


Visual Abstract

Abstract
Metaiodobenzylguanidine (MIBG) imaging has been the standard for neuroblastoma staging for many decades. Novel agents such as 18F-DOPA and 68Ga-DOTATATE are being used nowadays in academic centers. During the coronavirus disease 2019 (COVID-19) pandemic, procurement of 123I-MIBG has proved particularly challenging, necessitating the use of 68Ga-DOTATATE PET. 68Ga-DOTATATE is Food and Drug Administration–approved for imaging of somatostatin receptor–positive gastroenteropancreatic neuroendocrine tumors. Methods: 68Ga-DOTATATE PET/CT imaging was performed for staging of 3 pediatric patients with neuroblastoma at our institution. A review of the literature was also completed. Results: 68Ga-DOTATATE PET/CT scans were successfully performed on all patients. All patients showed 68Ga-DOTATATE–avid disease. PET scans showed an excellent spatial resolution and demonstrated high accuracy in concordance with current European Association of Nuclear Medicine guidelines. Conclusion: We have presented 68Ga-DOTATATE PET/CT imaging for staging of neuroblastoma and believe it can reliably be used as an alternative to 123I-MIBG. It has technical, clinical, and practical advantages making it an attractive option. Further multicenter studies are required before it can be recommended for standard clinical use.
Neuroblastoma, the most common extracranial solid tumor in the pediatric age group, accounts for about 10% of all solid tumors. It varies in presentation from self-resolving disease to the highly malignant variant associated with an extremely poor prognosis. The staging evaluation of neuroblastoma requires both anatomic and nuclear medicine imaging to look for skeletal metastatic deposits (1,2). 123I-metaiodobenzylguanidine (MIBG) can be used for localization of neural crest tumors such as neuroblastoma, pheochromocytoma, and other neuroendocrine tumors. MIBG with 131I and more recently 123I has been the standard for neuroblastoma staging since its utility was first reported by Geatti et al. in 1985 (3,4).
The reported sensitivity and specificity of 123I-MIBG are approximately 90% (2,5). However, because 10% of neuroblastomas are not 123I-MIBG–avid, alternate imaging techniques have been investigated, including PET with 18F-FDG and 18F-DOPA, as well as PET/CT with DOTA-conjugated peptides such as 68Ga-DOTATATE. Early evidence suggests that these modalities may be superior in sensitivity and specificity to MIBG, thus having the potential of replacing MIBG (6–9).
Somatostatin receptors are variably expressed in neuroblastoma (10,11). Somatostatin analogs such as 68Ga-DOTATATE have been in clinical use for nearly a decade. Their role is most established in imaging and treatment of adult neuroendocrine tumors and pheochromocytoma but has also been studied in neuroblastoma in limited settings (7,8). 68Ga-DOTATATE PET has been studied at the time of recurrence and at the therapeutic planning phase within a theragnostic paradigm. However, there are very few reports of its role at diagnosis for staging (5,12).
Because MIBG production is limited globally, the severe acute respiratory syndrome coronavirus 2 (coronavirus disease 2019 [COVID-19]) pandemic has resulted in unacceptable delays in performing MIBG scans due to interruption in international air traffic. Its availability became particularly challenging at our institution, and we therefore decided to perform 68Ga-DOTATATE PET scans for 3 newly diagnosed patients with neuroblastoma. This PET agent is locally produced in a nearby center, obviating the delivery logistics. Here, we report our results and review the literature.
MATERIALS AND METHODS
At the beginning of the COVID 19 pandemic, 3 patients were diagnosed with neuroblastoma at Sidra Medicine. MIBG scintigraphy had to be cancelled for patient 1 when the radiopharmaceutical did not arrive on the scheduled date because of flight cancellations. In a discussion with the clinical team, we decided to perform 68Ga-DOTATATE PET/CT imaging instead. For subsequent patients, 68Ga-DOTATATE PET was done electively to avoid delays and hazards during the pandemic.
A local 68Ge/68Ga generator was used to produce 68Ga, which was used to radiolabel DOTATATE. Required quality control tests were performed before injecting the patient, in accordance with good manufacturing practices. After radiopharmaceutical injection, an uptake phase of 45–60 min took place before the patient was scanned. All 3 patients were scanned on a GE Healthcare Discovery 690 PET/CT scanner with an axial field of view of 15.7 cm. A low-dose CT scan (80 kVp, mA dose modulation, adaptive statistical iterative reconstruction, 0.5-s rotation time, 40-mm collimation) was performed for attenuation correction and anatomic localization, followed by a whole-body PET scan at 4 min per bed position with an 11-slice overlap. Images were reconstructed using a time-of-flight iterative reconstruction algorithm with a correction for point-spread function (VUE Point FX [GE Healthcare]: 2 iterations, 28 subsets), and a 3.4-mm postreconstruction gaussian filter. The final pixel size was 1.56 × 1.56 mm, with a slice thickness of 3.27 mm. All 3 patients were scanned under general anesthesia. The need for sedation was independent of the type of study, as the patients would have required general anesthesia for MIBG as well. The administered activities were weight-based according to the guidelines of the Society of Nuclear Medicine and Molecular Imaging and the European Association of Nuclear Medicine (74 MBq [2 mCi], 101.75 MBq [2.75 mCi], and 45.88 MBq [1.24 mCi] in the first, second, and third patients, respectively) (2).
RESULTS
Patient 1
A 23-mo-old boy presented with lower back pain, ataxia, and leg weakness for 5 d. Physical examination rapidly progressed from normal to lower-limb weakness and frank paraplegia. His work-up included an MRI scan showing a paravertebral mass at the level of the T2–T4 vertebrae, causing spinal cord compression and edema. He underwent emergency laminotomy and laminoplasty by the neurosurgeons and a debulking procedure resulting in return of lower-limb function over the next 48 h.
Patient 2
A 6-y-old girl presented with an intermittent limp over 2 mo. There were no other symptoms. On physical examination, she was unable to stand straight because of pain in the left leg and had mild tenderness on the left side of the abdomen. MRI of her abdomen and pelvis demonstrated a large mass in the left adrenal gland and numerous bony metastatic lesions.
Patient 3
A 3.5-y-old girl presented with weight loss, swelling of the left eye, body aches, and constitutional symptoms over several months. She was severely malnourished and had left-sided proptosis. MRI showed a right-sided adrenal mass, numerous liver metastases, and multiple vertebral lesions.
The clinical and imaging findings are summarized in Table 1, Supplemental Table 1, and Figures 1–4 (supplemental materials are available at http://jnmt.snmjournals.org).

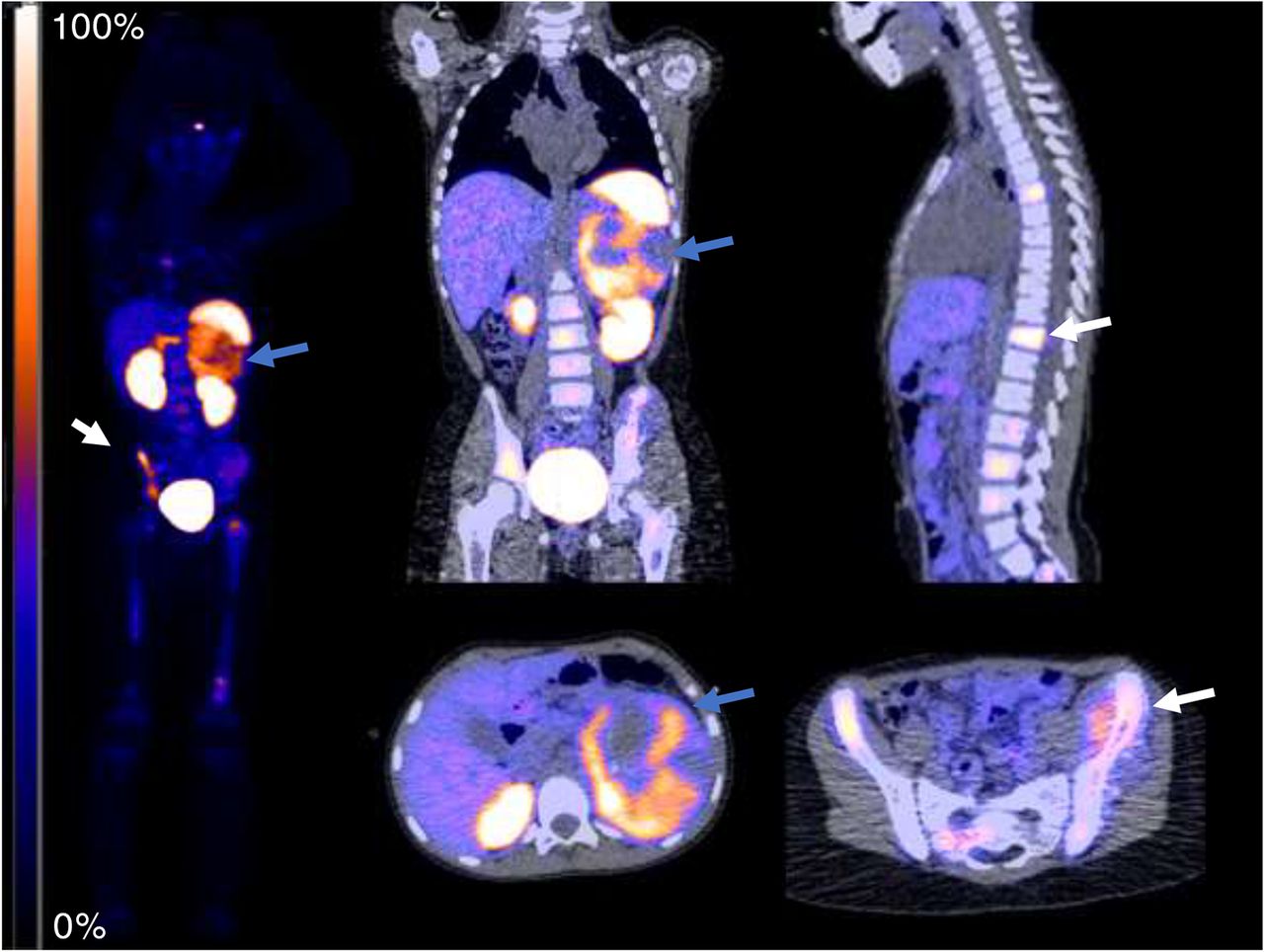
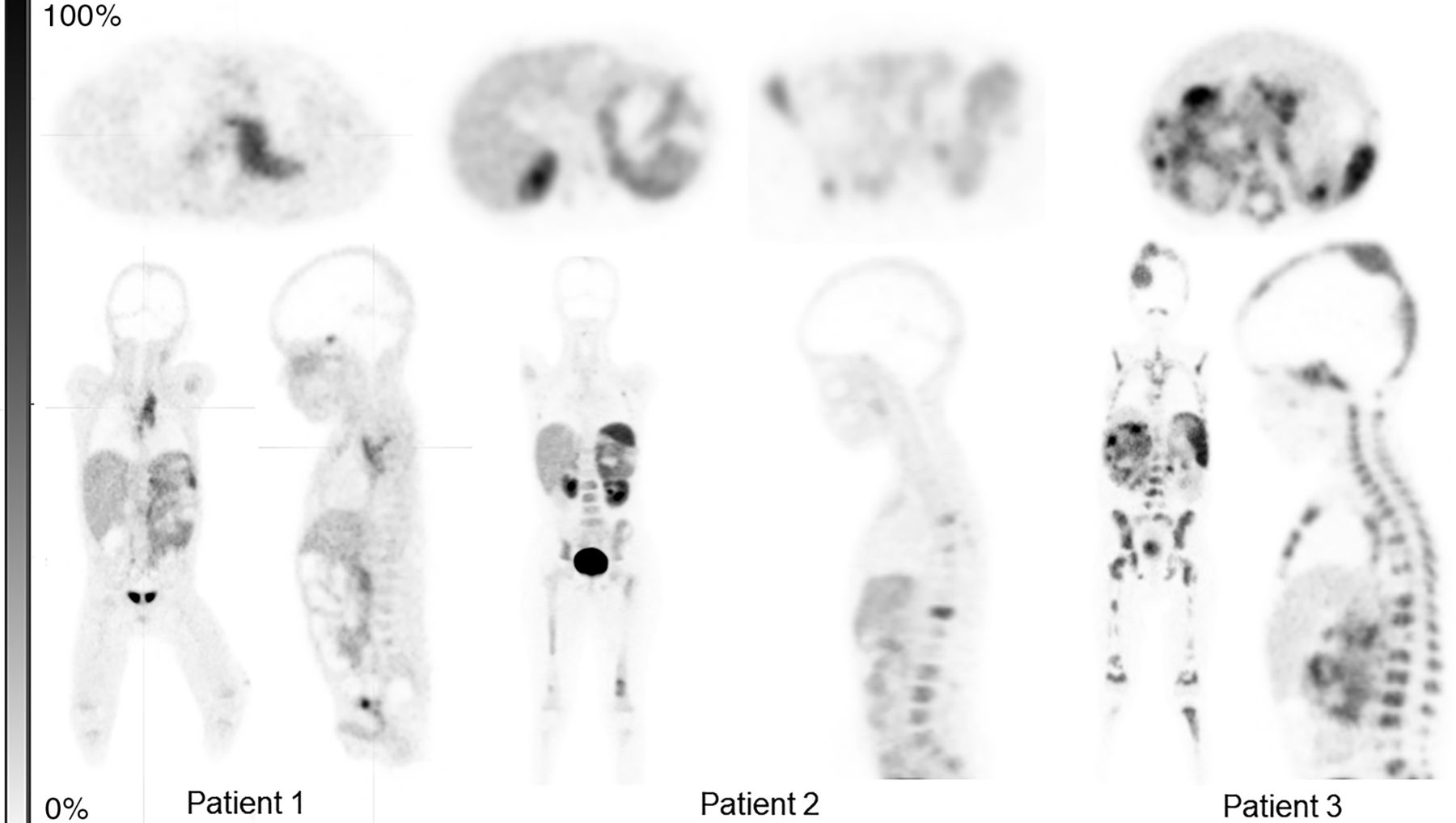
Increased uptake in left-sided paravertebral mass and invading the spinal canal and adjacent vertebral body of T3 (blue arrows).
Uptake in left suprarenal mass, with areas of necrosis (blue arrows) and evidence of skeletal metastasis (white arrows) and bone marrow infiltration.
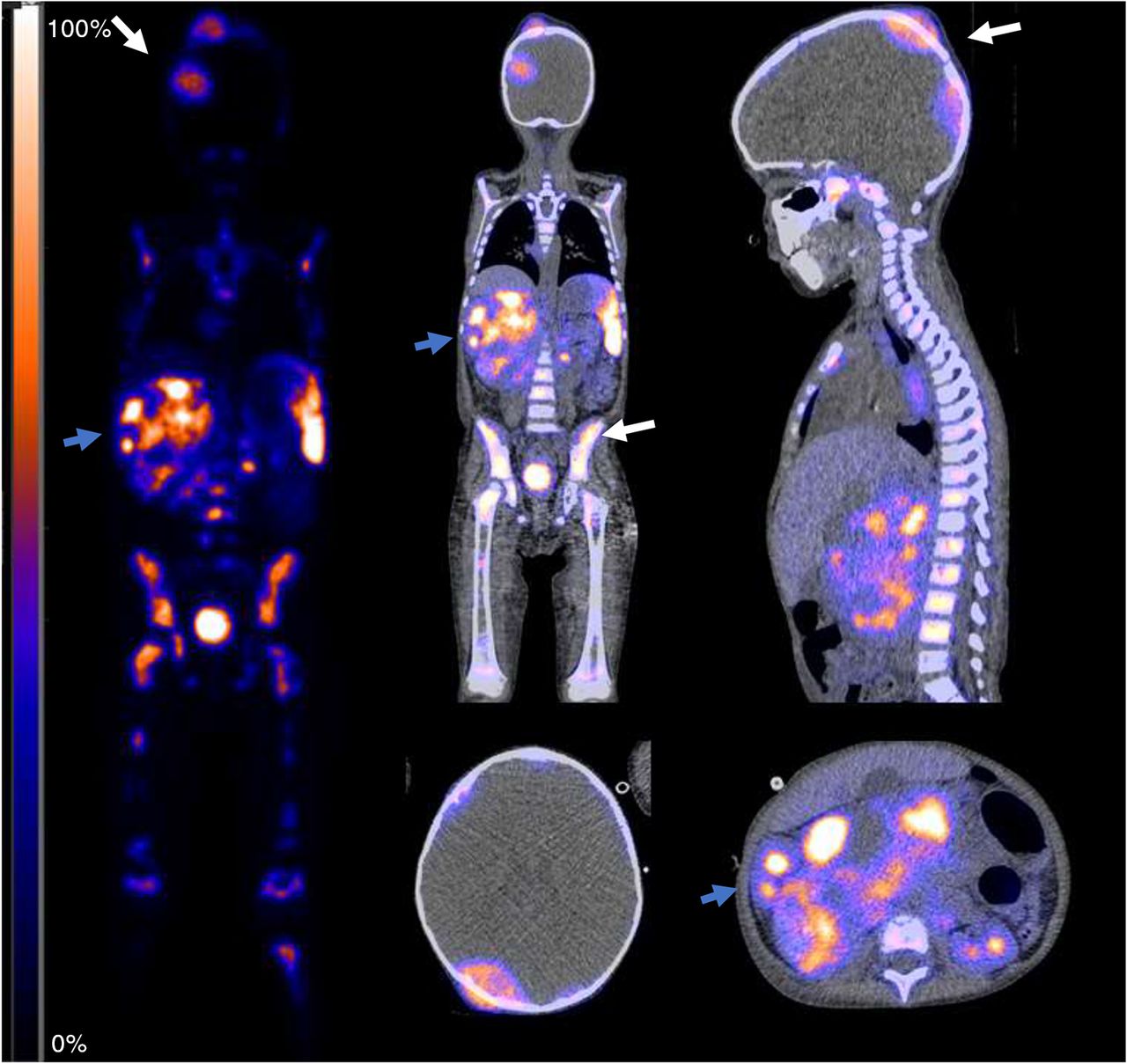
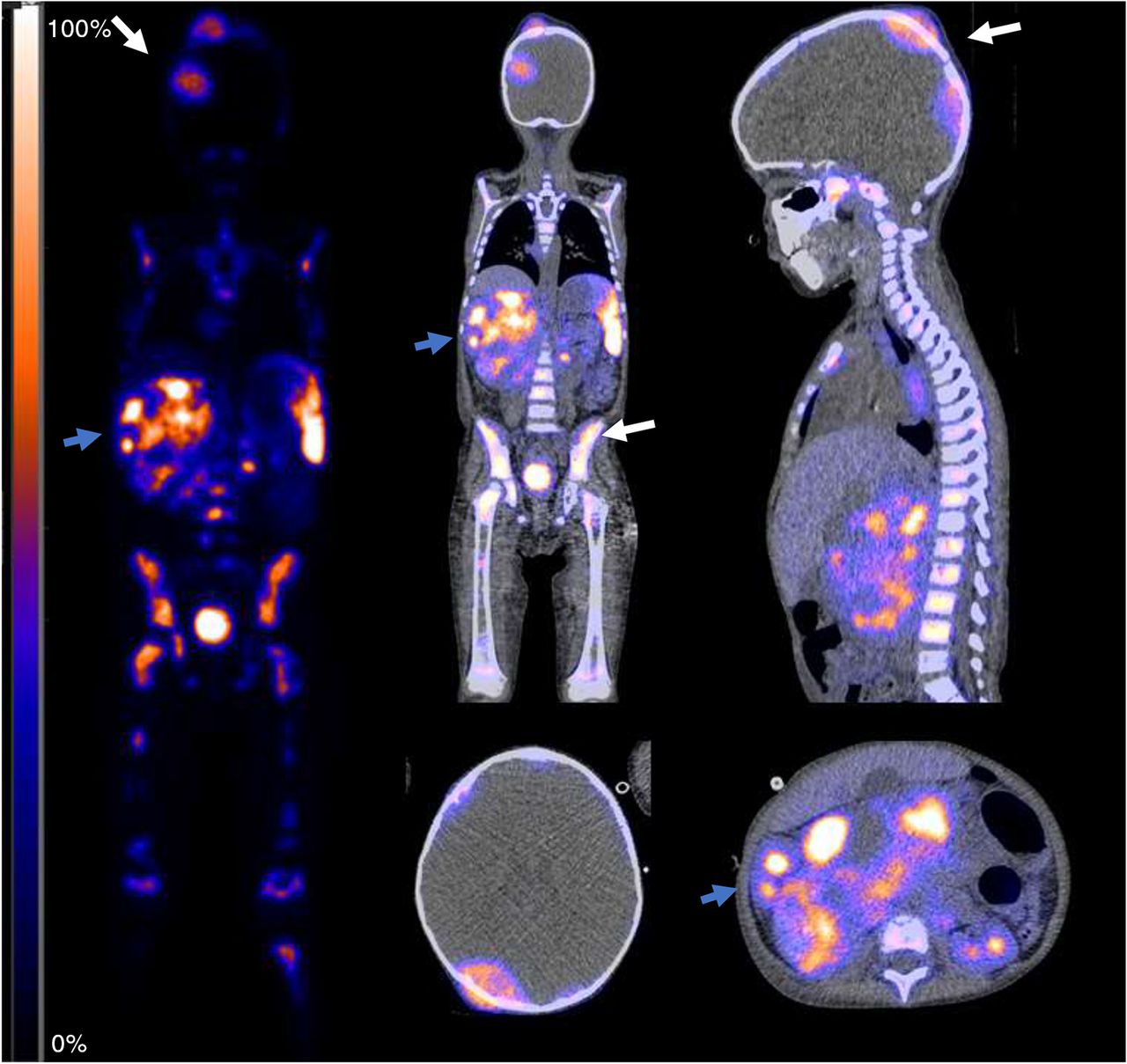
Heterogeneous uptake in lobulated right suprarenal mass (blue arrows), with diffuse skeletal metastasis, including in skull and pelvis (white arrows), and diffuse bone marrow infiltration.
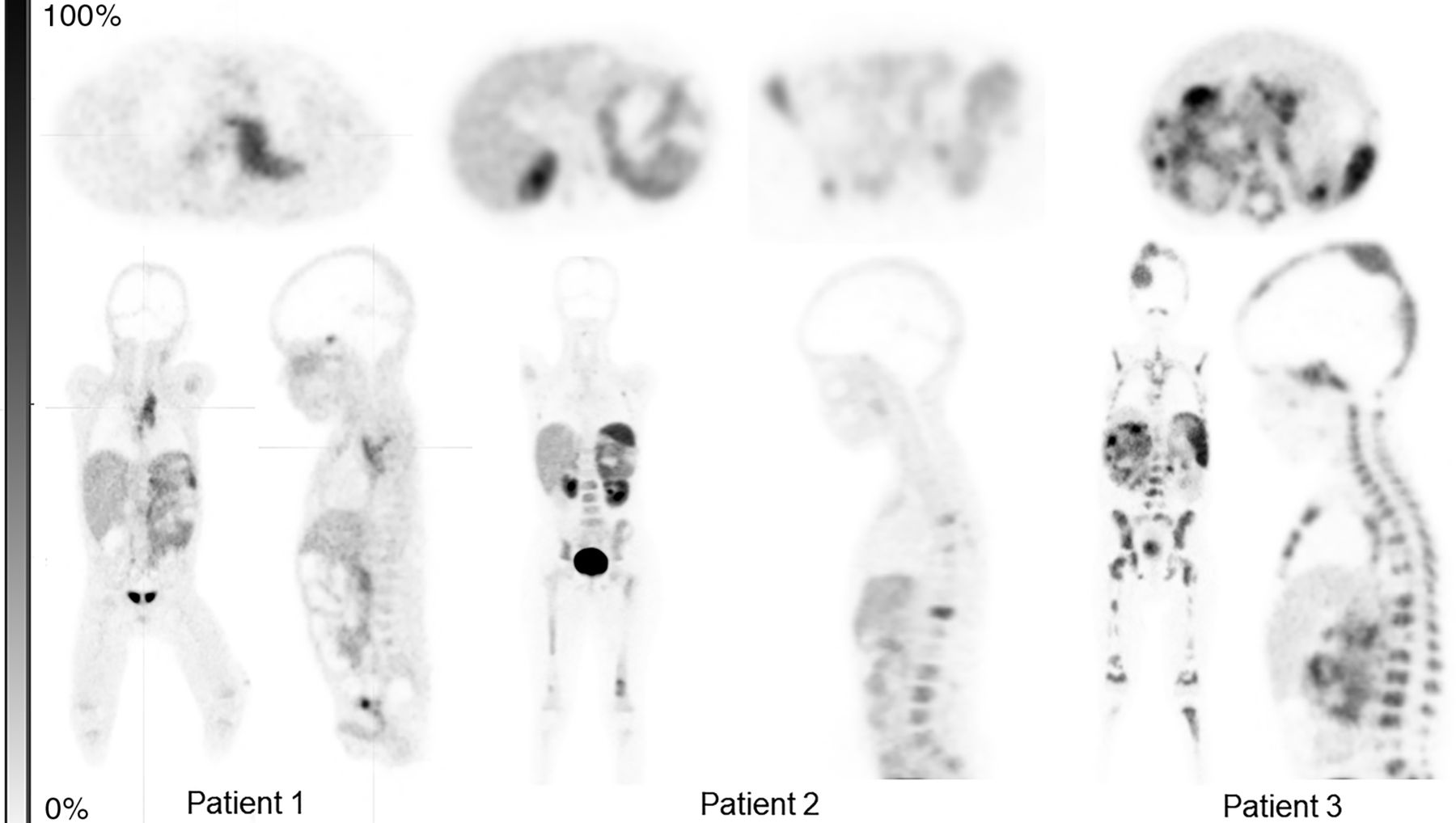
Summary of PET images for patients 1–3.
Patient Characteristics
DISCUSSION
The COVID-19 pandemic has posed many unanticipated and unprecedented health-care challenges worldwide, including challenges in the care of cancer patients (13). Before the pandemic, establishing a cancer diagnosis and performing the standard staging investigation were not seen to be a potential problem. Faced with the logistic difficulty of 123I-MIBG procurement, 68Ga-DOTATATE PET scans were performed in the light of limited but compelling evidence of their utility for initial staging of neuroblastoma. Our results will add to the evidence base for future studies.
68Ga-DOTATATE scans in our patients showed a high spatial resolution and high accuracy in concordance with reports in the literature (5,12,14).
In neuroblastoma management, the role of MIBG scintigraphy is established in staging, prognosis, and response evaluation (15,16). However, several logistic disadvantages make this form of imaging less attractive. These include a lengthy acquisition process, a protracted imaging schedule requiring repeated visits to the nuclear medicine department, and an occasional need for inpatient admission for younger patients. Another disadvantage is the need for thyroid blockade with Lugol solution, as MIBG can result in the accumulation of unbound iodine in the thyroid gland. Finally, MIBG uptake is affected by other medications affecting the sensitivity and accuracy of the study (17,18). On the other hand, 68Ga-DOTATATE can be produced locally using a generator and the patient is injected and imaged on the same day. No special preparation is required other than avoiding somatostatin analogs.
The role of 68Ga-DOTATATE PET has previously been studied at the time of recurrence and at the therapeutic planning phase within a theranostic paradigm. However, there are very few reports of its role for staging at diagnosis (5,12). Maurice et al. found that in their series of 15 adults with pheochromocytoma and paraganglioma, 68Ga-DOTATATE was positive in 5 patients in whom MIBG was negative, whereas the converse was true for only 2 patients (19). Similarly Naji et al. found that in adults with neural crest tumors, 68Ga-DOTATATE showed 10 of 12 lesions, versus 5 shown by MIBG (20). Krois et al. compared the sensitivity and specificity of 68Ga-DOTATATE with those of MIBG and morphologic imaging in their series of 11 patients (a mixed pediatric and adult cohort). Although only 5 of 11 patients had a diagnosis of neuroblastoma, 68Ga-DOTATATE had a sensitivity of 97%, versus 90% for MIBG (5). In a case report, Agrawal et al. reported the utility of 68Ga-DOTATATE PET/CT in diagnosis and response evaluation in a 12-y-old child with neuroblastoma (12).
All lesions evaluable on MRI scans were also avid on 68Ga-DOTATATE PET/CT imaging, affirming the hypothesis that it is highly sensitive for neuroblastoma.
The effective radiation doses for 123I-MIBG and 68Ga-DOTATATE are 0.013 mSv/MBq (0.481 mSv/mCi) and 0.021 mSv/MBq (0.777 mSv/mCi), respectively (21). Depending on the activity schedule for a 20-kg pediatric patient using the standardized European Association of Nuclear Medicine weight-based activity calculator (62 MBq [1.7 mCi] for 68Ga-DOTATATE and 136 MBq [3.7 mCi] for 123I MIBG), an approximately 25% lower radiation dose is possible with 68Ga-DOTATATE (14,21,22). Reducing the radiation exposure is especially relevant in low-stage tumors for which radionuclide therapy is not required.
Advantages of 68Ga-DOTATATE PET/CT include high image quality and better spatial resolution than with SPECT. Practical advantages also include more rapid imaging requiring less sedation, as well as no specific patient preparation requirements. Considering that 68Ga-DOTATATE has been Food and Drug Administration–approved for use with PET for localization of somatostatin receptor–positive neuroendocrine tumors in pediatric patients, and that it is relatively easy to acquire for clinical use, it should be considered for routine use in staging of neuroblastoma patients.
CONCLUSION
68Ga-DOTATATE PET/CT imaging can reliably be used as an alternative to MIBG for staging evaluation. It has numerous advantages over MIBG, including higher sensitivity, higher spatial resolution from PET, better image contrast, better tumor-to-background ratio, easier patient flow, easier patient preparation, and a more favorable dosimetry profile. Pooled data from multiple institutions may bring forth recommendations for its standard clinical use.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
ACKNOWLEDGMENTS
We thank Cyclomedica-HMC in facilitating the provision of 68Ga-DOTATATE and Dr. William Mifsud (pathology department at Sidra Medicine) for provision of histopathology images used in the graphical abstract.
Footnotes
Published online April 5, 2021.
REFERENCES
- Received for publication October 20, 2020.
- Accepted for publication February 16, 2021.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}