


Abstract
Gastric emptying studies are routinely performed in many nuclear medicine departments; however, there are many different techniques used to perform the procedure across the country. Creating consistency in clinical practice will aid gastroenterologists in diagnosing and treating illnesses associated with abnormalities related to gastric emptying. In 2017, Cincinnati Children’s Hospital adopted adult standards for pediatric gastric emptying studies that included a standard meal along with imaging over the course of 4 h. Gastric emptying studies are the second-highest-volume examination performed in the nuclear medicine section at Cincinnati Children’s Hospital. Accommodating this volume required changes in the scheduling template, scheduling questionnaire, and epic order sets, as well as identification of specific days and locations for gastric emptying studies. Both protocol standardization and workflow optimization are critically important in creating consistency in patient care. Gastric emptying can be evaluated with solid food, liquid food, or solid and liquid food simultaneously. The methodology of the study is initially determined by the ordering provider but may require special accommodations based on what the patient will tolerate. In coordination with the ordering and interpreting physicians, the nuclear medicine technologists at Cincinnati Children’s Hospital have the decision-making ability to deviate from the provider’s request as necessary, which helps expedite workflow and eliminates wasted time. Any deviation from the standardized protocol is documented by the nuclear medicine technologist and incorporated into the final report by the interpreting physician, as dietary information is meaningful to the ordering provider. Reference values associated with the standardized or modified protocol are also included in the final report.
Gastric emptying studies have become increasingly common, not because they are exceptionally awesome to look at or overly fun to perform but because they provide gastroenterologists with information on how well a patient’s stomach is functioning. The primary indication for performing gastric emptying studies is to rule out gastroparesis, a condition in which the stomach empties too slowly. A secondary indication is to rule out dumping syndrome, in which the stomach empties too quickly. Assessment of gastric emptying in nuclear medicine is based on the meal consumed. Challenges in performing gastric emptying studies in a pediatric population include food allergies (1) and the fact that many children are picky eaters. To accommodate young patients, there needs to be flexibility in the performance of the gastric emptying study so that it will continue to provide meaningful results to the ordering providers.
Performing a gastric empty protocol is relatively simple; however, several considerations need to be factored into clinical practice, especially when the volume of studies continues to rise. Most of the considerations fall into 2 categories: technical aspects of the study, and logistics and patient workflow. The structure of the nuclear medicine department is critical when performing a large volume of gastric emptying studies, including the number of available cameras in the department, the available collimators for each camera, and the available patient prep rooms. Assessing these key elements ahead of time will be helpful when developing a workflow pattern to support a high volume of gastric emptying studies. This article summarizes Cincinnati Children’s Hospital’s camera acquisition protocols, scheduling templates, and patient and meal preparation, as well as briefly discussing what the results of the gastric emptying study can provide for patient care.
Variety of Gastric Emptying Studies
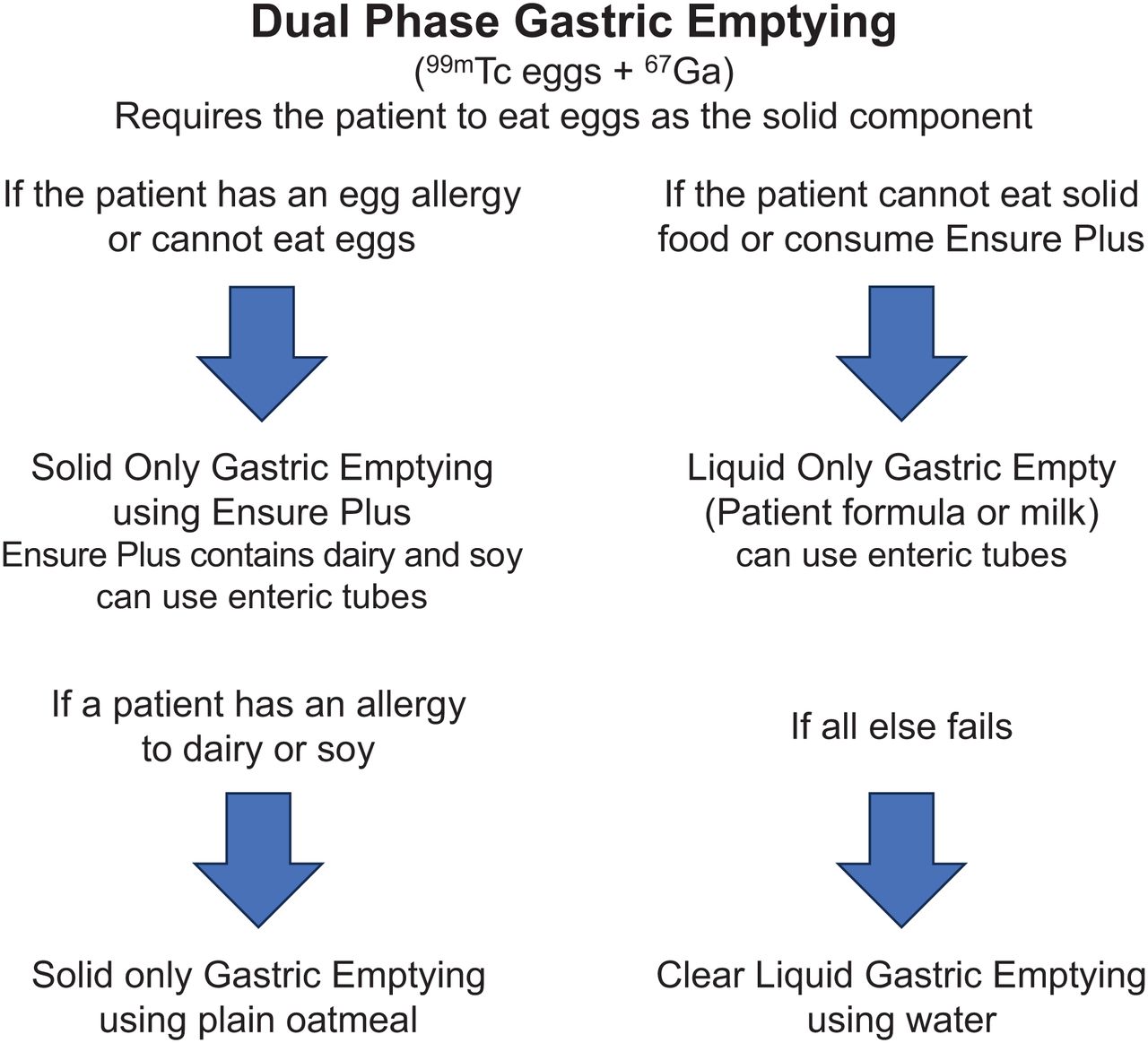
At Cincinnati Children’s Hospital, there are 3 different types of gastric emptying studies routinely performed: dual-phase (solid and liquid), single-phase (solid only), and liquid phase (liquid only). Gastric emptying studies begin with evaluating a patient for a dual-phase study and, from there, cascade to either a solid phase or liquid phase. The study performed is determined by what radiolabeled food the patient can consume. Dual-phase gastric emptying uses 99mTc-sulfur colloid–radiolabeled egg whites as the solid phase and 67Ga-citrate mixed with apple juice or water as the liquid phase (2,3). In our department, the solid-phase gastric emptying study is performed with radiolabeled egg whites, Ensure Plus (Abbott Laboratories) (4), or plain oatmeal (5). Liquid gastric emptying studies use the patient’s formula, milk, or clear liquid. Flexibility is essential in this patient population and is dependent on what the child will or will not eat. At Cincinnati Children’s Hospital, the nuclear medicine technologist is permitted to modify the dual-phase study as needed (Fig. 1).

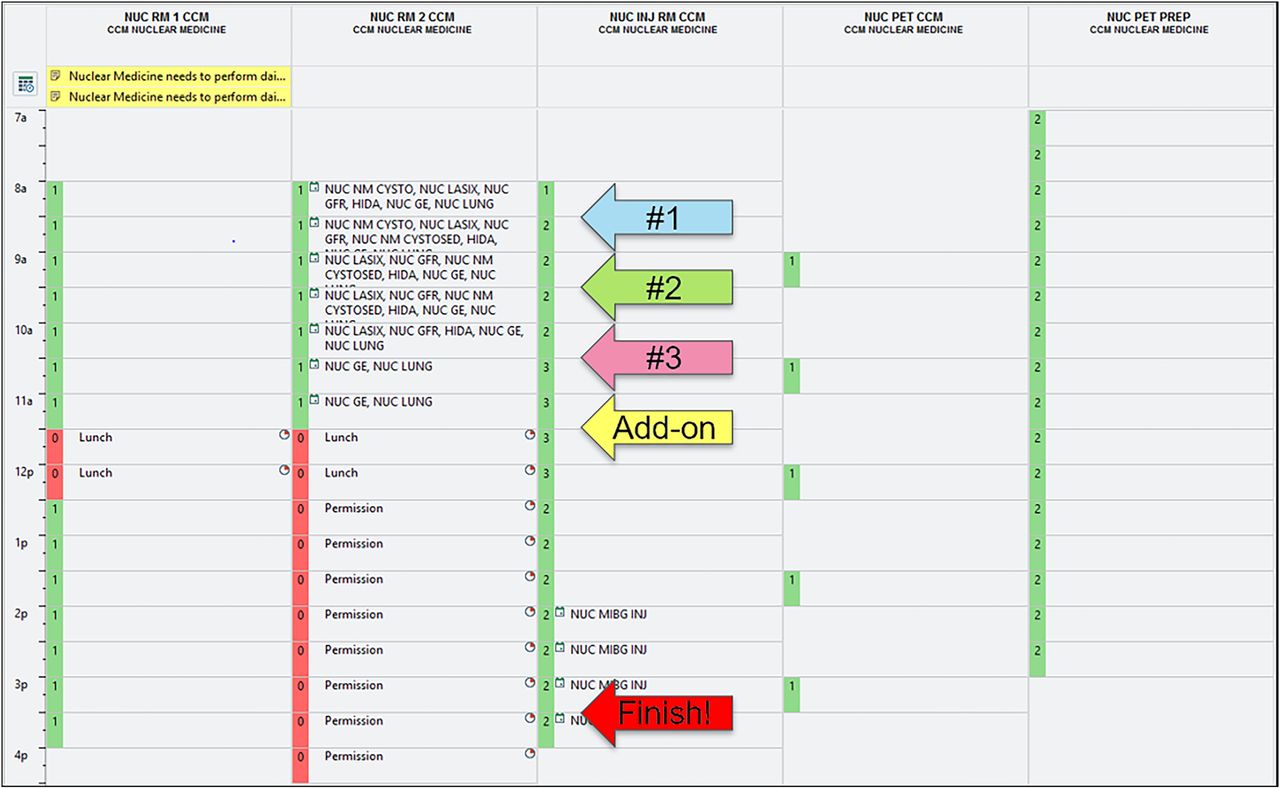
Epic schedule template for gastric emptying studies. Central scheduling can schedule 3 gastric emptying studies in 1 d. Scheduling template is blocked as “permission” in afternoon to allow for gastric emptying studies to be performed over 4 h.
Schedule Considerations
Patient preparation includes having the patient eat and drink nothing for 4 h before the study. We have found that scheduling the studies in the morning helps with patient satisfaction and staff satisfaction, with the standard meal more closely resembling breakfast or brunch. Adopting a standard meal for the study creates consistency, and the study results are comparable with reference values in the literature (2,6). The standard-meal study with solid food (egg whites), or a solid-food substitute (Ensure Plus) requires periodic imaging over the course of 4 h. At our institution, we needed to build a schedule template that would accommodate a high volume of gastric emptying studies while allowing the department to offer other nuclear medicine studies as well. This was accomplished by dedicating one of our γ-cameras to gastric emptying studies on Mondays, Tuesdays, Thursdays, and Fridays. Even though the study is 4 h in length, we schedule patient appointments in 1-h blocks to allow 3 or even 4 patients to be scheduled on a single day.
Our patient preparation on the day of the study is often the slowest phase of the study. The patient is brought to the prep room, where the technologist will obtain a patient history, explain the study, review allergies, answer any questions the patient (or parents) may have, and then give the patient the meal.
Patients have 10 min to consume the standard meal. Patients do not need to be in the γ-camera room while eating the meal; thus, use of the patient prep rooms aids in facilitating patient workflow. Patients simply leap-frog each other for imaging (Fig. 2).

Flow diagram of gastric emptying studies starting with dual-phase gastric emptying. Changes based on what patient can be fed are permitted.
Dual-Phase Gastric Emptying
The dual-phase gastric emptying components include a solid phase and a liquid phase. The solid phase consists of 118 mL (4 oz) of 99mTc-sulfur colloid–labeled egg whites. We use commercially available Egg Beaters (Bob Evans Farms, LLC) at our institution.99mTc-macroaggregated albumin can be substituted for 99mTc-sulfur colloid in the event of a sulfur colloid shortage. The liquid phase consists of 118 mL (4 oz) of 67Ga-citrate apple juice or water, whichever the patient prefers. We radiolabel the egg whites in the hot lab and cook them in a microwave oven that is designated for radioactive material use only. We use a disposable measuring cup and pour 118 mL (4 oz) of Egg Beaters into a 473-mL (16-oz) microwave-safe bowl. Liquid egg whites expand when cooking.
For the liquid phase, 111In-diethylenetriaminepentaacetic acid (DTPA) may be substituted for 67Ga-citrate if 67Ga-citrate is not available or if 111In-DTPA is preferred. There are significant cost differences between 67Ga-citrate and 111In-DTPA that should be considered. Unit doses of 67Ga-citrate are purchasable, whereas 111In-DTPA is typically sold in a 55.5-MBq (1.5-mCi) vial at a price that is approximately 35 times higher than a unit dose of 67Ga-citrate. One counter advantage to using 111In-DTPA over 67Ga-citrate, despite the cost, is that 111In-DTPA production is more reliable than 67Ga-citrate production.
When performing gastric emptying studies, we have found it advisable to provide patients with an emesis bag to contain any radioactivity in case they vomit. Cleaning up radioactive contaminants from a waiting room is not fun and will often alarm other patients and families when they see spill kits and radiation detection equipment in use. If a patient vomits during the gastric emptying study, the study must be terminated; accurate gastric emptying can no longer be calculated because of the change in stomach volume.
Dual-Phase Imaging Protocol
γ-cameras will need to be configured to accept 2 energy windows for the dual-phase study. When building the acquisition protocol for the dual-phase study, one should refer to the manufacturer guidelines for the specific camera to set the required energy peaks. At our institution, the photo peak for 99mTc is set at 140.5 keV with a window of ±10% and the 67Ga photo peak is set at 184 keV with a window of ±10%. The computer program (Xeleris; GE Healthcare) used for processing our gastric emptying studies requires 99mTc to be the first nuclide set or the program will not work correctly. We set our acquisition protocol with a 128 × 128 matrix and 2-min acquisitions at the standard time points: 0 min, 1 h, 2 h, 3 h, and 4 h.
A medium-energy general-purpose collimator must be used for the 184-keV photons generated by 67Ga. If we use 111In-DTPA for the liquid phase, the second energy setting is built for the 2 primary energy peaks of 171 and 245 keV for 111In. The higher-energy γ-emissions from 111In also require the use of a medium-energy general-purpose collimator.
Before the patient consumes the solid meal and the liquid, we prepare and acquire the 67Ga standard. The 67Ga standard is used to capture the total 67Ga activity to be administered to the patient and will be needed for postprocessing. The 67Ga standard allows the γ-camera to separate the 2 radiopharmaceuticals to calculate the solid 99mTc phase and the liquid 67Ga phase emptying. In preparing the 67Ga standard, we pour a small amount of apple juice or water (whichever the patient has chosen to drink) into a disposable cup—covering the bottom surface of the cup—and then squirt the 67Ga-citrate dose into the cup and rinse the syringe multiple times by pushing and pulling the plunger to ensure complete delivery of the 67Ga into the liquid. We center the 67Ga standard in the field of view, approximately 30 cm away from the camera head. We acquire a posterior view of the 67Ga standard for 2 min. Approximately 20% of the 67Ga 184-keV backscatter photons will bleed into the 99mTc window and will need to be subtracted when the data are processed.
The full standard meal for the solid-phase study consists of 118 mL (4 oz) of radiolabeled scrambled egg whites (e.g., Egg Beaters), 2 slices of white bread or toast, 2 packs of jelly (30 g), and 118 mL (4 oz) of water. Gluten-free bread is not allowed because it was not studied when the adult standard protocol was developed. If a patient has a gluten sensitivity, bread should not be included with the standard meal. Patients will likely forego the 2 packs of jelly if bread is not available to spread the jelly on. If the meal is modified in any way, what the patient consumed should be recorded. Once the standard meal is prepared, we encourage the patient to start eating the standard meal before we offer the 67Ga liquid dose (Table 1) in the disposable cup. We record what the patient ate and how long it took the patient to consume the meal. We do not let the patient eat for longer than 10 min, as the stomach can begin to empty before the 0-min image is acquired. We follow the image acquisition camera protocol and acquire a 2-min conjugate view (anterior and posterior) geometric mean image approximately every hour for up to 4 h. We conclude the study at 4 h or when 90% emptying of the solid meal is achieved.
Gastric Emptying Dose Chart
When several dual-phase gastric emptying studies are performed on a single γ-camera in a single day, some images are of greater importance than others. The 0-min image is the baseline image with which the stomach counts are compared over time to calculate emptying. Stomach emptying can begin before the 0-min acquisition if a patient takes too long to eat or if there is hypermotility. If the small bowel is visualized on the 0-min image, we include total abdominal counts (stomach and small bowel) as the region of interest for the baseline image so that total gastric emptying can be calculated. We acquire the 1-h image to rule out dumping syndrome, a stomach that empties too quickly. We acquire the 2-h image to compare with reference values for both solids and liquids at the 2-h time point. The 3-h image may be omitted if there are patient workflow issues or if the camera room is needed for other patients. We have found that one advantage of acquiring the 3-h image is that patients may achieve 90% emptying of solids at this time and the study can be completed. The 4-h image is needed if 90% emptying of the solid food phase has not been achieved at 3 h and final percent emptying calculations are needed to compare with reference values (Table 2).
Reference Values for Various Types of Gastric Emptying Studies
Single-Phase Gastric Emptying: Egg Whites or Ensure Plus
If a dual-phase study cannot be performed for any reason, such as if the radiopharmaceutical used for the liquid phase is not available or if the patient has an egg allergy or simply does not like eggs and refuses to eat them, we perform a single-phase gastric emptying study. In our department, labeled-food options for performing a single-phase gastric emptying study include liquid egg whites, Ensure Plus, or plain oatmeal. Our protocol for liquid egg whites or Ensure Plus (4) is the same as for the dual-phase study. The only difference is that 67Ga or 111In is not used to radiolabel liquid. Patients able to eat scrambled egg whites are offered apple juice or water to drink with the study. Patients consuming Ensure Plus or oatmeal for the study are not offered apple juice or water with the meal. Our camera acquisition protocol for the single-phase study uses only the 99mTc energy of 140.5 keV with a window of ±10%. We acquire conjugate-view geometric mean images for accurate emptying measurements (7). We have found that acquiring anterior and posterior conjugate-view static images improves the accuracy of the study by accounting for individual patient body habitus, patient attenuation, and scatter correction. In our experience, true stomach activity is higher when conjugate-view images are acquired than when single-projection (anterior or posterior) acquisition methods are used. The images of importance are the same as for a dual-phase study. Imaging at 3 h can also expedite completion if 90% gastric emptying has been achieved.
Single-phase studies using labeled egg whites, Ensure Plus, or plain oatmeal can be performed using either low-energy collimators or medium-energy collimators. Our technologists do not change collimators when they are performing multiple gastric emptying studies that vary between dual-phase and single-phase. The study is only collecting count data; image resolution is not relevant. Not changing collimators between patients is a significant time saver. We use medium-energy collimators if a dual-phase study is on the schedule even if single-phase gastric studies are also scheduled.
Single-Phase Gastric Emptying with Oatmeal
The last option for performing a single-phase gastric emptying study is to use plain oatmeal if a patient cannot consume liquid egg whites or Ensure Plus. 99mTc-sulfur colloid is the radiopharmaceutical of choice to radiolabel oatmeal (5). Unlike dual-phase or single-phase studies using Ensure Plus, the duration of a single-phase gastric emptying study with oatmeal is 1 h. Like dual-phase or other single-phase studies, low-energy or medium-energy collimators can be used. We still acquire an initial image (0 min) after the patient consumes the oatmeal but will also acquire an image at 30 min to rule out dumping syndrome. The image at 60 min will be the last image acquired. Reference values are greater than 50% emptying at 60 min.
Liquid-Only Gastric Emptying
In our department, a liquid gastric emptying study consists of any radiolabeled food that is not scrambled egg whites, Ensure Plus, or oatmeal. Liquid gastric emptying studies are performed when children are too young to consume solid food offered as part of a standard meal for solid studies. Allergens to ingredients such as eggs, dairy, or soy can steer patients to a liquid gastric emptying study. Additionally, a liquid-only study may be required for children with specific formula or dietary restrictions.
Unlike dual-phase or single-phase studies, in which conjugate view images are acquired, posterior images are acquired for liquid gastric emptying studies. A patient being fed via an enteric tube should be positioned with the left side down to prevent premature emptying of the stomach before the initial image can be acquired. After feeding is complete, the patient is positioned supine for imaging. Nasogastric tubes can be removed for imaging if the ordering provider so advises, as they may keep the cardiac sphincter open and potentially mimic gastroesophageal reflux. The image acquisition times of importance are the initial image after feeding (0 min) and the 1-h and 2-h images. If the ordering provider requests gastroesophageal reflux imaging, a 60-min dynamic protocol is applied to acquire images after the 0-min image and before the 1-h image. Dynamic acquisitions for reflux imaging use a 128 × 128 matrix and a 30-s frame time for 120 frames. Liquid gastric emptying studies can be completed if greater than 51% of gastric emptying is reached after 1 h of imaging. A 2-h posterior static image is acquired if 51% gastric emptying has not been achieved at 1 h.
Clear-Liquid Gastric Empty
Gastric emptying studies using clear liquid (i.e., water) may also be performed if patients cannot consume solid food, milk, or formula. There are some advantages to performing a gastric emptying study using only radiolabeled water. First, most pediatric patients do not have a problem drinking water. Second, the entire study is only 30 min (8). Third, adding an inpatient clear-liquid gastric emptying study to the daily workflow is much more feasible given that the length of the study is only 30 min. Clear-liquid gastric emptying studies are useful for evaluating gross gastroparesis. The main disadvantage is that clear-liquid studies do not provide specific details captured in a 4-h dual-phase or single-phase gastric emptying study.
The imaging protocol for a clear-liquid study begins with the patient drinking 237 mL (8 oz) of radiolabeled water. Anterior dynamic images are acquired using a 128 × 128 matrix at a rate of 1 min per frame for 30 frames. Conjugate views may be acquired; however, the processing program requires only the anterior view for the dynamic phase. At Children’s Cincinnati Hospital, a Xeleris workstation (GE Healthcare) is used to process dynamic images. The reference value for clear-liquid gastric emptying is a half-time of less than 25 min.
Patient Care Management
The results of the gastric emptying study can help guide therapy for patients with upper gastrointestinal symptoms, especially if they have delayed emptying (gastroparesis) or rapid emptying (dumping syndrome). Symptoms include nausea, vomiting, early satiety, postprandial fullness, and abdominal pain, which may be caused by gastric sensory or motor dysfunction or both (overlap).
With delayed gastric emptying or gastroparesis, the severity of the symptoms guides the level of supportive care that may be needed (9). Patients with grade 1 or mild gastroparesis have intermittent, easy-to-control symptoms and can maintain their weight and nutrition with dietary modifications such as low-fat small, frequent meals. Patients with grade 2 or compensated gastroparesis have partially controlled symptoms and benefit from pain control medications, antiemetics (ondansetron, promethazine, prochlorperazine, lorazepam), and prokinetics (erythromycin, prucalopride, metoclopramide, domperidone, cisapride) to improve their symptoms and avoid hospitalization. Although not a prokinetic agent, Cyproheptadine is widely used in clinical practice for dyspeptic symptoms and may have a role in alleviating symptoms of delayed gastric emptying because of its plausible effects on gastric accommodation.
Patients with grade 3 gastroparesis (gastric failure) respond less to dietary modification or medications, cannot maintain oral nutrition or hydration, and need frequent emergency room visits and hospital admissions; these patients may benefit from enteral tube feeds (gastrostomy tube or gastrostomy–jejunostomy tube), parenteral nutrition, endoscopic procedures (pyloric onabotulinumtoxinA [Botox; Allergan, Inc.] injection and dilation), surgical intervention (pyloroplasty and peroral pyloromyotomy), or neuromodulation (gastric electric stimulation) (10–12). Although the consensus recommendations for gastric emptying scintigraphy by the American Neurogastroenterology and Motility Society combined with the Society of Nuclear Medicine and Molecular Imaging are based on a standardized solid meal, dual-phase gastric emptying studies may help target therapy in dyspeptic children. A recent study showed that over half of children with dyspepsia had delayed liquid gastric emptying, and one quarter had delayed liquid emptying with normal solid emptying, highlighting the utility of dual-phase scans (11).
Rapid gastric emptying can be seen with iatrogenic dumping syndrome (after esophageal, gastric, or bariatric surgery, as well as in diabetes mellitus, autonomic neuropathy, postural orthostatic tachycardia syndrome, and disorders of gut–brain interaction [dyspepsia, cyclic vomiting syndrome]). Symptoms of rapid emptying or dumping include abdominal pain, bloating, borborygmi, nausea, and diarrhea, as well as vasomotor symptoms such as flushing, palpitations, perspiration, tachycardia, hypotension, fatigue, or syncope, and are attributed to osmotic effects, peptide hormone release, and autonomic neural responses. Treatment of dumping syndrome includes dietary modifications, pharmacologic interventions, surgical intervention, or continuous tube feeding. Dietary modification is usually beneficial for most patients and reduces the amount of food consumed at each meal. Acarbose (an α-glycosidase hydrolase inhibitor that decreases carbohydrate digestion in the small intestine and limits postprandial hyperglycemia and subsequent hypoglycemia), somatostatin analogs, diazoxide (a potassium channel activator that inhibits calcium-induced insulin release), and glucagonlike peptide 1 receptor antagonist exendin 9-39 (corrects hypoglycemia after gastric bypass) are some of the medications used in patients with rapid emptying. Maintaining the patient’s nutrition with gastrostomy or even jejunostomy feeds may be necessary (12).
CONCLUSION
At Cincinnati Children’s Hospital, performing gastric emptying studies for pediatric patients starts with a dual-phase gastric emptying study and branches off from there depending on what radiolabeled food the patient can consume for the study. Creating an environment of flexibility while simultaneously adhering to standardization is critical so that meaningful results can be reported to ordering providers. Treatment for patients with upper gastrointestinal symptoms can vary depending on the results provided by gastric emptying studies.
KEY POINTS
QUESTION: How are gastric emptying scans performed in pediatrics?
PERTINENT FINDINGS: This article discusses the possible variations from standardized protocols when gastric emptying scanning is performed in pediatrics. The scans may be performed as solid only, liquid only, or a dual phase that includes both solid and liquid emptying data.
IMPLICATIONS FOR PATIENT CARE: For patients with upper gastrointestinal symptoms, the results of gastric emptying scans can help guide therapy, which includes dietary modifications, pharmacologic interventions, surgical intervention, or continuous tube feeding.
DISCLOSURE
Joby MacLean is a consultant for GE Healthcare. No other potential conflict of interest relevant to this article was reported.
ACKNOWLEDGMENT
We thank Dr. Andrew Trout for reviewing the manuscript.
Footnotes
Published online Feb. 13, 2024.
REFERENCES
- Received for publication October 30, 2023.
- Revision received January 17, 2024.
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.