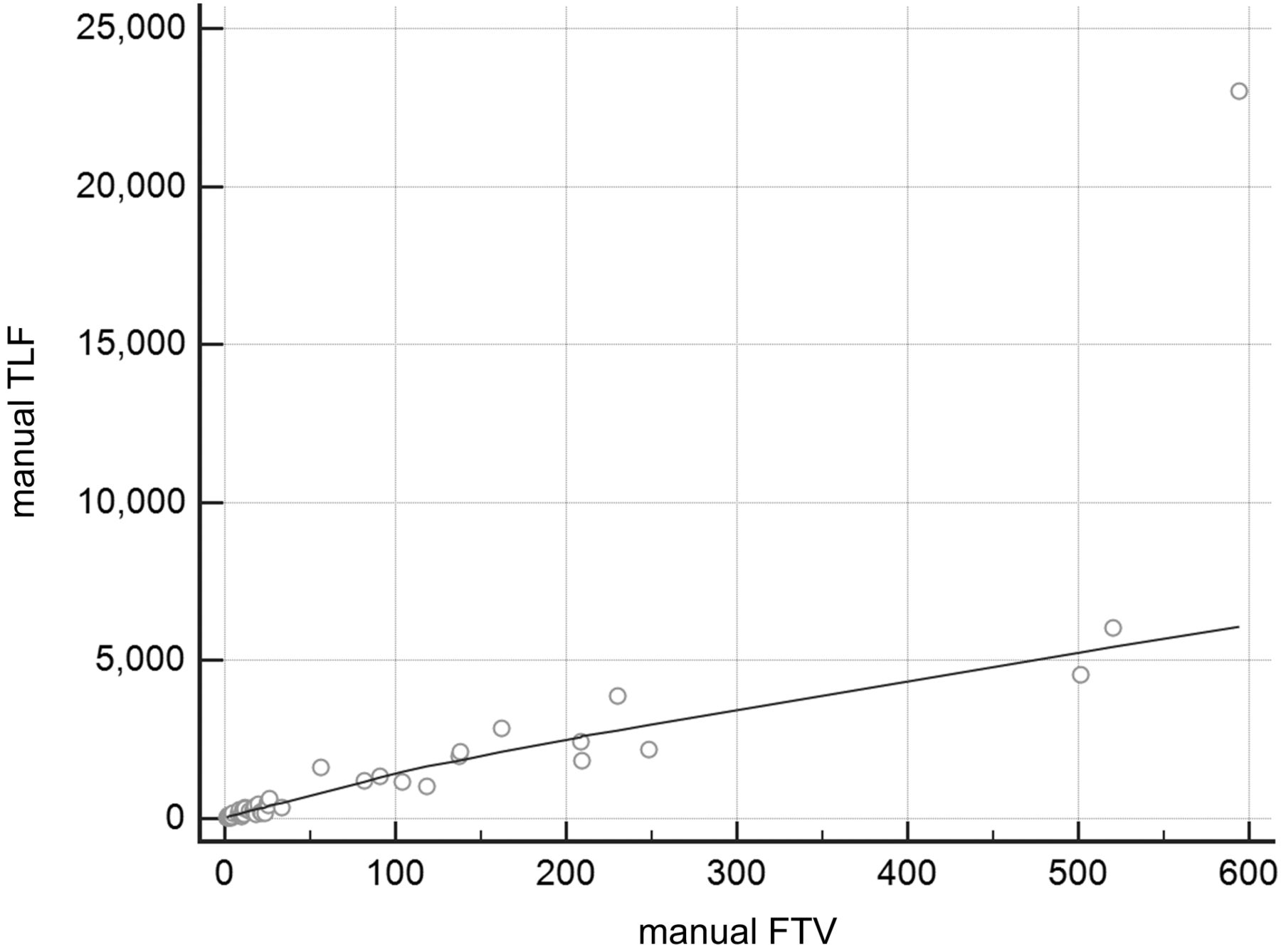
Because of the strong correlation between mTLF10 and mFTV10 (ρ = 0.8117; P < 0.0001; 95% confidence interval, 0.6905–0.8885), only mTLF10 was used for subsequent analyses (Fig. 3). The same was true for saTLF10 and saFTV10 (ρ = 0.9234; P < 0.0001; 95% confidence interval, 0.8690–0.9558), with only saTLF10 being used for subsequent analyses (Fig. 4).
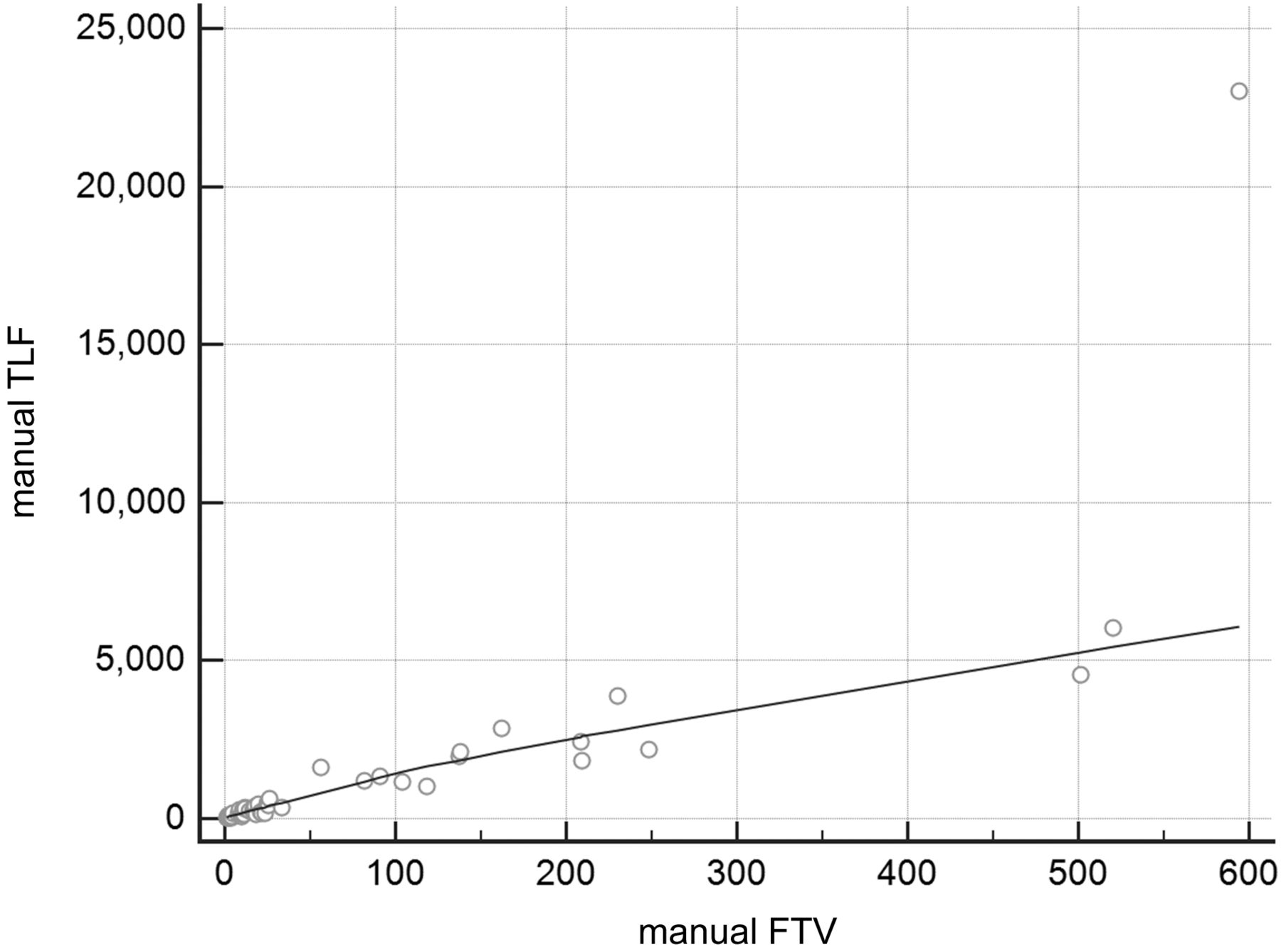
Graph showing strong correlation between values for mTLF10 and mFTV10 (ρ = 0.8117; P < 0.0001; 95% confidence interval, 0.6905–0.8885).
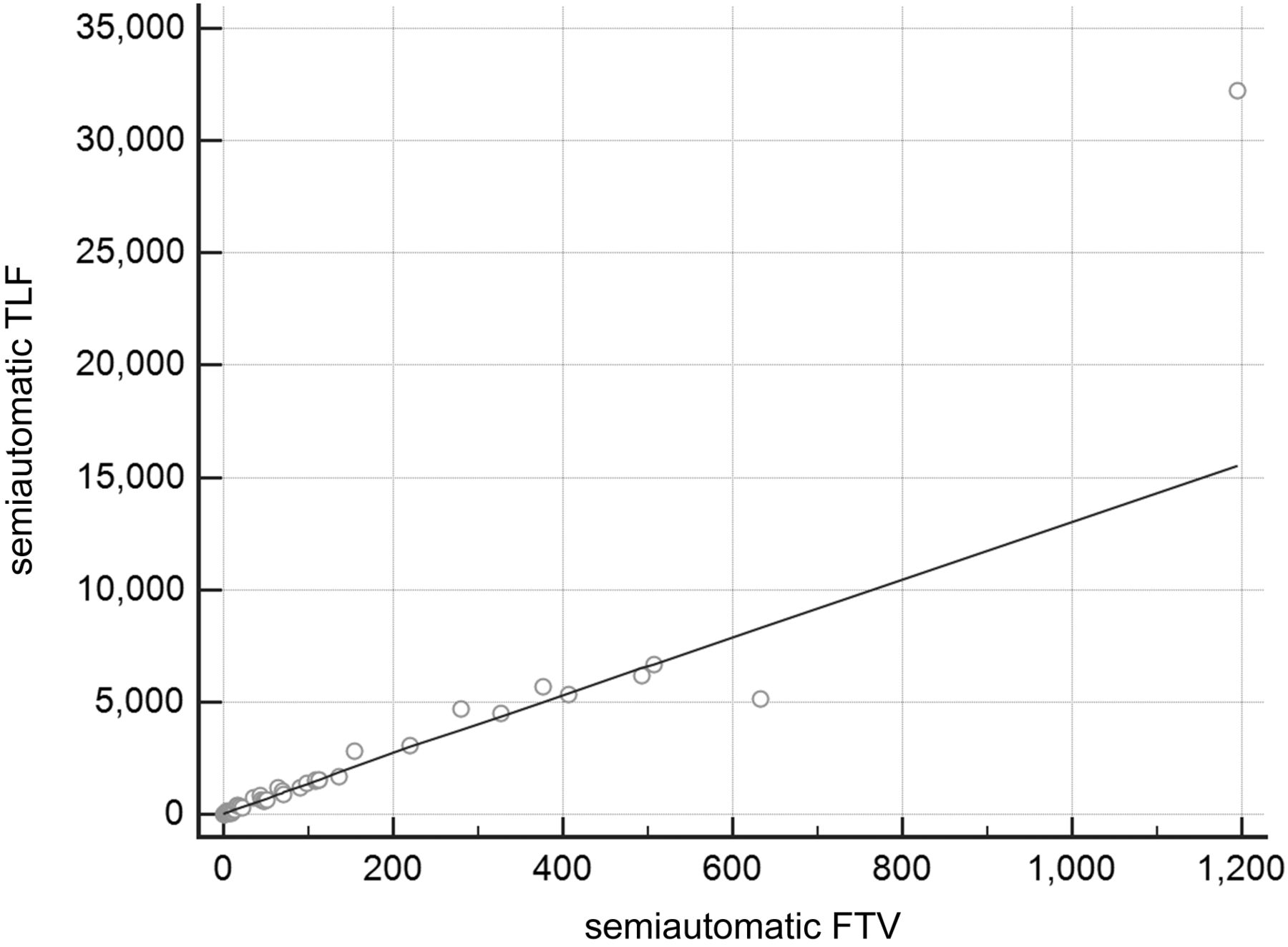
Graph showing strong correlation between values for saTLF10 and saFTV10 (ρ = 0.9234; P < 0.0001; 95% confidence interval, 0.8690–0.9558).
The median mTLF10 was 255 g (range, 18–23.027 g), and the median saTLF10 was 574 g (range, 8–32.225 g).
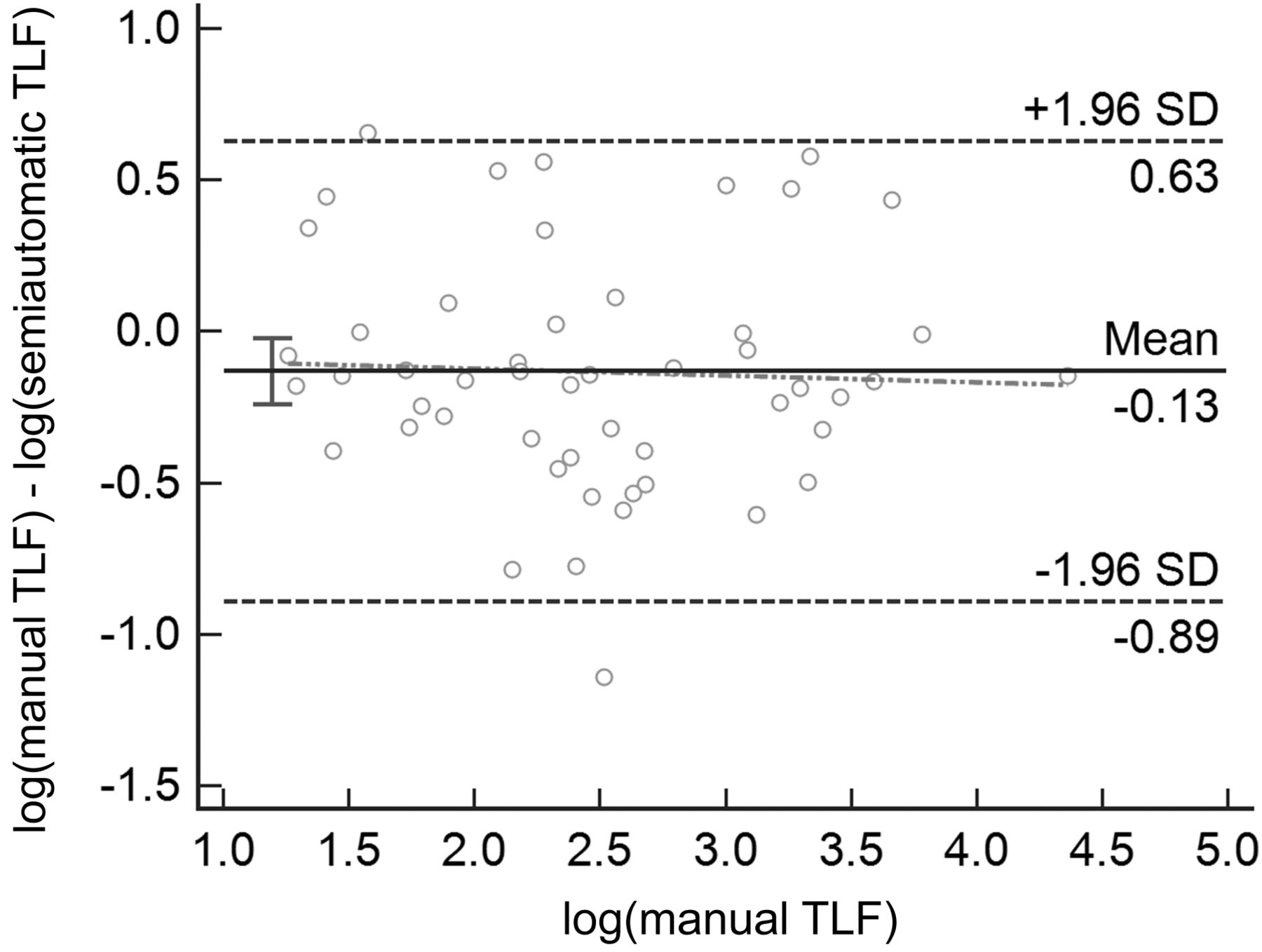
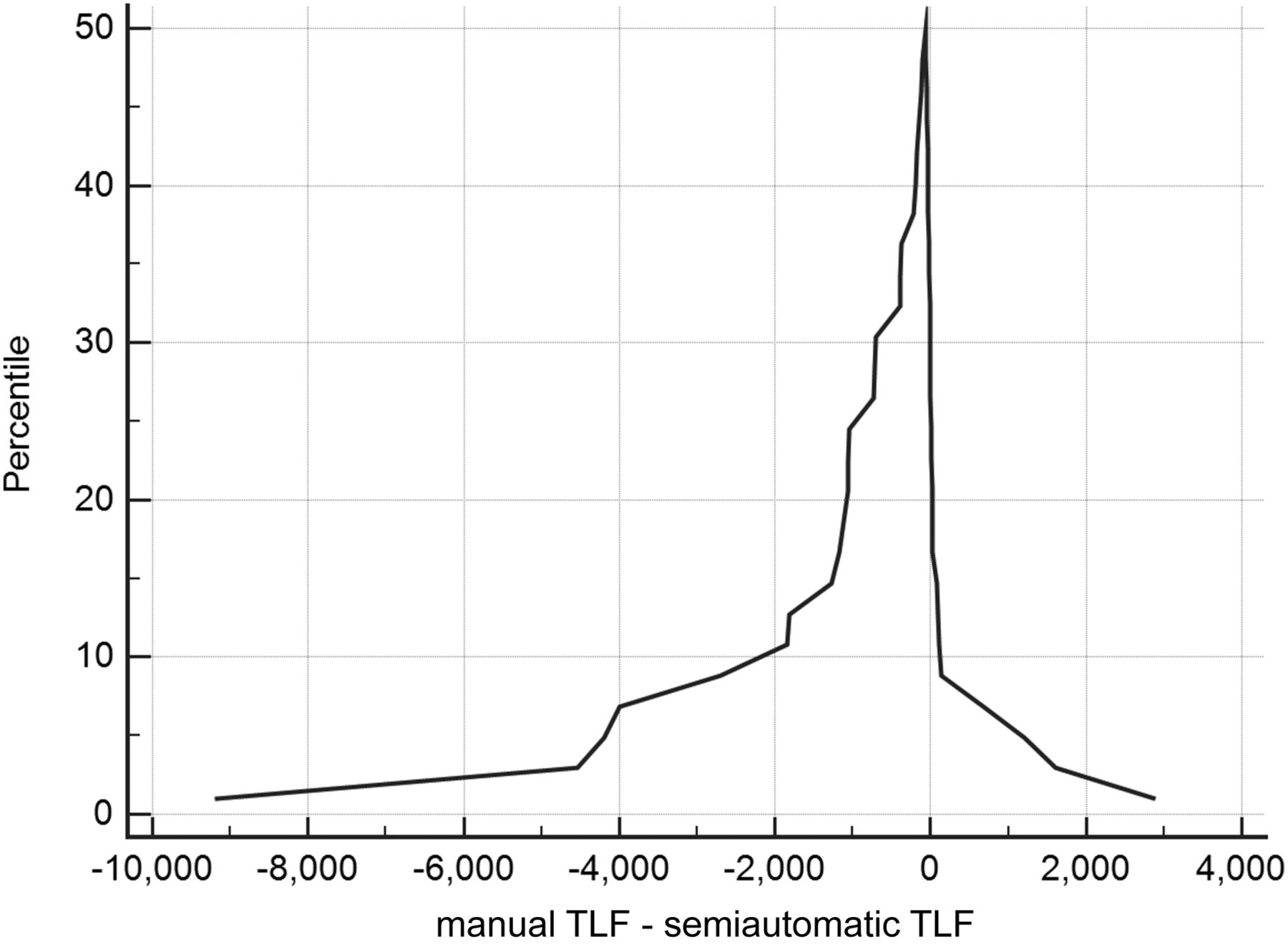
The Pearson correlation coefficient between mTLF10 and saTLF10 was 0.9596 (P < 0.0001; 95% confidence interval, 0.9300–0.9769). The Bland–Altman test showed similarity between the manual and semiautomatic methods. There was only one outlier, as seen in Figure 5. That patient had a high tumor burden on semiautomatic quantification and a low tumor burden on manual quantification (TLF10, 4,523 and 327.2 g, respectively). The mountain plots showed the center to be near zero, with a left tail (Fig. 6).

Bland–Altman test showing similarity between manual and semiautomatic quantifications.
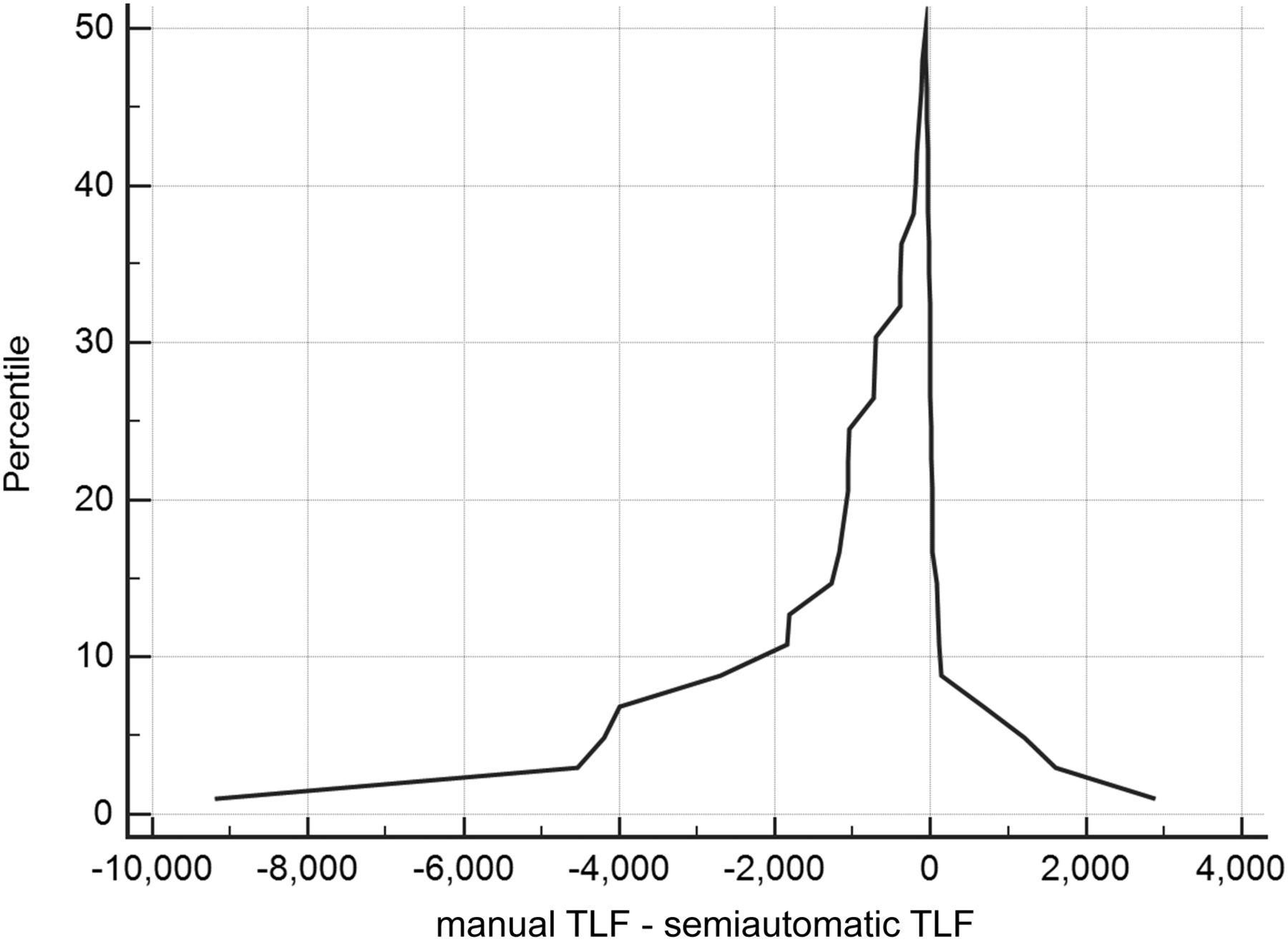
Mountain plot showing similarity between manual and semiautomatic quantifications, with peak near zero and small left tail.
Because of the strong correlation between mTLF10 and saTLF10, a multivariable analysis was undertaken solely on the semiautomatic measures. The analysis showed that saTLF10 correlated significantly with overall and progression-free survival (Table 1). None of the variables were associated with bone events. The highest SUVmax did not bear a significant prognostic value.
Correlation of Clinical and Imaging Variables to Overall Survival and Time to Progression on Multivariable Analysis
Approximate times for quantifying skeletal tumor burden (semiautomatic vs. manual) were, respectively, 30 s versus 321 s in patients with fewer than 5 metastases, 120 s versus 640 s in patients with 5–10 metastases, and 240 s versus 1,200 s in patients with more than 10 lesions.
DISCUSSION
Semiautomatic quantification of whole-body skeletal tumor burden with 18F-fluoride PET/CT (TLF10 and FTV10) has been shown to be a strong and independent prognostic biomarker in breast (6) and prostate (7,14) cancers. To the best of our knowledge, semiautomatic quantification of 18F-fluoride PET/CT had not previously been validated for clinical use. Therefore, we manually quantified whole-body skeletal tumor burden (the method of quantification most often used in clinical practice) and compared it with semiautomatic quantification to validate the latter method.
Like studies comparing manual with semiautomatic quantification for 18F-FDG PET/CT—studies that revealed a high level of agreement (15)—our study for 18F-fluoride PET/CT obtained comparable results. In our study, mountain plots were centered over zero for both the manual and the semiautomatic methods, with a small left tail, showing that although the methods had some differences, they correlated strongly overall. These differences were secondary to an underestimation of the manually quantified values in a few cases, when compared with the semiautomatic method. Furthermore, the visual assessment of the Bland–Altman scatterplots showed uniform bias, and we can thus conclude that these metrics are similar, equivalent, and strongly correlated.
Although both methods of quantification are related, the manual method is time-consuming. In addition, the manually drawn VOIs are elliptic; in patients with multiple lesions, the observer might reduce the size of these VOIs to avoid overlap of VOIs, and this reduction might reduce the total volume of lesions. That is why there was such a discrepancy between the median mTLF10 (255 g) and the median saTLF10 (574 g). This issue does not occur in the semiautomatic quantification because the software draws the VOIs according to the exact shape of the lesions, without overlap.
The semiautomatic quantification, therefore, clearly becomes the method of choice for whole-body tumor determination. Furthermore, it was necessary to confirm that saTLF10 and saFTV10 were prognostic factors in breast cancer. Specifically, when quantifying osteoblastic bone metastases on the 18F-fluoride PET/CT studies, we applied a cutoff SUVmax of 10, which has been shown to separate normal bone from malignant lesions in approximately 98% of patients (8,16). This cutoff is not undisputed, and some authors prefer a cutoff of 15 to minimize nonpathologic and normal-bone uptake (17,18). There are no comparative studies between the 2 cutoffs (10 and 15) to decide which is better. However, we believe that increasing the cutoff reduces the sensitivity (while increasing the specificity), potentially leading to erroneous measurement of skeletal tumor burden. After semiautomatic quantification, a visual inspection is warranted to manually exclude VOIs placed in areas unrelated to bone metastases. Hence, increasing the SUVmax cutoff (to 15, for instance) may render this task more time-consuming because not only will areas unrelated to bone metastases have to be excluded but areas related to bone metastases will have to be included.
One limitation of both quantification methods relates to metastatic lesions whose activity is near the level of physiologic activity. For instance, in a metastasis in the pubic bone, which is near the bladder, a perfect delimitation was sometimes not possible because of the physiologic urinary excretion. Manual quantification also has limitations, in addition to being laborious. First, because it is observer-dependent, the VOI may vary widely, potentially influencing the whole-body quantification results. Second, the number of quantifiable lesions is not perfect. Although manual quantification was attempted in all patients regardless of the number of lesions, in some patients with a very high tumor burden (above 20 VOIs delineated), the software processing began to slow (most likely because of work overload) and the workstation had to be restarted. This problem did not occur with the semiautomatic quantification method; therefore, that method has the additional benefit of being able to include all patients, even those with a high volume of disease. A recent study showed that manual volumetric quantification of 68Ga-PSMA PET/CT correlated with serum prostate-specific antigen values in patients with suspected biochemical recurrence of prostate cancer (19), but unfortunately, the authors excluded from the analysis patients with more than 10 lesions, claiming that manual measurement of tumor volumes was time-consuming and labor-intensive. To date, there is only one clear advantage of manual over semiautomatic quantification: the manual method allows drawing of an irregular ROI. In that scenario, semiautomatic quantification software still needs improvement, as there is no freehand drawing tool for VOIs, allowing only spheric VOIs and their variations. Segmentation is a necessary step in semiautomatic quantification and requires human interaction. Totally automatic forms of volumetric quantification will dispense with the segmentation process; such procedures are under study and will require extensive validation before clinical use (20).
One clear strength of this study was the possibility of addressing the clinical relevance of these quantitative findings. In our retrospective analysis of female breast cancer patients, semiquantitative determination of whole-body tumor burden on 18F-fluoride PET/CT independently correlated with overall survival (6). This finding demonstrates the potential of this approach for prognostication of these patients. Although we have validated this approach for breast cancer patients, our findings need confirmation for other cancer types.
Guidelines recommend that tumor burden be reported when available (9), but such reporting is feasible only for localized solid tumors. In current clinical practice, information on 18F-fluoride PET/CT skeletal tumor burden cannot be reported for patients with widespread disease such as lymphomas and bone metastases from breast and prostate cancer and must be reserved for research. A quantitative metric widely used in clinical practice because of its ease of measurement is SUVmax. In our analyses, the highest SUVmax on 18F-fluoride PET/CT examination was not a significant prognostic factor, as also shown by other investigators (6), even though the SUVmax of the primary lesion is a prognostic factor in breast cancer patients on 18F-FDG PET/CT (21,22). The lack of correlation between the highest SUVmax and outcome justifies calculation of whole-body skeletal tumor burden and not just the highest SUVmax.
In daily clinical practice, quantification of whole-body skeletal tumor burden has to be in at least a semiautomatic form. In this respect, the quantification proposed here is feasible, fast, and reproducible. These advantages open the door to new clinical possibilities in the theranostics setting (7,14) and in evaluating response to therapy (17).
CONCLUSION
Semiautomatic determination of whole-body skeletal tumor burden might be able to replace manual quantification for 18F-fluoride PET/CT in breast cancer patients. Furthermore, it is a strong independent prognostic imaging biomarker. These findings need confirmation in other cancer types.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Aug. 3, 2018.
REFERENCES
- Received for publication March 13, 2018.
- Accepted for publication June 29, 2018.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}