


Abstract
Chemotherapy followed by prophylactic cranial irradiation (PCI) is associated with increased survival in patients with small cell lung cancer but is associated with fatigue and cognitive impairment. This retrospective study evaluated regional differences in 18F-FDG uptake by the brain before and after PCI. The null hypothesis was that direct toxic effects on the brain from PCI and chemotherapy are symmetric; thus, asymmetric deviations may reflect functional changes due to therapy. Methods: Electronic medical records from 2013 to 2016 were reviewed for patients with small cell lung cancer, MRI of brain negative for metastasis, and 18F-FDG PET/CT scans before and after PCI. As the standard of care, patients received first-line chemotherapy or chemoradiation to the thorax followed by PCI. The 18F-FDG PET/CT scans nearest the PCI were selected. Sixteen patients met these initial criteria. Commercially available PET software was used to register and subtract the PET scans before and after PCI to obtain difference maps. Occipital and cerebellar regions were excluded from the final statistical analysis given the known high variability and misregistration. The χ2 test was used to analyze the data. Results: Two patients had 18F-FDG uptake differences only in the occipital and cerebellar regions. The software registration failed on 1 patient’s scans. Therefore, 13 patients were included in the final analysis. Nine of 13 patients demonstrated significant unilateral changes in only 1 region of the brain, and 3 of 13 showed significant changes unilaterally in 2 regions. The χ2 test revealed a significant unilateral regional difference on a patient level (χ2 = 6.24, P = 0.025). The most commonly affected brain region was the frontal lobe. Conclusion: Significantly more patients had unilateral than bilateral regional differences (both increases and decreases) in 18F-FDG uptake in the brain before and after PCI. This finding suggests that differences in unilateral distribution are related to functional changes, since direct toxicity alone from PCI and chemotherapy would be symmetric. The frontal region was the most commonly affected, suggesting a potential contributing etiology for cognitive impairment and decreased executive function after therapy.
- molecular imaging
- lung cancer
- 18F-FDG PET/CT
- cognitive impairment
- prophylactic cranial irradiation
- small cell lung cancer
Approximately 5%–10% of patients with lung cancer are diagnosed with high-grade-malignancy small cell lung cancer (SCLC). SCLC originates from neuroendocrine cells in the bronchus (1). The greatest risk factor for this type of lung cancer is smoking. Treatments for SCLC are limited. Depending on tumor stage and individual factors, the treatments that are considered include surgical resection, chemotherapy, or chemotherapy combined with radiotherapy to the thorax. Platinum-based chemotherapy remains the standard first-line chemotherapy in both limited and extensive stages of the disease (2,3).
A recent metaanalysis demonstrated a relative risk of approximately 45% for developing brain metastasis within 1 y after diagnosis for SCLC, plus a decreased incidence of brain metastasis after prophylactic cranial irradiation (PCI) (4). Multiple studies reported increased survival after PCI in patients with SCLC; however, controversy does exist in the literature, with one studying show similar outcomes for PCI versus a strategy of close observation with MRI (5–7). Additionally, cognitive impairment has been observed after chemotherapy, especially after combined whole-brain radiation therapy (8,9). An MRI study on patients with SCLC who received chemotherapy and PCI showed an association between long-term cognitive effects and structural brain changes (10).
This retrospective pilot study evaluated regional differences in 18F-FDG uptake of the brain in SCLC patients before and after PCI (all patients had already received first-line chemotherapy). The null hypothesis was that direct toxic effects on the brain from chemotherapy and whole-brain irradiation are symmetric. Hence, asymmetric differences in 18F-FDG uptake in the brain may represent functional changes as a consequence of the therapy.
MATERIALS AND METHODS
Patient Selection
This retrospective study was approved by the institutional Human Subjects Protection Program.
The electronic medical record database from 2013 to 2016 was searched for patients with biopsy-proven SCLC who received standard-of-care first-line chemotherapy followed by PCI (25 Gy in 10 fractions at 2.5 Gy per daily fraction). Patients were excluded if they had brain metastases or any other intracranial pathology that could alter 18F-FDG uptake. All included patients underwent 18F-FDG PET/CT at our institution before and after PCI as part of standard-of-care assessment of tumor response. The 18F-FDG PET/CT scans nearest the PCI (about 2 mo before and about 3 mo after) were selected. All 18F-FDG PET/CT scans at our facility extend from vertex to thigh. In total, 27 patients with SCLC were treated over this period, and 16 patients met the inclusion criteria.
PET/CT Scanning
A minimum of 4 h of fasting before intravenous administration of 18F-FDG was standard for all patients. Fingerstick blood glucose levels were measured before intravenous injection of 18F-FDG at a weight-based dose of 3.7 MBq (0.1 mCi)/kg, with a range of 185 MBq (5 mCi) to 370 MBq (10 mCi). After injection of 18F-FDG, the patients sat quietly awake for approximately 60 min. 18F-FDG PET/CT was performed from vertex to thighs using a GE Healthcare 690 time-of-flight PET/CT scanner. A low-dose CT scan was obtained without intravenous contrast material and with oral contrast material before the PET acquisition. The acquisition time was 2.5 min per bed position, and 7–8 bed positions were used, depending on the height of the patient. The PET data were reconstructed using ordered-subsets expectation maximization (28 subsets, 2 iterations).
Analysis of PET/CT Scans
The brain portions of the scans were saved as separate files and analyzed using commercially available software (MIM; MIM Software Inc.). MIMneuro, quantitative analysis brain software, was used to register and subtract the brain PET scans (before and after PCI) and obtain difference maps. The baseline scan was first registered to a template image to define the whole-brain outline region. A mutual information-based algorithm was then used for image coregistration. Registration was performed using the Assisted Alignment method, and the alignment was manually corrected as necessary. The 2 images were automatically normalized within the whole-brain outline region, and subsequent z score analysis was restricted to this region. For PET subtraction analysis z scores, the mean and SD were calculated for all voxels contained within the brain mask contour on the subtraction data. In MIMneuro, the z score analysis window displays regions with low metabolism or perfusion and regions with high metabolism or perfusion. Regions are displayed in the “hyper” or “hypo” z score list of MIM if the region is unilaterally hypermetabolic or hypometabolic, even if the entire bilateral region is not hypermetabolic or hypometabolic. For each patient, areas of the brain with differences greater than a z score of ±2.5 were recorded. Each area of significant difference was categorized into 1 of 5 lobar regions (frontal, parietal, temporal, occipital, or cerebellar) by the software program. The occipital region was excluded from the final analysis given the known high variability in this region from visual stimulation. The cerebellar region was also excluded because of misregistration of brain to bone.
Statistical Analysis
The data were analyzed using single-variable χ2 tests to determine whether the distribution demonstrated significant changes in only 1 region (asymmetric) of the brain or bilaterally (symmetric).
RESULTS
Sixteen patients with biopsy-proven SCLC met the inclusion and exclusion criteria. The software registration failed for 1 patient, and 2 patients had 18F-FDG uptake differences only in the occipital and cerebellar regions. Thus, 13 patients were included in the final analysis for regional cerebral differences. The mean age was 65 y (range, 49–78 y), and 6 of 13 (46%) were female. Five of 13 (38%) had limited-stage SCLC, and 8 of 13 (62%) had extensive-stage SCLC. Table 1 provides the characteristics of the study population.
Patient Characteristics (n = 13)
The average blood glucose measured before injection of 18F-FDG was 117 mg/dL (range, 83–281 mg/dL) on the pre-PCI scan and 98 mg/dL (range, 80–121 mg/dL) on the post-PCI scan. The mean of the differences in blood glucose, subtracting the post-PCI from the pre-PCI values on an individual basis, was 19 mg/dL with an SE of 14 mg/dL. The average 18F-FDG uptake time was 62 min (range, 49–70 min) for the pre-PCI scan and 62 min (range, 51–75 min) for the post-PCI scan.
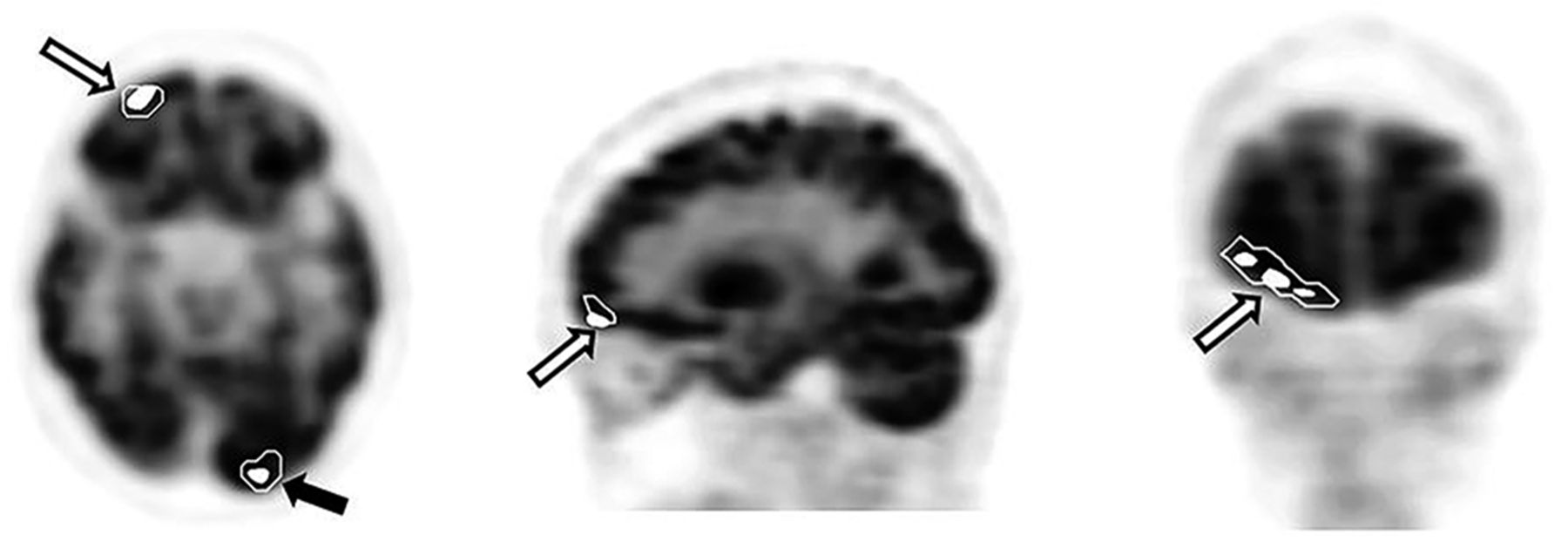
Statistically significant increases or decreases in regional cerebral 18F-FDG uptake before PCI compared with after PCI were found in 13 patients. Nine of 13 patients (69%) demonstrated significant unilateral changes in only 1 region of the brain (Fig. 1), and 3 of 13 (23%) showed significant changes unilaterally in 2 regions. Only 1 patient showed bilateral changes (frontal). Therefore, 12 of 13 patients (92%) showed unilateral regional changes. Overall, a χ2 test for unilateral regional differences on a patient level was significant (χ2 = 6.24, P = 0.025). Eight patients showed significant positive z score differences (z ≥ 2.5), and 3 displayed negative z score differences (z ≤ −2.5). Two patients demonstrated negative as well as positive z score differences in different regions. The most commonly affected cerebral region was the frontal lobe, in 8 of 13 (62%) patients. Five patients showed significant differences in the parietal lobe and 3 in the temporal lobe (Table 2).

Subtracted pre- and post-PCI 18F-FDG PET images using MIMneuro software are presented in transaxial (left), sagittal (middle), and coronal (right) planes. A region of right frontal lobe (white arrows) was calculated to have 18F-FDG uptake difference greater than z score ≥ +2.5. A region of left occipital lobe (black arrow) also demonstrated difference after subtraction.
Regional z Score Differences for Each Patient (n = 13)
DISCUSSION
To the best of our knowledge, this retrospective pilot study was the first to investigate regional increases or decreases in 18F-FDG uptake of the brain before and after PCI in patients with SCLC (all previously treated with first-line chemotherapy). If changes in 18F-FDG uptake were solely due to direct cellular toxicity from systemic chemotherapy or whole-brain irradiation and not to functional changes, one would expect to see symmetric differences in 18F-FDG uptake in the brain before and after radiation. However, significantly more patients had unilateral (92%) than bilateral (8%) regional uptake differences. The χ2 test for unilateral regional difference on a patient level was significant (P = 0.025). The percentage of asymmetric regional differences in 18F-FDG uptake in the cerebrum after chemotherapy and PCI suggests that functional brain changes related to PCI are likely common. The frontal lobe was the most commonly affected cerebral region.
Horky et al. found decreased glucose metabolism in both gray and white matter structures associated with chemotherapy for SCLC, and the frontal cortex was more affected (11). In breast cancer patients, Silverman et al. used a combination of 15O-water and 18F-FDG PET to reveal changes in the activity of the frontal cortex 5–10 y after completion of chemotherapy (12). This result in the frontal region may suggest an etiology for cognitive impairment after therapy, also referred to as chemo-brain. Prior studies in SCLC have also shown that first-line chemotherapy followed by PCI was associated with development of cognitive impairment (9,10). Commonly reported cognitive dysfunctions include decreased attention, loss of concentration, and impaired memory (13).
A limitation of this pilot study is the relatively small sample size. However, our results are in line with the above-cited studies and thus together do support the hypothesis that asymmetric differences in 18F-FDG uptake in the brain may represent functional changes as a consequence of PCI after chemotherapy. These results justify assessing functional changes in the brain by 18F-FDG PET/CT in a larger, prospective study that would allow for correlation of 18F-FDG PET/CT parameters (by region and direction of change) with cognitive testing and quality-of-life assessments. This analysis could also be performed for patients with different types of cancers and therapies, which may allow separation of the effects of chemotherapy from radiation therapy. Another possible limitation is that despite instructions to sit quietly, patients may have been active during the 18F-FDG uptake period.
CONCLUSION
This retrospective pilot study of SCLC patients who underwent chemotherapy followed by PCI found unilateral increases and decreases in 18F-FDG uptake by the brain before and after PCI. Importantly, asymmetric rather than symmetric regional differences were observed, suggesting functional changes after PCI since direct toxicity alone from PCI and chemotherapy would be symmetric. The most commonly affected region was the frontal cortex, which may suggest an etiology for cognitive difficulties after therapy.
DISCLOSURE
Phillip Kuo is a consultant or speaker for Endocyte, GE Healthcare, Imaging Endpoints, Invicro, Lilly, MD Training at Home, Molecular Neuroimaging Institute, and Progenics; is an investigator for clinical trials with Astellas, Endocyte, GE Healthcare, and Merck; and has educational and investigator-initiated grants from GE Healthcare. No other potential conflict of interest relevant to this article was reported.
Footnotes
Published online Aug. 3, 2018.
REFERENCES
- Received for publication April 5, 2018.
- Accepted for publication May 31, 2018.





{kind=link}