


Visual Abstract

Abstract
The aim of this study was to analyze the interobserver agreement of visual and quantitative assessment of cardiac 123I-metaiodobenzylguanidine scintigraphy. Methods: Planar images were acquired using a low-energy collimator. The heart-to-mediastinum (HM) ratio was adjusted for the use of a low-energy collimator, using a published formula. Interpretation was undertaken both visually and after the addition of adjusted HM ratios. Image findings were classified as normal, abnormal, or borderline. Results: The cohort consisted of 10 patients. On visual interpretation only, there was strong agreement on the interpretation of the scan (κ = 0.82, P < 0.01). Adjusted HM ratios led to a significant increase in mean ratios (1.79 vs. 1.36, P = 0.02) and, when utilized in reporting, resulted in perfect agreement (κ = 1.0, P < 0.01). Conclusion: The use of quantified HM ratios adjusted for low-energy collimator use improves on visual assessment alone and allowed for excellent interobserver agreement.
Sympathetic input, via noradrenaline, augments the function of the heart as part of the autonomic nervous system. Patients with Parkinson disease display altered noradrenergic function (1). 123I-metaiodobenzylguanidine (123I-MIBG) is a radioactive analog of noradrenaline, which localizes in the myocardial sympathetic nerve terminals and thereby allows this altered function to be imaged (2).
Myocardial sympathetic denervation on cardiac 123I-MIBG scintigraphy has shown great promise in the differential diagnosis of Parkinson disease (3,4) and is included in the Movement Disorder Society diagnostic criteria for Parkinson disease (5). A cardiac 123I-MIBG study can be assessed both visually and quantitatively. The type of quantitative data derived from this test is the heart-to-mediastinum (HM) ratio, which has been demonstrated to be significantly lower in patients with Parkinson disease than in patients with other Parkinsonian syndromes (6).
The use of a low-energy collimator for cardiac 123I-MIBG scintigraphy produces significantly lower HM ratios than those produced by a medium-energy collimator (7). However, correlation between the 2 methods is excellent, and the use of a simple formula allows for the conversion of HM ratios derived from a low-energy collimator cardiac 123I-MIBG study (8).
In the present study, we analyzed the interobserver agreement in the reporting of cardiac 123I-MIBG studies using visual interpretation and quantitative data with HM ratios. We hypothesized that the use of a low-energy collimator conversion formula to calculate adjusted HM ratios will lead to improved interobserver agreement.
MATERIALS AND METHODS
Study Design
A retrospective review was conducted of all patients who underwent cardiac 123I-MIBG scintigraphy at 2 nuclear medicine departments between 2015 and 2019. Patients who underwent the study for a nonneurologic indication were excluded. The institutional review board (Trust Audit Committee) approved this retrospective study, and the requirement to obtain informed consent was waived.
Technical Information
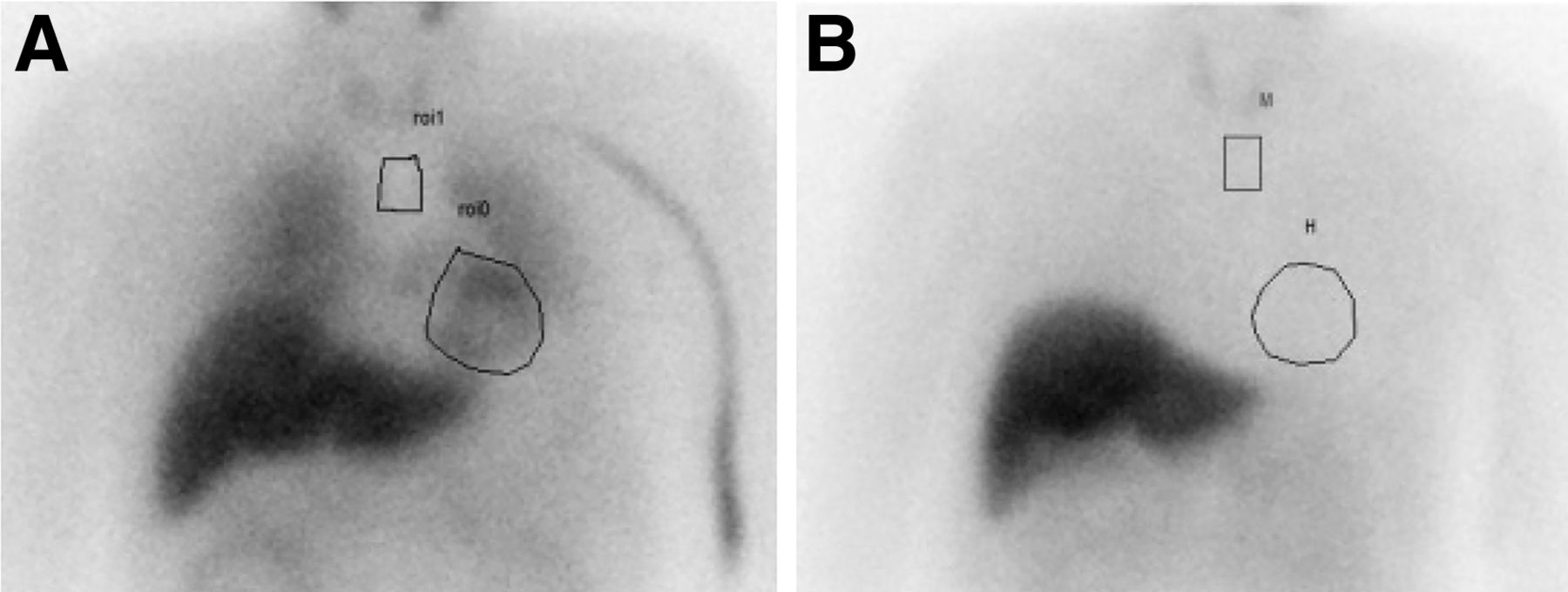
After intravenous injection of 100 MBq (2.7 mCi) of 123I-MIBG, planar images were acquired in the anterior view at both 15 min and 4 h using a dual-head Infinia γ-camera (GE Healthcare) and a low-energy collimator. Photopeak energy was centered on 159 keV with a 10% window and processed on Xeleris software (GE Healthcare). The HM ratio was measured by 2 consultant radiologists on the anterior planar images for image interpretation. A freehand region of interest was drawn around the left ventricle, and a small rectangular region of interest was drawn in the mediastinum, as per Kashihara et al. (6). The average counts in the left ventricular region of interest were divided by those in the mediastinal region of interest to calculate the HM ratio. Both the early-phase and the delayed-phase images were processed. Normal HM ratios may vary by patient population, and there are no clearly defined normal values for HM ratios using low-energy or medium-energy collimators. However, a normal HM ratio of more than 2.0 has been suggested for both the early and the delayed imaging (6,9), and it has also been demonstrated in healthy controls that a normal early HM ratio is more than 2.07 and a normal delayed HM ratio is more than 1.86 (10). We subsequently recalculated each patient’s HM ratio for a medium-energy collimator, using the following published formula: medium energy HM ratio = low-energy HM ratio/(0.41 − 0.63) (8).
Image Interpretation
Each 123I-MIBG study was visually interpreted by 2 radiology consultants without access to the patient’s HM ratio and masked to the clinical information for each patient. Interpretations were classified as normal, abnormal, or borderline for each patient (Fig. 1). Interpretation was then undertaken using the visual analysis and quantitative HM ratio data.
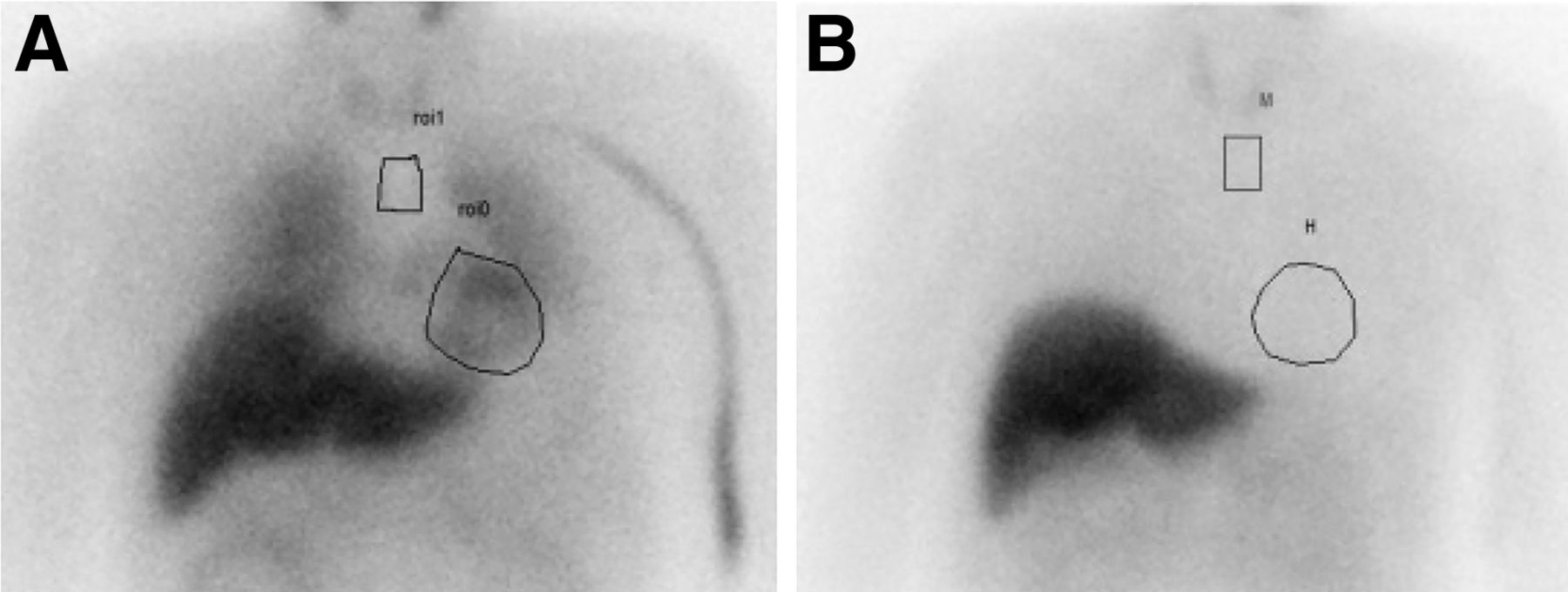
Cardiac 123I-MIBG scintigraphy interpreted as normal on visual assessment by both reporters (A), and study interpreted as abnormal by both reporters (B). HM ratios were 2.3 and 1.1, respectively, on delayed-phase images. H = heart; M = mediastinum; ROI = region of interest.
Statistical Analysis
Interobserver agreement was calculated using the Cohen κ. Interobserver agreement for the HM ratio measured by consultants, registrars, and technologists was performed via intraclass coefficient correlation analysis. The mean HM ratio with low-energy collimators and the mean HM ratio after adjustment with the medium-energy formula were compared using the paired t test. Statistical analysis was performed in R software, version 3.3.3.
RESULTS
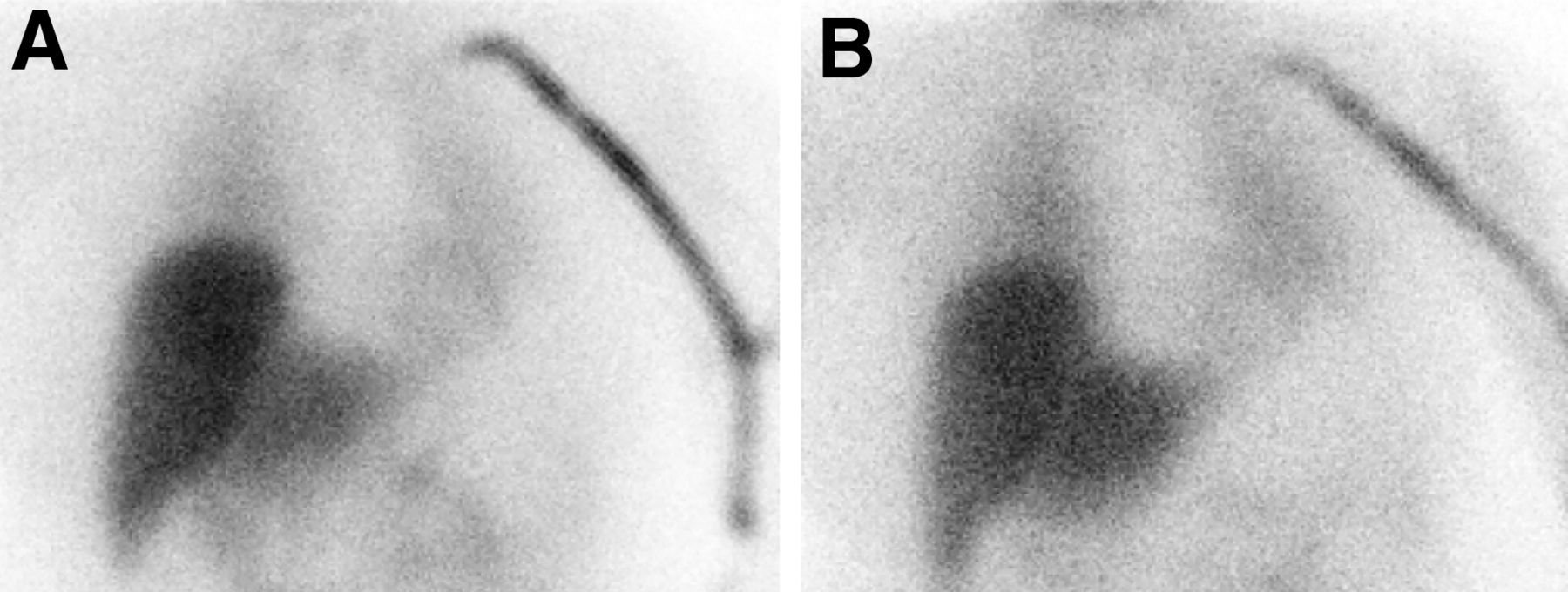
The cohort consisted of 10 consecutive patients, with an average age of 71 y. There were 7 men and 3 women. The clinical diagnoses were Parkinson disease (n = 7), multiple-system atrophy (n = 2), and dementia with Lewy bodies (n = 1). On visual interpretation of each patient’s cardiac 123I-MIBG study, there was strong agreement between the 2 reporters’ interpretation of the results (κ = 0.82; 95% CI, 0.510 –1.00; P < 0.01). There was disagreement about one patient (Fig. 2), for whom reporter 1 labeled the results as borderline whereas reporter 2 labeled them as abnormal (Table 1).

Early (A) and delayed (B) cardiac 123I-MIBG scintigraphy images interpreted as borderline by one reporter and abnormal by second reporter on visual assessment. After addition of HM ratios of 1.78 and 1.58, respectively, both reporters interpreted study as abnormal.
Visual Interpretation of Study Cohort
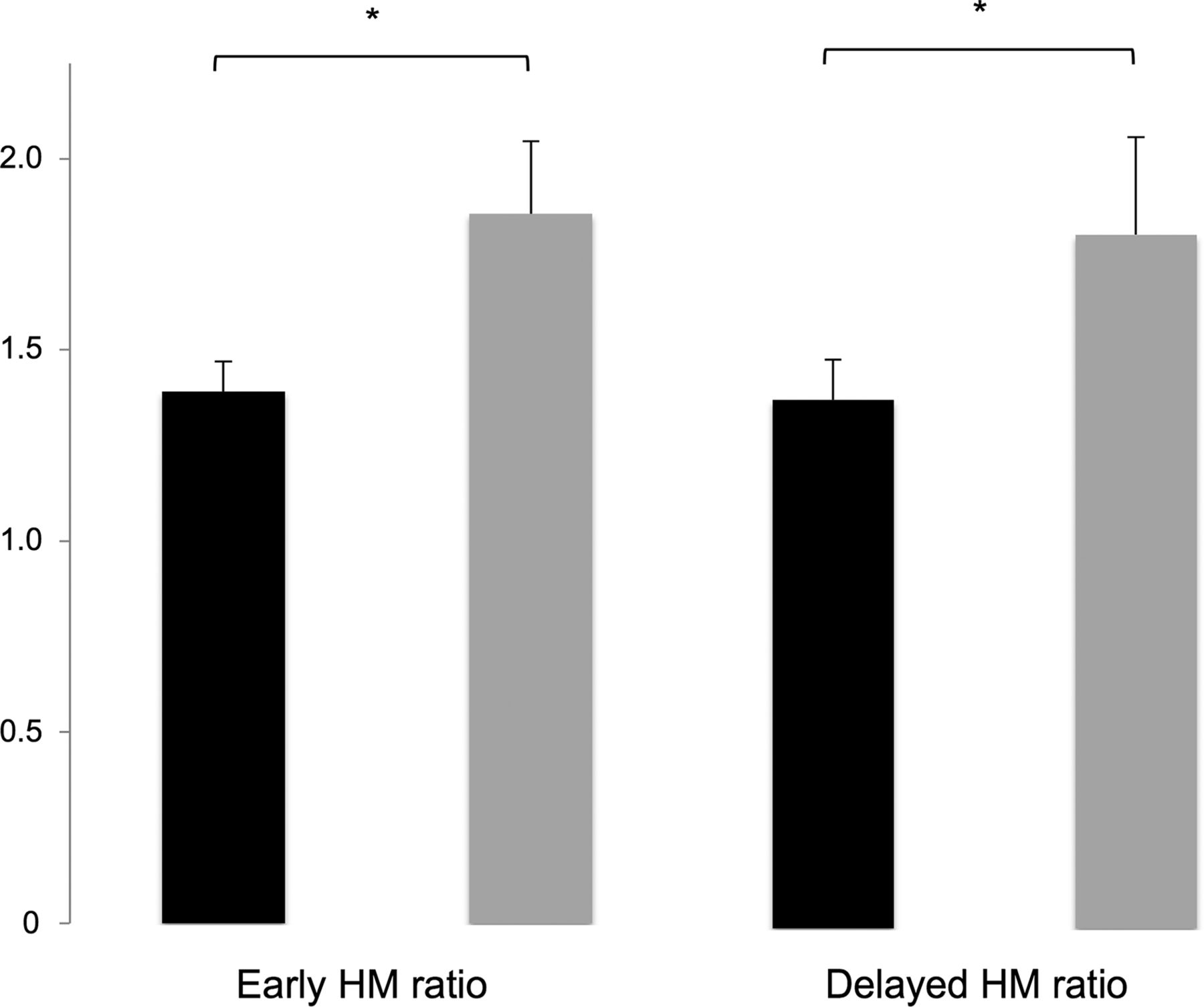
The mean HM ratio in this cohort was 1.36 using the low-energy collimators, whereas the mean HM ratio was 1.79 using the medium-energy conversion formula (Fig. 3). This was a statistically significant increase (P = 0.02). The interpretation of each cardiac 123I-MIBG study after the addition of the adjusted HM ratios led to perfect agreement between the 2 raters (κ = 1.0; 95% CI, 1.0–1.0; P < 0.01). The patient about whom there was disagreement on the visual assessment demonstrated an HM ratio of 1.78 on early imaging and a ratio of 1.58 on delayed imaging. This patient’s results were subsequently labeled as abnormal by both raters after the addition of the quantitative data to their interpretation.
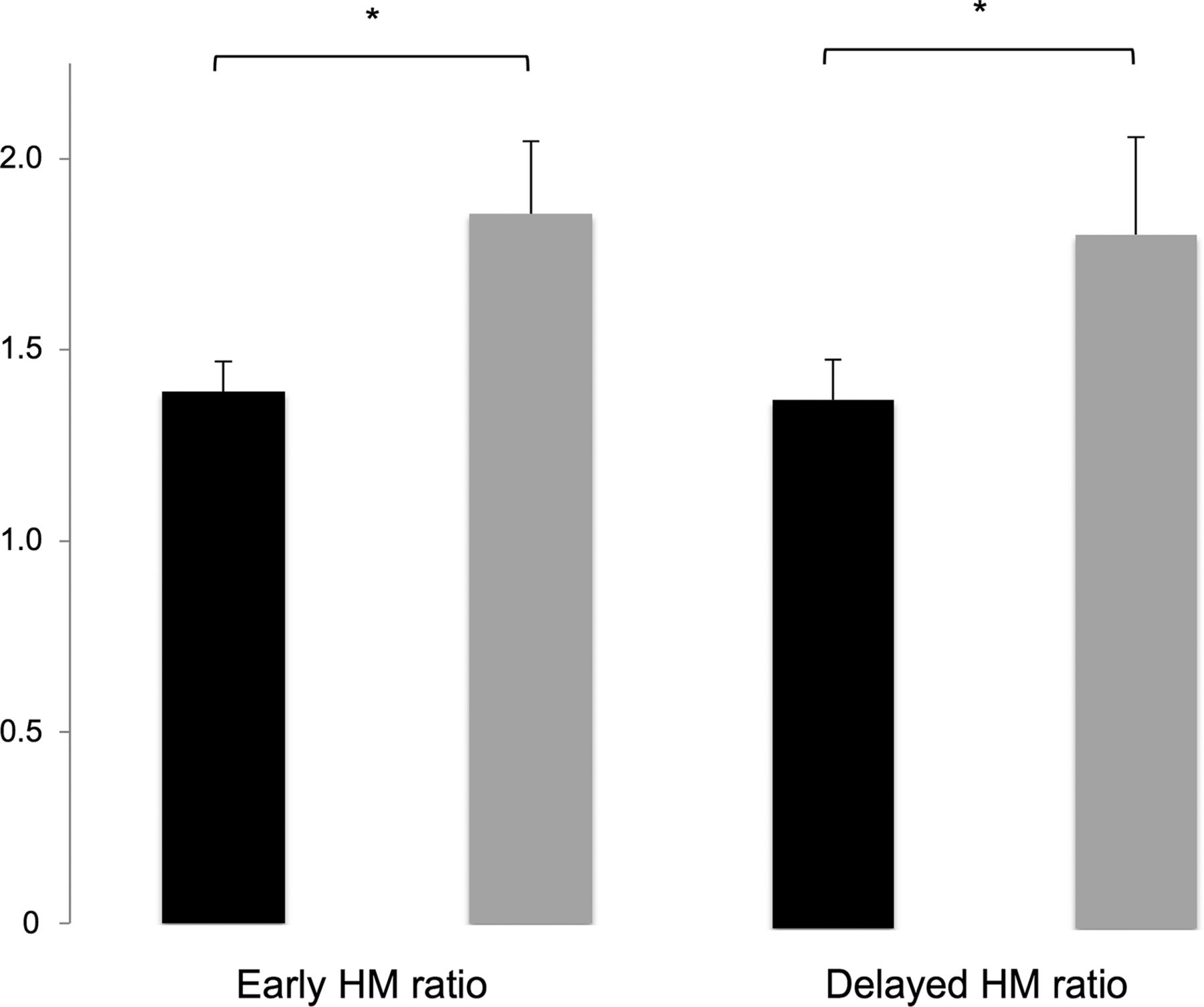
There was significant increase in average HM ratio, for both early-phase and delayed-phase imaging after application of linear conversion formula (medium-energy HM ratio = low-energy HM ratio/(0.41 − 0.63)). Original HM ratio is shown in black, with corrected HM ratio in gray. *P < 0.05.
DISCUSSION
The use of cardiac 123I-MIBG scintigraphy in the diagnostic pathway for patients under investigation for Parkinson disease has been well established in the literature. The gold standard for the diagnosis of Parkinson disease is a clinical one; however, in a systematic review of 2016, the overall accuracy of clinical diagnosis is approximately 80%–83% (11). Therefore, imaging retains a core role in attempts to improve this accuracy. Several studies have demonstrated significantly lower HM ratios on cardiac 123I-MIBG scintigraphy in patients with Parkinson disease (6,12) and in the other Lewy body diseases: dementia with Lewy bodies and pure autonomic failure (6,9,12,13). This finding is in contrast to various patient populations with a normal HM ratio, which includes healthy controls and patients with vascular parkinsonism, drug-induced parkinsonism and the Parkinson-plus syndromes, multiple-system atrophy, progressive supranuclear palsy, and corticobasal degeneration (6,9,12,13).
The results of the present study demonstrate that agreement between 2 experienced readers in the visual interpretation of cardiac 123I-MIBG is strong. The interobserver agreement is further improved by the addition of quantitative data in the form of the HM ratio. Previous research has demonstrated that visual interpretation of cardiac 123I-MIBG studies was equivalent to that of quantitative HM ratios (14,15). In the present study, we demonstrated that the use of quantitative methods in combination with visual assessment in the reporting of 123I-MIBG studies leads to improved agreement between reporters.
Some authors recommend the HM ratio as the primary method of interpretation (16), with visual assessment used as a secondary tool, particularly in borderline cases. This technique would require the normal and abnormal cutoffs for the HM ratio to be defined precisely at each center. However, this is clearly not the case, with normal values demonstrating wide ranges in the literature, varying from 1.38 to 1.94 for early imaging and from 1.34 to 2.40 for delayed imaging (3). Therefore, we recommend a reporting strategy that utilizes both visual interpretation and the quantitative HM ratio data in tandem when interpreting cardiac 123I-MIBG scintigraphy.
The present study utilized a low-energy, high-resolution collimator, as use of such a collimator was our practice for other 123I studies. Inoue et al. found that the average ratio in patients imaged with a medium-energy collimator was 2.66 ± 0.74, whereas the average ratio with a low-energy collimator was 1.81 ± 0.29 (P < 0.05) (7). Therefore, the use of a low-energy collimator makes comparison with established cutoffs in the literature difficult. We have demonstrated that the use of a low-energy collimator for cardiac 123I-MIBG studies can be adjusted via the formula derived by Brumberg et al. (8). If cardiac 123I-MIBG scintigraphy is performed using a low-energy collimator, this formula can be utilized to allow for meaningful comparisons of HM ratios with the published cutoffs in the literature. No such study comparing the clinical interpretation of cardiac 123I-MIBG studies acquired using a medium-energy and a low-energy collimator has been undertaken, and this is a potential area for future research.
We acknowledge several limitations to the present study. This was a relatively small patient cohort under investigation. However, we attempted to remedy this limitation by including 2 nuclear medicine centers. We did not attempt to quantify the overall accuracy of this test in the diagnosis of Parkinson disease. However, as previously discussed, there is myriad evidence for the utility of cardiac 123I-MIBG scintigraphy in the diagnostic pathway for patients under investigation for Parkinson disease.
The present study adds to the body of evidence surrounding the use of cardiac 123I-MIBG scintigraphy in 2 ways. First, we demonstrated that interobserver agreement is improved by the use of visual assessment and HM ratio data. We therefore recommend that a visual and quantitative assessment take place in tandem for the reporting of cardiac 123I-MIBG studies. Second, we demonstrated that the use of a low-energy collimator for cardiac 123I-MIBG studies can be adjusted via a published formula (8) to allow for comparisons with published HM ratios.
CONCLUSION
The use of HM ratios in cardiac 123I-MIBG scintigraphy, adjusted for low-energy collimator use, improves on visual assessment alone and allowed for excellent interobserver agreement in the present study.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online April 5, 2021.
REFERENCES
- Received for publication October 14, 2020.
- Accepted for publication March 12, 2021.





{kind=link}
{kind=link}
{kind=link}
{kind=link}