


Abstract
Myocardial perfusion imaging using radionuclides is a well-established protocol for determining the diagnosis, prognosis, and management of coronary artery disease. Pharmacologic stress agents are used to induce cardiac hyperemia in patients unable to achieve the target workload by physical exercise alone. The vasodilators adenosine and dipyridamole are most commonly used, with dobutamine used only when these agents are contraindicated. However, because of frequent and intense side effects, as well as complex procedures both for patients and the nuclear medicine staff, there is room for improvement in these traditional stress agents. An ideal stress agent would be effective, safe, and well tolerated; have a simple protocol; be suitable for use in patients with reactive airway disease; and have few restrictions for the patient to adhere to before the procedure. Neither adenosine nor dipyridamole are receptor-specific, and act on A1, A2A, A2B, and A3 adenosine receptors. As it is the A2A receptor that mediates the desired coronary vasodilation, the A1, A2B, and A3 adenosine receptors are deemed responsible for most side effects associated with adenosine and dipyridamole. A2A-selective pharmacologic stress agents should mediate the required hyperemic response while reducing the frequency of adverse events. The only selective A2A adenosine receptor agonist currently approved for clinical use as a pharmacologic stress agent for myocardial perfusion imaging is regadenoson. Regadenoson has demonstrated non-inferiority to adenosine for detecting reversible myocardial perfusion defects in phase 3 trials, and patients were more comfortable during the regadenoson stress procedure than during an adenosine infusion. As regadenoson dosing is not dependent on patient weight or renal impairment and can be administered by rapid injection, it has the potential to simplify the stress procedure, reduce costs, and streamline the working day for the staff of the nuclear medicine department. In this review, the need to improve on older pharmacologic stress agents will be considered, along with an assessment of how A2A receptor agonists fulfill that potential. Practical aspects of regadenoson are reviewed, and the impact that A2A receptor agonist use may have on the nuclear medicine department is evaluated.
Myocardial perfusion imaging (MPI) using radionuclides is a well-validated, noninvasive method to aid in the determination of diagnosis and prognosis for patients with suspected or known coronary artery disease. Myocardial blood flow during hyperemia is inversely related to coronary artery stenosis when the degree of stenosis is greater than 40% (1). Because of the inability of stenotic vessels to dilate, there is a disparity in flow between normal and diseased myocardium (2). Images of relative myocardial perfusion are obtained by PET or SPECT after radionuclide administration. Images obtained during myocardial hyperemia, induced by exercise or pharmacologic stress agents, are compared with images obtained at rest to determine the coronary flow reserve and identify areas of compromised myocardial perfusion.
The preferred modality for inducing hyperemia is physical exercise, because of the additional diagnostic information provided from the exercise tolerance of the patient and the hemodynamic response, heart rate recovery, and electrocardiographic changes during exercise (3). Pharmacologic stress agents are indicated for patients with medical conditions for which exercise stress is not suitable or is unsafe, or for those unable to achieve the cardiac workload necessary for optimal imaging (4,5). Pharmacologic stress MPI may therefore be more commonly used in patients who are elderly, debilitated, or morbidly obese; have musculoskeletal or neurologic limitations; or have severe pulmonary disease, peripheral vascular disease, artificial pacemakers and implantable cardioverter defibrillators, left bundle branch block, or underlying rhythm disturbances (3). Adequate exercise is dependent on the patient's achieving at least 85% of the age-adjusted maximal predicted heart rate (220 beats per minute minus patient age), a workload of more than 5 metabolic equivalents, and at least 3 min of exercise to completion of stage 1 of the standard Bruce protocol (6,7). An inability to achieve these targets is often the case in patients who are older, have noncardiac physical limitations, take concomitant medications, or lack the necessary motivation (7).
Approximately 8.5 million stress MPI studies are performed yearly in the United States, of which around 40% use vasodilator pharmacologic stress agents (8). Furthermore, the use of pharmacologic stress agents or a combination of pharmacologic stress and low-level exercise is increasing (9,10). In the future, the number of stress MPI studies is expected to rise as the population ages and the prevalence of cardiovascular risk factors, such as obesity and diabetes, increases.
The aim of this article is to provide an overview of pharmacologic stress agents, focusing on regadenoson, the first A2A receptor agonist approved by the U.S. Food and Drug Administration for use as a pharmacologic stress agent in MPI. The available data for regadenoson are reviewed, with particular emphasis on the practical aspects that are relevant to nuclear medicine staff. The impact of the use of such A2A-selective agonists on patients, staff, and nuclear medicine departments as a whole is considered.
PHARMACOLOGIC STRESS AGENTS
Most pharmacologic stress MPI procedures use the vasodilators adenosine or dipyridamole, with the catecholamine dobutamine used when vasodilators are contraindicated. Definitions of common pharmacologic terms used in this article can be found in Table 1.
Definitions of Common Pharmacologic Terms
Adenosine induces hyperemic coronary flow to the heart by stimulating the A2A adenosine receptors on the smooth muscle cells of coronary vessels, which causes their dilation (11). Dipyridamole indirectly activates the same pathway by inhibiting the cellular uptake of adenosine and, consequently, increasing its interstitial concentrations. The excess adenosine nonselectively activates all adenosine receptor subtypes, including the A2A receptors, resulting in vasodilation. Because diseased vessels cannot dilate, images of relative myocardial perfusion can identify stenoses.
Up to 80% of patients experience side effects resulting from the use of adenosine or dipyridamole for pharmacologic stress MPI (12–16). Most of these side effects are mild and include flushing, chest pain, dyspnea, dizziness, and nausea. These frequent side effects, although not serious, are uncomfortable for the patient and create a need for increased monitoring time and care by the nuclear medicine staff. More serious events, including bronchospasm, atrioventricular block, and peripheral vasodilation (resulting in hypotension), are observed with lower frequency (7,12,14–16). Patients with asthma and chronic obstructive pulmonary disease (COPD) are at increased risk of bronchoconstriction and respiratory problems resulting from the use of adenosine or dipyridamole (7,17,18). The use of dipyridamole-containing medications and the adenosine receptor antagonists aminophylline, theophylline, and caffeine are heavily restricted before the procedure (7). The dose of adenosine or dipyridamole is adjusted according to patient weight and administered by infusion over several minutes, with vital signs and side effects monitored during the infusion (7,9). Both agents cause a 4- to 4.5-fold increase in coronary blood flow (19), which is higher than ideal because of the nonlinear uptake of the radionuclides at higher myocardial flow rates (20). The half-life of adenosine is extremely short (<10 s), whereas the half-life of dipyridamole is approximately 30–45 min (7).
Dobutamine primarily stimulates β1-adrenergic receptors, causing an increase in heart rate, blood pressure, and myocardial contractility and, therefore, an increased myocardial oxygen demand and consequent hyperemia. Side effects observed during dobutamine stress are similar in frequency to those observed for adenosine and dipyridamole and include palpitations, chest pain, headache, flushing, arrhythmias, and ST-segment depression. Dobutamine stress is contraindicated in patients taking β-blockers and is not recommended for patients with asthma and COPD (7). The half-life of dobutamine is around 2 min (7).
Adenosine, dipyridamole, and dobutamine all exhibit unfavorable side effect profiles, have common medical and drug contraindications, and have procedures that are inconvenient and challenging for both the patient and the staff, requiring many resources. A theoretic ideal pharmacologic stress agent would induce a 2- to 3-fold increase in coronary blood flow rapidly after administration. This increase would return to baseline soon afterward yet would be maintained long enough to allow the radiopharmaceutical to concentrate adequately in the myocardium and represent the true distribution of ischemia. Additionally, a longer hyperemic response would permit administration by rapid injection, rather than by the constant infusion required for adenosine, dipyridamole, and dobutamine (21). An ideal agent could be used in patients for whom current agents are unsuitable, such as patients who have contraindicated medical conditions or cannot safely discontinue any concomitant medications that may interfere with the MPI study. It would also be preferable if the stress agent did not require dose adjustment according to patient weight or renal status. If these ideal characteristics were realized, pharmacologic stress MPI procedures would be better tolerated and simpler for the patient while being faster, easier, and more accurate for nuclear medicine staff. From a cost perspective, fewer ancillary items, such as microbore tubing and large-volume syringes, would be necessary for a rapid injection than for a constant infusion. In addition, there would be no need for infusion pumps, thus reducing the cost and the possibility that an incorrect pump setup might result in dosing errors. If prefilled syringes were available, which is possible only for an agent that does not require dose adjustment, there would also be no dose wastage when procedures are delayed or cancelled. Furthermore, as the U.S. Pharmacopoeia chapter 797 (a federal act that mandates changes in how pharmaceuticals are drawn up, stored, and handled) is implemented at the state level, the practice of nuclear medicine departments performing MPI procedures will be affected. Moving forward, it is likely that agents that facilitate compliance with these higher standards will be favored.
A2A RECEPTOR AGONISTS
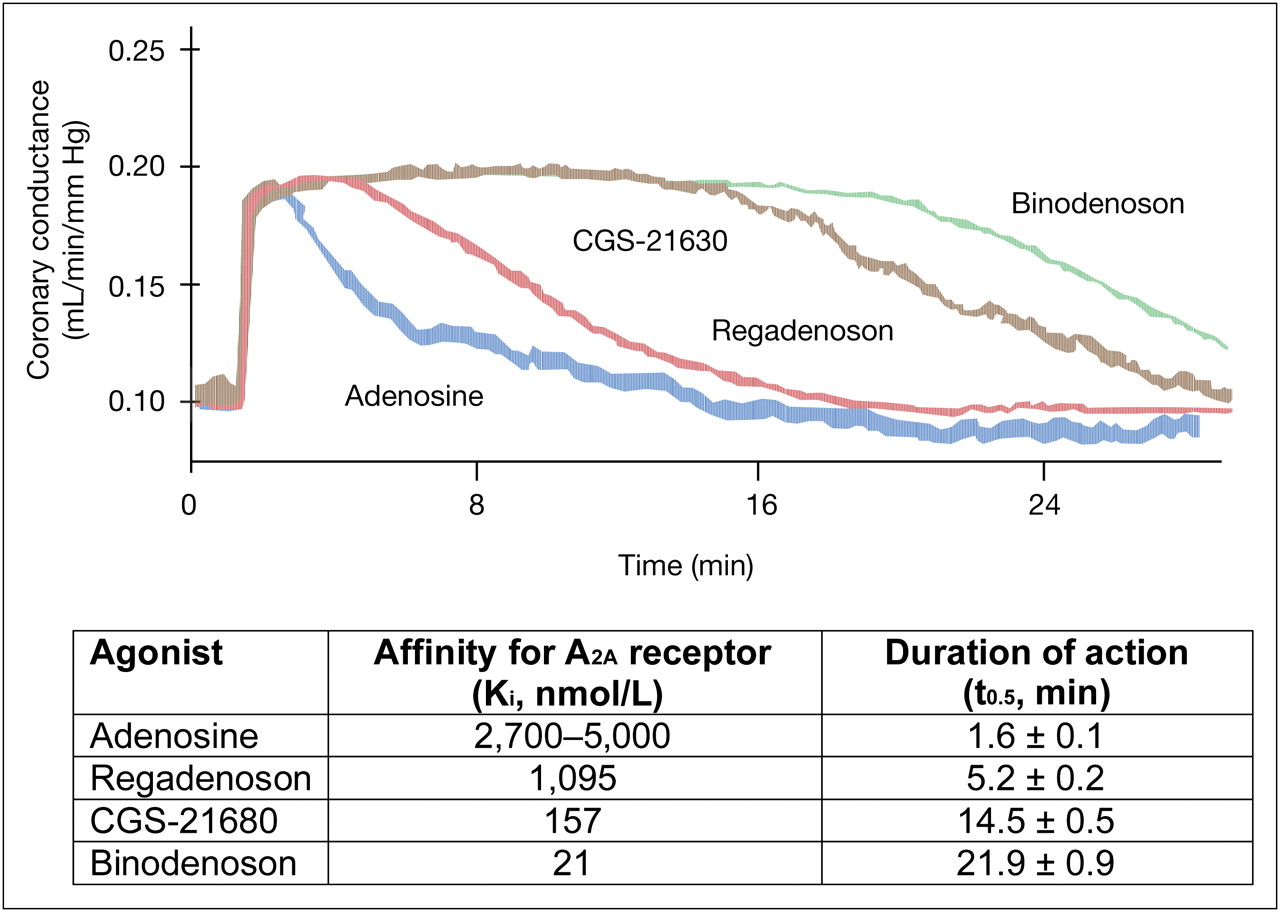
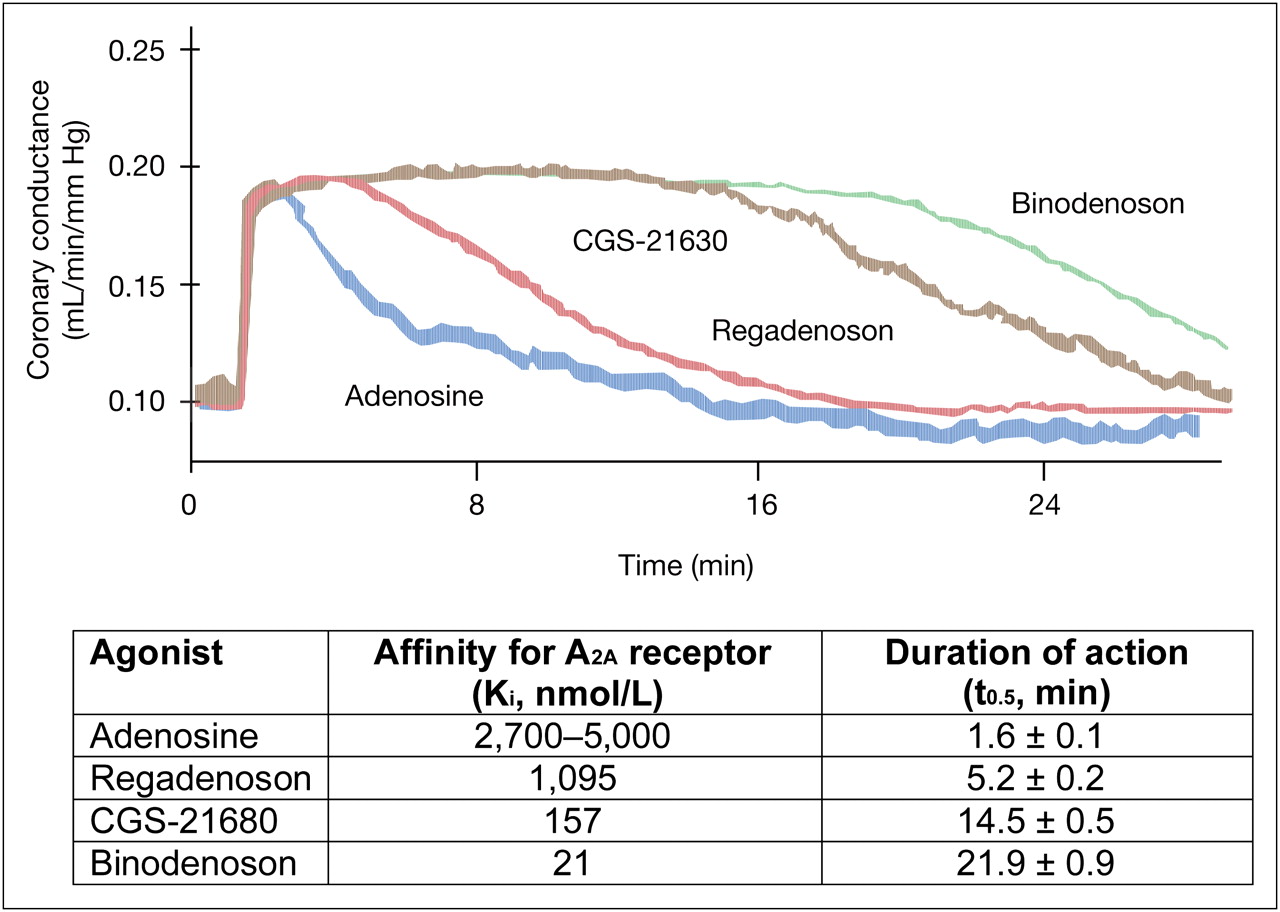
A2A receptor stimulation causes the desired coronary vasodilation to induce the myocardial hyperemia required for MPI (11), whereas the nonselective action of adenosine and dipyridamole on the A1, A2B, and A3 receptors is deemed predominantly responsible for the side effects associated with these agents (22,23). Of particular interest are the less frequent but more serious adverse events, including bronchospasm (mediated by the A1, A2B, and A3 receptors), atrioventricular block (A1 receptor), and peripheral vasodilation (A2B receptor) resulting in hypotension (7,12,14–18,21–24). More selective A2A receptor agonists have the potential to mediate the desired level of hyperemia while reducing the frequency of adverse effects (21). Regadenoson, binodenoson, apadenoson, and 2-p-(2-carboxyethyl) phenethylamino-5′-N-ethylcarboxamido adenosine (CGS-21680) represent a new generation of such A2A receptor agonists. Regadenoson is, so far, the only agent approved by the Food and Drug Administration for clinical use. Apadenoson and CGS-21680 have been investigated in preclinical trials. To date, there are limited data published for binodenoson (25–30) and even fewer for apadenoson and CGS-21680 (31,32).
In clinical studies, regadenoson and binodenoson appear to provide diagnostic information comparable to that of adenosine while having improved side effect profiles. In a dose-ranging study of binodenoson, side effects were generally milder and were reported less frequently in patients randomized to receive binodenoson than in those who received adenosine, and second- or third-degree atrioventricular block was observed in 3% of patients who were administered adenosine but in none of the patients who received binodenoson (28). Two randomized, double-blind, crossover phase 3 trials (Vasodilator-Induced Stress In cONcordance with Adenosine (VISION) trials 302 and 305) have been completed with binodenoson (33), and a New Drug Application was submitted to the Food and Drug Administration in December 2008.
As yet, there are no studies comparing regadenoson and binodenoson directly, and the differences between the study designs in the data published so far make comparisons difficult. Initial results indicate that the use of A2A-selective agonists for pharmacologic stress MPI reduces the frequency and severity of side effects for the patient undergoing the procedure.
REGADENOSON
In vitro studies have demonstrated that regadenoson is a full agonist as a coronary vasodilator and is 10-fold more potent than adenosine at increasing coronary conductance (34). The selectivity of regadenoson for the A2A receptor was also demonstrated, with regadenoson having a 13-fold lower affinity for the A1 receptor than for the A2A receptor and little or no interaction with the A2B or A3 receptor (34).
As there is a large receptor reserve for A2A-mediated coronary vasodilation, low-affinity agonists have the potential to elicit large-scale, but rapidly terminating, vasodilation with increased specificity for coronary vessels (34,35). It has been shown that the duration of the vasodilatory response is inversely related to the affinity of the agonist to the A2A receptor (34). Regadenoson has a much lower affinity than binodenoson or CGS-21680 for the A2A receptor but a higher affinity than adenosine (Fig. 1). In human patients, a rapid dose of regadenoson mediated an increase in coronary blood flow of 2.5-fold or greater for 2–3 min (36). This is close to the theoretic ideal response for an MPI stress agent and enables regadenoson to be administered by a single rapid injection (21). In a study of 16 patients with varying degrees of renal function, it was demonstrated that regadenoson does not require dose adjustment according to the renal function of the patient (37). Although the effective half-life of regadenoson was increased with decreased renal function, the maximum plasma concentrations and the pharmacokinetic parameters associated with distribution showed only minor differences between treatment groups, and the plasma concentration–time profiles were not significantly altered early after dosing (38). Additionally, the regadenoson dose does not need to be adjusted according to patient weight.
Initial studies of regadenoson in humans were positive, demonstrating that a rapid (over 10 s) intravenous injection of regadenoson was well tolerated, with no serious side effects observed. However, these initial studies were small and not powered to investigate the clinical efficacy of regadenoson versus adenosine (36–39).
The aim of the Adenoscan Versus Regadenoson Comparative Evaluation for Myocardial Perfusion Imaging (ADVANCE MPI) 1 and 2 trials was to demonstrate the non-inferiority of regadenoson, compared with adenosine, by examining the concordance of images detecting reversible myocardial perfusion defects (40,41). ADVANCE MPI 1 and 2 were methodologically identical, double-blind, randomized, active-comparator, double-dummy, multicenter, phase 3 trials. The results of ADVANCE MPI 2 have been published (40), together with a combined analysis of the results of the 2 trials (41).
Patients older than 18 y who had been referred for pharmacologic stress SPECT MPI were eligible for inclusion in the ADVANCE MPI trials (40). All patients first underwent an initial adenosine study and were then randomized 2:1 to a second study using regadenoson or adenosine. In the combined ADVANCE MPI 1 and 2 efficacy population, 1,240 patients received regadenoson and 631 patients received adenosine. All MPI procedures were performed according to the American Society of Nuclear Cardiology guidelines (42). Detailed methods are available in the original publications and are summarized here (40,41). Three expert readers independently scored blinded images, and reversible myocardial perfusion defects were identified and categorized as none to minimal, small to moderate, or large. The overall diagnosis and image quality was also assessed by each reader.
The agreement rates between the initial adenosine procedure and the second randomized procedure with either adenosine or regadenoson were almost identical. The interpretation agreement rate ranged from approximately 50% in patients with a small to moderate or large extent of ischemia to approximately 85% in patients with no or minimal ischemia (Fig. 2). Age, sex, body mass index, or diabetes mellitus did not affect the agreement rates (41). Overall, 92% of images were rated as good or excellent for both agents. Thus, in the ADVANCE MPI trials, regadenoson achieved non-inferiority to adenosine for pharmacologic stress MPI.

Agreement rates of adenosine–adenosine and adenosine–regadenoson stress MPI studies with respect to extent of ischemia in combined ADVANCE MPI 1 and 2 study population (41). Data are median ± SE.
Hemodynamic evaluations performed in the ADVANCE MPI trials showed that regadenoson caused a more rapid and greater peak increase in heart rate than did adenosine and that heart rate returned to baseline more slowly in the patients administered regadenoson. Systolic and diastolic blood pressure decreased by a similar extent with both agents, but hemodynamic recovery was more rapid for patients who received adenosine than for those who received regadenoson (40).
Side effects were rated as mild, moderate, or severe. As a measure of tolerability, patients were asked to rate how they felt during the procedure. Additionally, patients were asked to compare the initial study (adenosine) with the second procedure (adenosine or regadenoson). In both the ADVANCE MPI 2 analysis and the combined analysis, patients who received regadenoson had a lower side effect symptom score for the prespecified combination of the most common side effects (chest pain, dyspnea, and flushing), which remained lower for regadenoson when all symptoms were included (40,41). Headache and gastrointestinal discomfort were observed more frequently in the regadenoson group. This complaint has also been observed in postmarketing experience and is discussed in more detail below.
In the combined ADVANCE MPI 1 and 2 populations, first-degree atrioventricular block was observed in 2.8% (n = 34) of patients who received regadenoson, compared with 7.0% (n = 43) of those who received adenosine, and second-degree atrioventricular block was observed in 0.1% (n = 1) of patients who received regadenoson, compared with 1.5% (n = 9) of those who received adenosine (P = 0.001) (41). There were no instances of third-degree atrioventricular block. However, by study design, patients with a history of high-degree atrioventricular block or those who experienced atrioventricular block during the initial adenosine stress procedure were not randomized to the second procedure. The reduced incidence of atrioventricular block with regadenoson, compared with adenosine, is attributed to the reduced affinity of regadenoson for the A1 receptor. Patients who received regadenoson were more comfortable, and when questioned if they preferred the first (adenosine) or second (adenosine or regadenoson) procedure, 62% of patients randomized to receive regadenoson preferred the second procedure, compared with 43% of patients who were randomized to receive a second adenosine procedure. The high number of patients who preferred the second adenosine test is attributed to their being more prepared for the procedure and side effects the second time around (40).
These studies demonstrated that regadenoson was non-inferior for detecting reversible myocardial perfusion defects while being better tolerated than adenosine. The A2A specificity of regadenoson does not completely eradicate the side effects that were thought to be solely determined by adenosine receptor types other than A2A. The authors hypothesized that side effects such as chest pain and dyspnea, thought to be the result of A1 receptor stimulation, may be a consequence of sympathetic stimulation (40).
PRACTICAL ASPECTS
The improved tolerability and reduction in the number of serious adverse events together with similar clinical efficacy, compared with adenosine in the ADVANCE MPI trials, indicates that regadenoson represents an improvement over traditional pharmacologic stress agents.
The Nuclear Medicine Service of the VA San Diego Healthcare System has performed approximately 2,000 MPI procedures using regadenoson since 2008. In our clinical experience, the incidence of gastrointestinal discomfort and persistent headache appears to be higher for regadenoson than for adenosine. In most patients, headaches seem to be alleviated by intake of caffeine after the stress procedure. Nausea and vomiting, although infrequent, may occur shortly after the injection of regadenoson and are usually resolved by 3–4 min after administration. Discussions with other facilities using regadenoson have raised speculation as to the cause of these side effects; some believe that the vomiting may be due to stimulation of A2A receptors in the stomach, whereas others believe that it may be related to consumption of water before the stress procedure. In some nuclear medicine departments, patients are given water before the acquisition of images at rest to prevent gut activity from interfering with the imaging. If the stress procedure is performed on the same day as the rest scan, the patient's stomach may be full, which may be partly responsible for the nausea and vomiting observed.
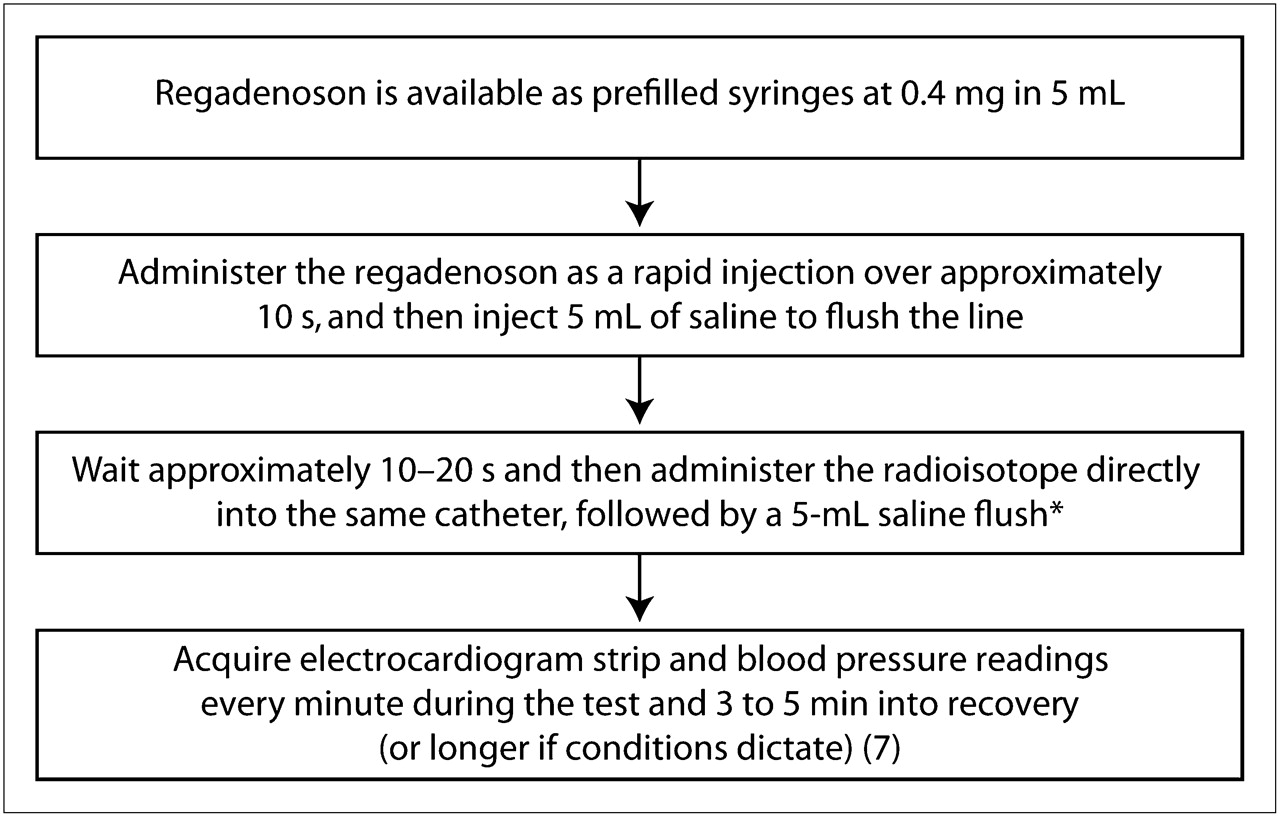
These side effects may also be related to how fast the regadenoson dose is administered. Regadenoson should be administered as a rapid injection over approximately 10 s followed by a 5-mL saline flush. The radiopharmaceutical is injected 10–20 s later, or 25–35 s after the start of the procedure, followed by another saline flush (Fig. 3). We recommend the use of a digital stopwatch to ensure that the injection timing sequence is followed appropriately. When nuclear technologists first use regadenoson, they may tend to rush the regadenoson injection. In our department, after the importance of a steady injection of regadenoson over 8–10 s had been emphasized, and after a sufficient period of practical experience with regadenoson, the staff noticed a reduction in the number of patients with nausea and vomiting. Additionally, the manner in which the regadenoson syringe seal is broken is important. On removal from the package, the syringe must be pulled back and twisted clockwise 3 times to break the seal on the contents before injection. This practice allows the regadenoson to be administered evenly over the recommended 10-s period. Thus, a rapid administration of regadenoson may be partly responsible for the increased incidence of nausea and vomiting. Further studies are needed to determine the underlying factors causing the increase in these mild side effects. Our primary purpose in mentioning these issues here is to prepare the nuclear medicine technologist to be vigilant for an increased incidence of vomiting and persistent headache, compared with adenosine and dipyridamole, and to highlight some potential causes.

Administration of regadenoson. *Aminophylline may be given 1–2 min after injection of isotope to reverse persistent or severe side effects.
In the event of lingering side effects, aminophylline can be administered after the radiopharmaceutical has been injected and had adequate time to distribute (at least 1–2 min after injection of the radiopharmaceutical). For regadenoson-treated patients in the ADVANCE MPI trials, the most common adverse events for which intervention with aminophylline was considered appropriate were angina pectoris, headache, electrocardiogram changes/ST-segment depression, and chest pain. Aminophylline was infused at doses ranging from 72 to 300 mg after an average of 15 min from the start of the regadenoson infusion (43).
The pharmacologic stress procedure is faster and less complicated for regadenoson than for other agents. A flow chart of the regadenoson stress procedure is shown in Figure 3. Because regadenoson has a lower affinity for the A2A receptor than does adenosine (resulting in longer dilation response) and does not require dose adjustment, regadenoson can be administered by a single rapid injection of 0.4 mg in 5 mL (7,34). Administering regadenoson by rapid injection has both practical and cost implications. Not only is a rapid injection easier for staff and patients, but regadenoson dosing does not require the costly materials needed for the constant infusion of adenosine or dipyridamole, such as infusion pumps, microbore tubing, and large-volume syringes. Quantifying the exact savings that can be realized is difficult because of the varying costs among different types of institutions, and a detailed cost analysis is beyond the scope of this paper. The response duration of binodenoson means that it likely can also be administered by this method (27,28). However, the length of the binodenoson effect (>14 min) may require an increase in the monitoring time for each patient.
Additionally, dose adjustment according to patient weight or renal function not only is extra work for the nuclear medicine staff but also increases the possibility of dosing error. A stress agent that does not require dose adjustment can be supplied as prefilled syringes. Any unused agent can then be returned to storage for use in a subsequent procedure, whereas an individually prepared adenosine, dipyridamole, or dobutamine dose would be wasted if a procedure was cancelled or rescheduled. In addition, the use of prefilled syringes facilitates compliance with many of the requirements of U.S. Pharmacopoeia 797. As part of this legislation, doses drawn from vials will have to be used within 1 h, and the syringes that contain these doses will have to be adequately labeled. The increased scrutiny could increase the already high wastage of doses for adenosine and dipyridamole. Thus, the use of prefilled syringes would have a positive effect on the nuclear medicine department by facilitating conformity with U.S. Pharmacopoeia 797 and lowering costs by reducing wastage.
Regadenoson is contraindicated in patients with second- or third-degree atrioventricular block or sinus node dysfunction without a functioning artificial pacemaker and, because of the potential for drug-induced arterial vasodilation, in patients with systolic blood pressure below 90 mm Hg (7). The use of dipyridamole-containing medications within 48 h before the regadenoson procedure, or of aminophylline within 24 h before the procedure, should be avoided (7). Methylxanthines, including caffeine and theophylline, should be avoided for 12 h before regadenoson stress (7). Inadvertent caffeine intake is a major cause of cancellations and rescheduling of procedures, an important waste of time and money for the nuclear medicine department. Mounting evidence suggests that regadenoson may allow greater flexibility with regard to caffeine intake before the MPI procedure. In a pilot study of 41 healthy volunteers, Gaemperli et al. (44) investigated the effects of caffeine on myocardial blood flow during regadenoson stress. Patients were randomized to receive 200 mg of caffeine (equivalent to 2 cups of coffee) or placebo before myocardial blood flow was determined at rest (2 h after caffeine ingestion) and immediately after intravenous administration of regadenoson (0.4 mg). After a 2- to 14-d crossover period, the patients who had received the caffeine underwent imaging again with placebo, and the patients who had received placebo underwent imaging with caffeine. The myocardial blood flow after caffeine was similar to that after placebo both at rest (1.13 ± 0.04 and 1.06 ± 0.05 mL/min/g, respectively) and during regadenoson stress (2.98 ± 0.14 and 3.05 ± 0.14 mL/min/g, respectively). Similarly, the coronary flow reserve after caffeine was not significantly different from that after placebo (2.75 ± 0.16 and 2.97 ± 0.16 mL/min/g, respectively). The data from this study demonstrated with 1-sided 95% confidence that any coronary flow reserve reduction associated with caffeine intake is less than 20% for regadenoson stress. The findings of this study indicate that use of regadenoson may potentially reduce the necessity for caffeine restriction before a stress procedure. This possibility is to be addressed further in future trials.
Other pilot studies indicate that regadenoson may be suitable for use in patients with COPD (45) and asthma (46). Such patients are at increased risk of bronchoconstriction and respiratory problems because of the action of adenosine and dipyridamole on the A2B or A3 receptors, resulting in mast cell degranulation and release of IgE and histamine (23,47–50). Thus, the A2A specificity of regadenoson may potentially prevent these reactions and allow use in patients with reactive airways.
Leaker et al. (46) enrolled patients with mild or moderate asthma who were deemed to be particularly at risk of bronchoconstriction, having demonstrated bronchial hyperreactivity in a standard adenosine monophosphate challenge test. Subjects were randomized 1:1 to receive a single intravenous 0.4-mg bolus of either regadenoson or placebo followed by a 1-to 14-d washout period, before receiving the other treatment. In total, 47 patients completed the study. No significant difference was observed in the mean forced expiratory volume in 1 s (FEV1) at any time after regadenoson or placebo administration. The mean ratio of the FEV1 values at each posttreatment time point to the baseline values was significantly greater after regadenoson administration than after placebo from 10 to 60 min after treatment and was numerically higher (although not significantly so) for other time points. The greatest FEV1 reduction (−36.2%) was observed after a patient was administered regadenoson, although this reduction was asymptomatic and reversed spontaneously. The incidence of bronchoconstrictive reactions, defined as an FEV1 reduction of more than 15% from baseline within 2 h after treatment, was similar after regadenoson (2/47, or 4.3%) and placebo (2/48, or 4.2%); none of these patients had a serious adverse event or a pulmonary adverse event. More patients experienced an adverse event after receiving regadenoson (98%) than after receiving placebo (8%). After receiving regadenoson, 34% of patients experienced dyspnea 0–15 s after dosing. This dyspnea did not correlate with bronchoconstriction in this study, unlike a similar study of adenosine (51), and none of these episodes required treatment.
Thomas et al. (45) enrolled patients with moderate COPD (stage II) and severe COPD (stage III), according to the staging criteria of the scientific committee of the Global Initiative for Chronic Obstructive Lung Disease (52). Patients were randomized 1:1 to receive a single intravenous 0.4-mg dose of regadenoson or placebo, followed by a 7- to 14-d crossover period, before receiving the alternate treatment. There were no statistically significant differences in the least squares mean FEV1 or forced vital capacity at any time point after regadenoson or placebo administration. The maximum reduction in FEV1 was also similar between regadenoson and placebo: 0.11 ± 0.02 and 0.12 ± 0.02 L, respectively (least squares mean ± SE). New-onset wheezing occurred in 6% of patients after receiving regadenoson and 12% of patients after receiving placebo. Bronchoconstrictive reactions (defined as in the asthma study) were observed in 12% (6/49) of patients after receiving regadenoson and 6% (3/49) of patients after receiving placebo; no treatment was administered for any of these events. Adverse events were experienced by 86% of patients after regadenoson and 12% of patients after placebo, with dyspnea the most common adverse event reported after regadenoson administration (61%). All incidences of dyspnea resolved spontaneously within 38 min. Dyspnea was not reported by any patients after receiving placebo.
In these trials, no difference was observed in lung function parameters between patients administered regadenoson and patients administered placebo. Regadenoson is not contraindicated in patients with COPD or asthma, although it is recommended that patients discuss their respiratory history and administration of pre- and poststudy bronchodilator therapy before undergoing regadenoson stress MPI (53). Furthermore, it is recommended that patients with ongoing wheezing not undergo regadenoson stress MPI (7). Further research is required to confirm these observations before regadenoson can confidently be used for MPI procedures in these patient populations; a phase 4 study of the safety and tolerance of regadenoson in patients with COPD and asthma is ongoing. Having an agent that is safe for these patient groups would allow a single protocol to be used for most patients, reducing the number of protocols that have to be in place.
Combining pharmacologic stress with low-level exercise for MPI is thought to decrease side effects, improve image quality, and increase test sensitivity (10,54). The use of regadenoson in conjunction with low-level exercise has been investigated (55). In total, 60 patients underwent an initial MPI procedure with adenosine administered in the supine position, before being randomized to a second procedure with either regadenoson in combination with 4 min of low-level treadmill exercise (2.7 km/h at 0% grade) (n = 39) or placebo in combination with 4 min of low-level treadmill exercise and radiotracer placebo (n = 21). Patients experienced 1 or more adverse events with higher frequency after the adenosine–supine procedure than after the regadenoson–exercise procedure (95% vs. 77%, respectively), with severe adverse events (abdominal pain, chest pain, ST-segment depression, neck pain, headache, and paresthesia) observed in 6.7% of patients during the adenosine–supine procedure and in no patients during the regadenoson–exercise or placebo–exercise procedures. Images obtained using the regadenoson–exercise protocol were judged by all experts to be at least of the same quality as images obtained using the adenosine–supine protocol and were judged to be better by 26% (P = 0.002) (55). It is thought that exercise induces a sympathetic response that compensates for the hypotension and other adverse events that may result from pharmacologic stress agent administration. A limitation of this study is that the regadenoson–exercise protocol was not compared with an adenosine–exercise protocol. Further study will determine whether this is an optimal procedure for regadenoson stress MPI.
CONCLUSION
Initial evidence suggests that A2A-selective agonists such as regadenoson are an improvement on currently available pharmacologic stress agents such as adenosine, dipyridamole, and dobutamine. The fact that regadenoson has clinical efficacy comparable to adenosine, and better safety and tolerability, is probably due to the A2A receptor selectivity of regadenoson. As a low-affinity A2A agonist, regadenoson has an extent and duration of hyperemic response that is close to ideal for MPI and allows administration by rapid injection. The lack of necessity for dose adjustment according to patient weight and renal function allows regadenoson to be supplied in prefilled syringes; this is important to reduce waste and facilitate compliance with legislation. The less complex regadenoson administration will simplify the work of the nuclear medicine staff and offer patients a quicker and easier procedure with potentially milder side effects. In turn, patient satisfaction, department efficiency, and cost-effectiveness should improve.
Further research will reveal if regadenoson can be used in patients with reactive airway disease and how efficacy is affected by caffeine and other drugs normally contraindicated for pharmacologic stress procedures. A reduction of preprocedural requirements would be an improvement, as patient preparation for the procedure would be simplified and the number of cancelled and rescheduled procedures, and the associated costs, would be reduced.
Regadenoson appears to have many of the attributes of an ideal pharmacologic stress agent for MPI. Further research will reveal if other A2A agonists have similar clinical utility.
Acknowledgments
Editorial support was provided by Emily Hutchinson and Elaine Griffin, medical writers at Envision Scientific Solutions funded by Astellas Pharma Global Development, Inc.
REFERENCES
- Received for publication July 10, 2009.
- Accepted for publication May 10, 2010.





{kind=link}
{kind=link}
{kind=link}