


Abstract
Urinary-system elimination of 18F-FDG can be mistaken for pathologic uptake. Furosemide helps eliminate this artifact. Unnecessary administration should be avoided. Our approach obviates furosemide administration and other invasive procedures in many cases. Methods: Thirty-seven cancer patients referred for PET to evaluate treatment response or suspected recurrence were prospectively studied using whole-body scanning, with 18F-FDG injected via dorsal hand catheter beforehand. The catheter was left in place to enable injection of furosemide while the patient was inside the scanner. After abdominopelvic scanning, physicians evaluated the need to inject furosemide. Thirty minutes after furosemide injection, another abdominopelvic scan was obtained to detect postinjection urinary tract changes. Results: Postfurosemide images showed effects due to physiologic elimination in 24 patients (64.9%), of whom 11 patients (45.8%) had more than one inconclusive prefurosemide finding. In 13 patients (35.1%), delayed images confirmed persistent lymph node uptake, including 3 patients (23.1%) with 1 lesion. Conclusion: Furosemide injection during scanning reduces artifacts, shortens examinations, and helps avoid invasive procedures.
The work of nursing professionals in the care of patients with urinary track abnormalities is not limited to dialysis centers or renal departments in hospitals. Many graduates in nursing apply their practical and theoretic knowledge in other areas where these patients require specialized, high-quality care.
Radionuclide renography, cystography, renal scintigraphy, renal ultrasound, and pyelography are common procedures in kidney patients. However, in many cases urinary tract processes have an oncologic etiology. Renal tumors, adrenal masses, bladder cancer, and retroperitoneal nodes can make diagnosis and staging difficult (1). Diagnostic imaging techniques such as PET are useful in this context.
18F-FDG is the most frequently used radiotracer in oncologic PET and allows evaluation of the glucose metabolism of both normal and tumor cells. 18F-FDG PET is useful in precisely diagnosing the primary tumor and determining the extent of the cancer and thus can play a significant role in therapeutic decision making. 18F-FDG is fundamentally eliminated through the urinary system, and physiologic elimination of the radiotracer can be mistaken for focal uptake due to oncologic processes and can interfere with the diagnostic evaluation of the abdominopelvic region, especially in patients with known urogenital disease, gynecologic cancer, or colorectal cancer.
Intravenous administration of the diuretic furosemide (Lasix; Sanofi-Aventis) has proven useful in eliminating these effects. Furosemide administration before radiotracer injection forms part of the 18F-FDG PET protocol in many hospitals. However, furosemide is rarely injected simultaneously with PET image acquisition, while the patient is in the scanner, and without stopping the examination.
This study was performed to evaluate the utility of simultaneous intravenous furosemide injection in eliminating focal uptake due to the physiologic elimination of 18F-FDG during studies performed to confirm or to rule out tumor involvement in the abdominopelvic region.
Through this innovation in the standard furosemide protocol, we aimed to obviate furosemide administration at the beginning of the PET examination protocol, avoid Foley catheterization and collector placement and thus the possibility of bladder perforation, and reduce the acquisition time for delayed PET images.
MATERIALS AND METHODS
A prospective study was performed between April 2003 and January 2004 on 37 patients (24 men and 13 women; mean age, 56.9 y; range, 31−74 y) diagnosed with colon cancer (n = 21), lung cancer (n = 6), cervix cancer (n = 6), bladder cancer (n = 1), breast cancer (n = 1), or abdominal lymphoma (n = 2). The patients were referred to our PET department for evaluation of the response to treatment or of recurrence suspected on the basis of elevated carcinoembryonic antigen levels or inconclusive findings on radiography, bone scanning, CT, or MRI.
Patients with significant antecedents of renal lithiasis, urinary track disease (nephropathy, renal insufficiency with anuria, hypokalemia, hyponatremia, or hypovolemia with or without hypotension), hypersensitivity to sulfonamides, or allergy to furosemide were excluded.
The study was approved by the institution's review board. Before inclusion, patients were informed about the PET examination and the possible adverse effects related to intravenous furosemide injection. Patients agreeing to participate provided their written consent.
Patients underwent whole-body 18F-FDG PET after 4−6 h of fasting with oral hydration (15 L of water). Blood glucose levels were monitored, and the radiotracer was injected when glucose levels were no more than 140 mg/dL.
On arrival, patients were asked about their clinical history, allergies, and preparation for the PET examination (fasting and hydration). They then lay down on a hospital bed in a cubicle. Care was taken to ensure that the temperature was comfortable, and a muscle relaxant was administered if needed.
A 23-gauge butterfly catheter was inserted into a vein in the back of the hand. This site facilitates injection during the PET acquisition, while the patient is inside the scanner. The 18F-FDG dose was injected (4.625 MBq/kg) (2) approximately 50 min before the whole-body PET scan started, and the catheter was left in place.
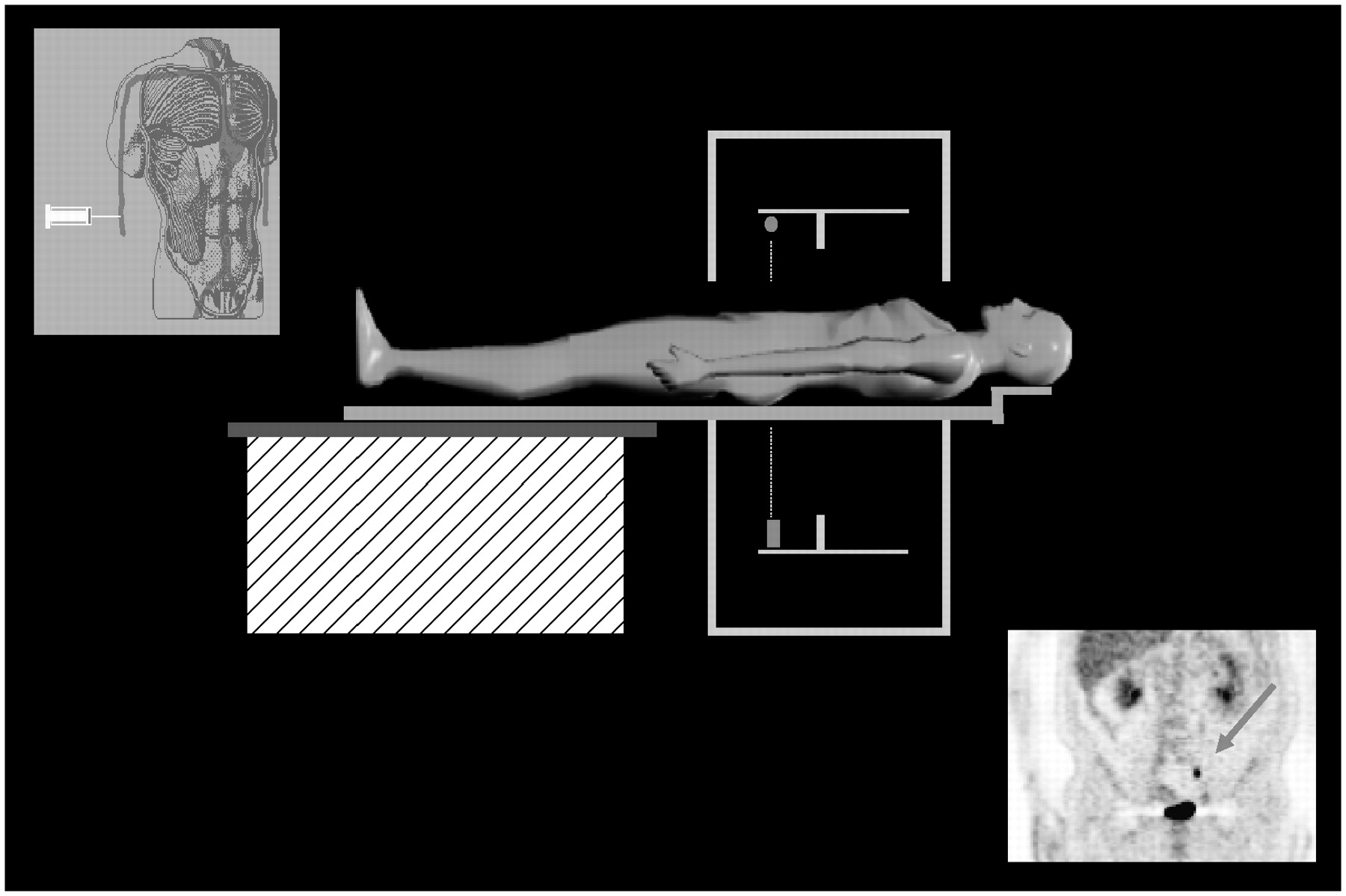
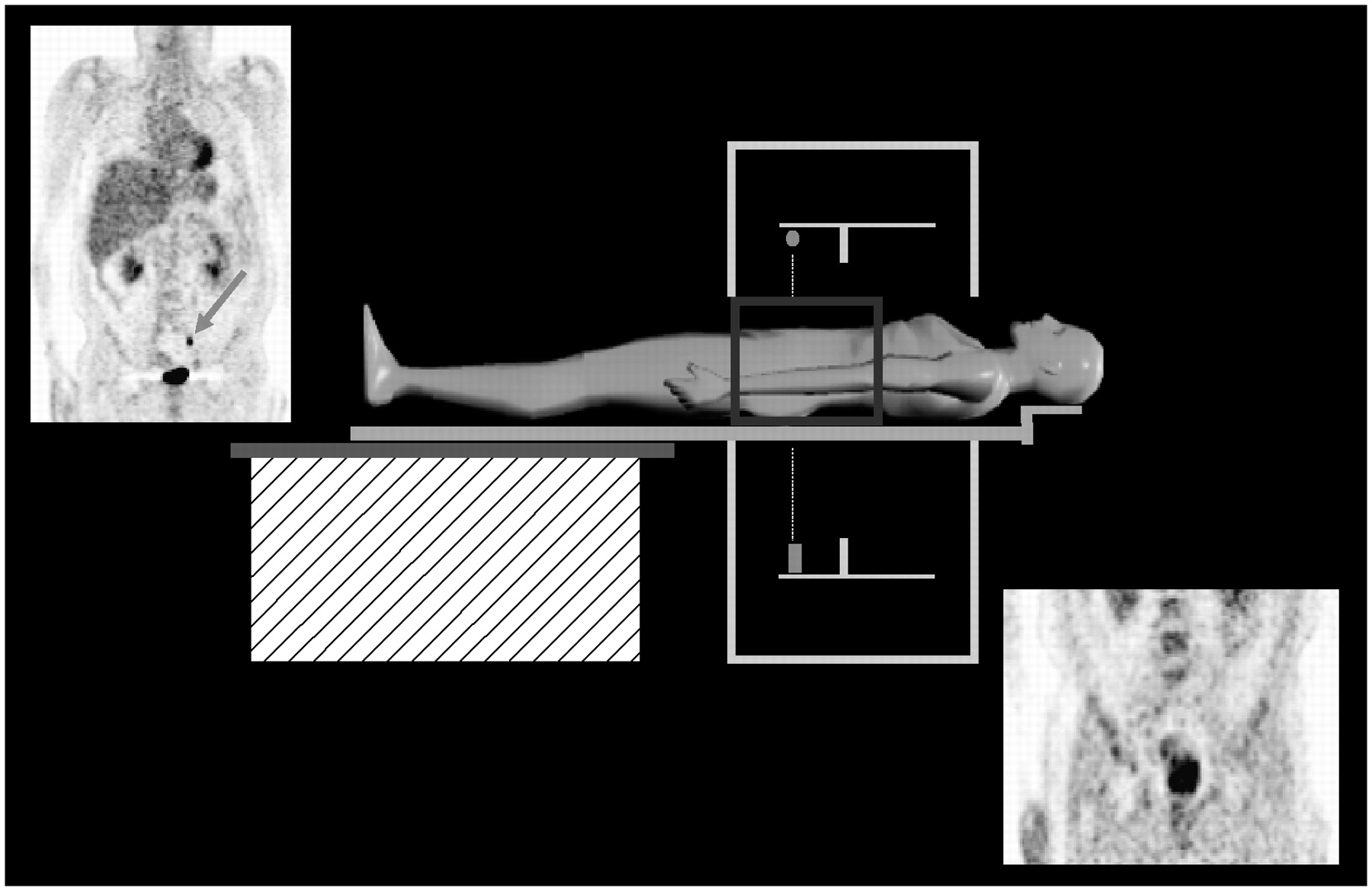
Whole-body scanning was performed from the head to the pelvic floor using an Advance NXi scanner (GE Healthcare) with attenuation correction (germanium transmission rod sources). Immediately before image acquisition, patients were asked to void the bladder to reduce urine accumulation and thereby reduce radiotracer effects due to physiologic 18F-FDG elimination (3). Whole-body PET was performed in the caudocranial direction, acquiring data at 6 bed positions 144.5 mm apart (total, 867 mm). Emission time was 5 min 30 s per bed position; transmission time was 3 min per bed position (2 groups of 3 bed positions, with the emission scan starting after the transmission scan). After scanning the abdominopelvic region, 2 nuclear medicine physicians evaluated the need to inject furosemide (0.5 mg/kg of body weight), based on whether the cause of focal uptake along the urinary tract was clear. The diuretic was always injected during the emission scan to lessen exposure of the nursing staff to radiation (Fig. 1). The average duration of the whole-body scan was approximately 50 min.
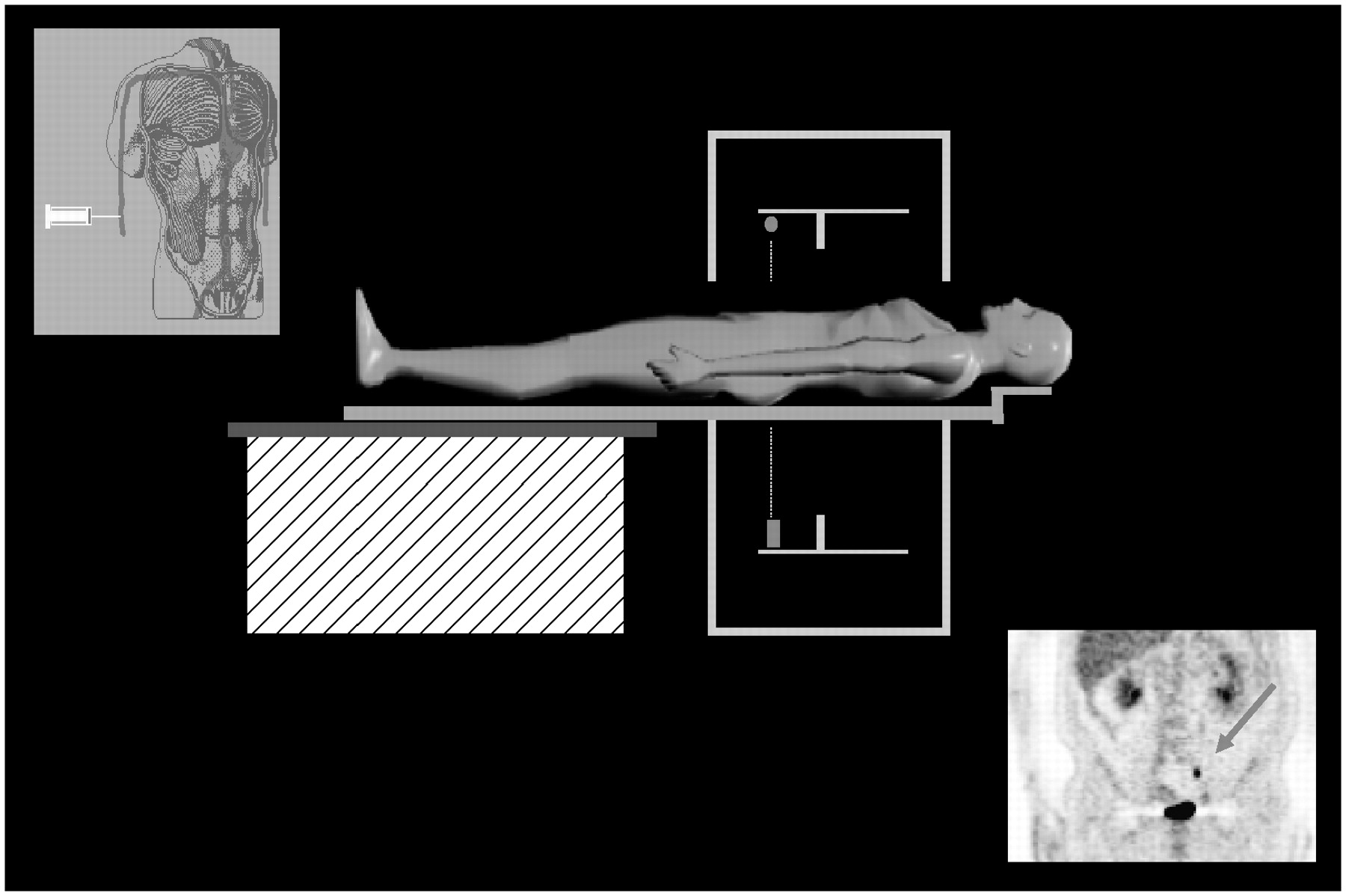
Depiction of furosemide injection (0.5 mg/kg) during third bed position of whole-body 18F-FDG PET acquisition.
Thirty minutes after furosemide injection (coinciding with maximum diuretic effects) (4), a second scan of the abdominopelvic region was obtained to detect postinjection changes along the urinary tract. Data were acquired at 2 bed positions 144.5 mm apart (total, 289 mm). Emission time was 4 min per bed position; transmission time was 2 min per bed position (1 group of 2 bed positions, with the emission scan starting after the transmission scan). This procedure took approximately 12 min (Fig. 2).
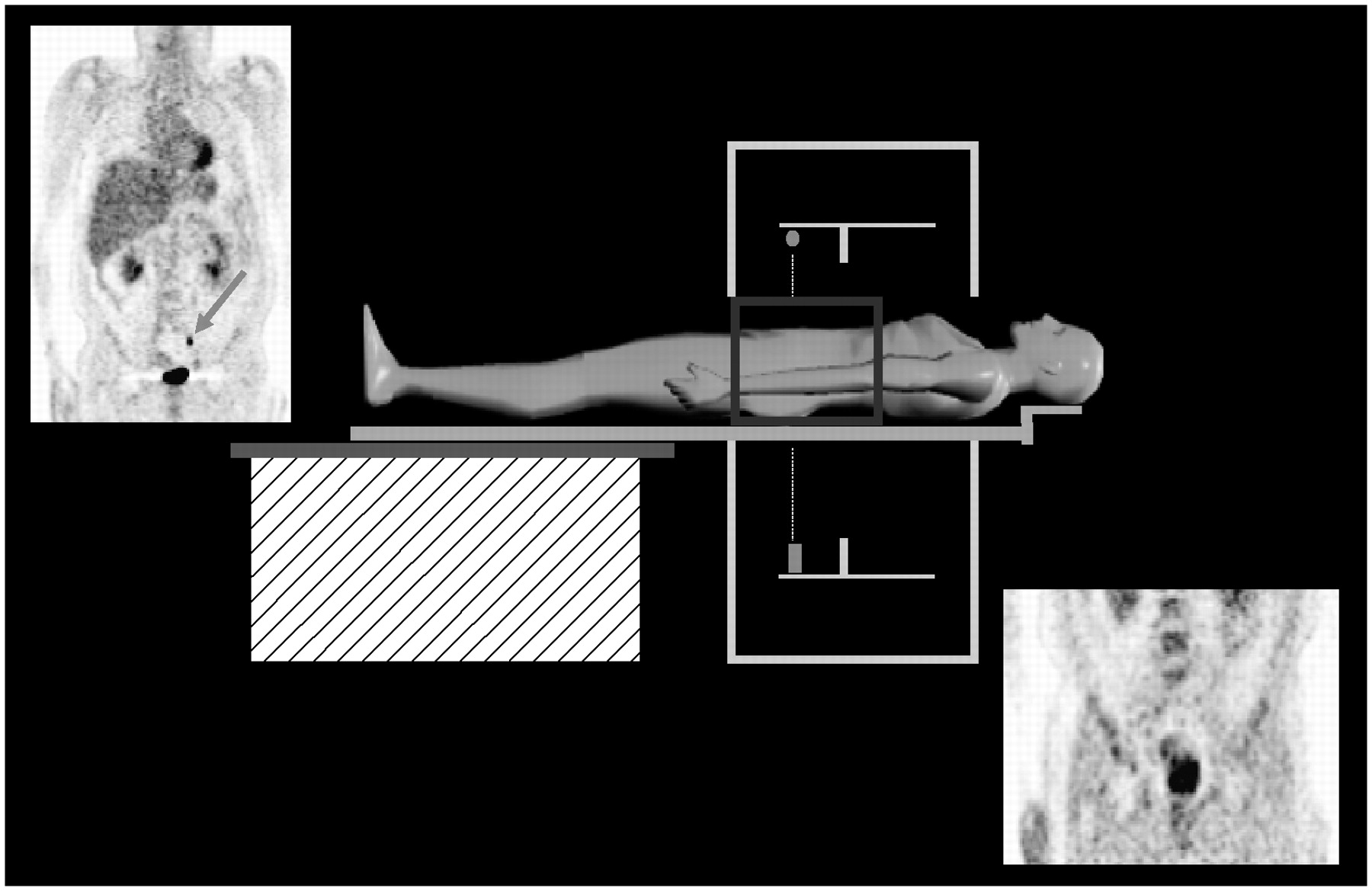
Depiction of postfurosemide acquisition of abdominal and pelvic 18F-FDG PET images at 2 bed positions.
Two nuclear medicine physicians evaluated the whole-body scan visually and scored inconclusive findings as 1 (mild uptake) or 2 (high uptake). Changes in activity on the delayed images were scored as 0 (clearance of prior activity), 1 (mild uptake), or 2 (high uptake).
RESULTS
Images acquired before and after furosemide injection clearly show that the technique was effective at clarifying the etiology of inconclusive focal uptake of 18F-FDG.
Postfurosemide images showed that the prefurosemide findings were due to physiologic elimination in 24 patients (64.9%). Of these patients, 11 (45.8%) had more than one inconclusive prefurosemide finding.
In 13 patients (35.1%), delayed images confirmed lymph nodes with persistent uptake. Of these patients, 3 (23.1%) had a single lesion.
The findings of 21 of 44 images were interpreted as benign, that is, 18F-FDG uptake without a corresponding lesion on CT or MR images. In 16 of these 21, the degree of uptake was mild, with clearance of activity seen on delayed images. The most frequent region of 18F-FDG localization was in the ureter, adjacent to the iliac chain (16/21 images).
The findings of 23 of 44 postfurosemide images showed persistent uptake that was considered pathologic. In 20 of these 23, the degree of uptake was high, showing even greater intensity on delayed images. Lymph node involvement was most common in the iliac chain (8/21) and retroperitoneal region (5/21).
Only 1 patient experienced renal colic. Another patient required previous Foley catheterization of the bladder because of urinary incontinence.
DISCUSSION
PET appeared a decade ago as a noninvasive diagnostic imaging technique for oncologic diseases. The most commonly used radiotracer for oncologic PET studies is 18F-FDG, which enables the evaluation of glucose metabolism and in vivo quantification of this biomolecular process. PET can detect the increased 18F-FDG metabolism in tumor cells that occurs because of cellular proliferation and that is dependent on the stage of malignancy.
Although PET cannot detect micrometastases, it can show lymph node infiltration 0.5 cm in size or larger and in organs without morphologic changes revealed by CT or MRI. PET is used to determine the benignity or malignancy of primary tumors, to assess the response to treatment (chemotherapy, radiotherapy), and to detect tumor recurrence in patients with increased serum tumor markers.
In daily clinical practice, the study of the abdominopelvic region presents special difficulties. Physiologic 18F-FDG elimination is often a confounding factor that could lead to diagnostic error in cases of pathologic focal uptake in kidneys, ureters, and urinary bladder. PET departmental protocols commonly include procedures such as oral hydration and bladder drainage using a Foley catheter before PET acquisition to reduce the 18F-FDG accumulation in the kidneys and bladder (5).
Moreover, in some diseases such as bladder cancer and gynecologic cancer, Foley catheterization is recommended after aggressive surgery that distorts anatomic planes. The procedure involves draining as much urine as possible from the bladder and refilling it with saline solution to increase the contrast of bladder wall uptake and make it easier to identify. Although nurses and technologists have been trained in ways to avoid complications with this technique, it still carries a risk of infection. Some departments prefer the use of a collector device to retain the urine, but this practice is uncomfortable and stressful for the patient. Sometimes, oral hydration is insufficient and an intravenous dose of furosemide is required to increase urine excretion.
Many PET departmental protocols include the use of the diuretics and the Foley catheter before injection of the 18F-FDG (6). However, it is essential to bear in mind that patients with oncologic conditions are physically weak from treatment and that administration of unnecessary medicines must be avoided. In our study, evaluating the abdominal and pelvic region before furosemide administration made it possible to decide whether such administration was needed during the PET acquisition. This enabled shortening of the scan, avoidance of medication overload, and omission of Foley catheterization in some cases.
Intravenous injection of furosemide is necessary when rapid 18F-FDG elimination is required to enable evaluation of doubtful focal uptake along the urinary tract. Furosemide metabolism inhibits the absorption of sodium and chloride ions in the proximal and distal tubules, as well as in the loop of Henle, and thus is highly effective at these locations. The rate of bolus injection of furosemide should never exceed 4 mg/min (i.e., 0.4 mL/min) to avoid hypovolemia. Diuresis begins 5 min after intravenous injection and maximizes at 30 min. This is why we perform delayed scanning 30 min after diuretic administration. Because the effects of furosemide last approximately 2 h, it is important for the patient to drink water when leaving the PET department to avoid dehydration. The PET acquisition time is shorter with our protocol than with standard furosemide protocols.
Because of the rapid diuretic effects of intravenous furosemide, its use during a PET acquisition holds great promise for improving the management of patients with urinary tract conditions.
In cases of diagnostic doubt because of the possible effects of 18F-FDG elimination, administration of intravenous furosemide increased confidence among our nuclear medicine physicians in diagnosing malignant lesions. However, in some cases, quantification of the suspected lesions using the standardized uptake value will be necessary. This could be an interesting direction for further research concerning diuretics and PET (Figs. 3 and 4).
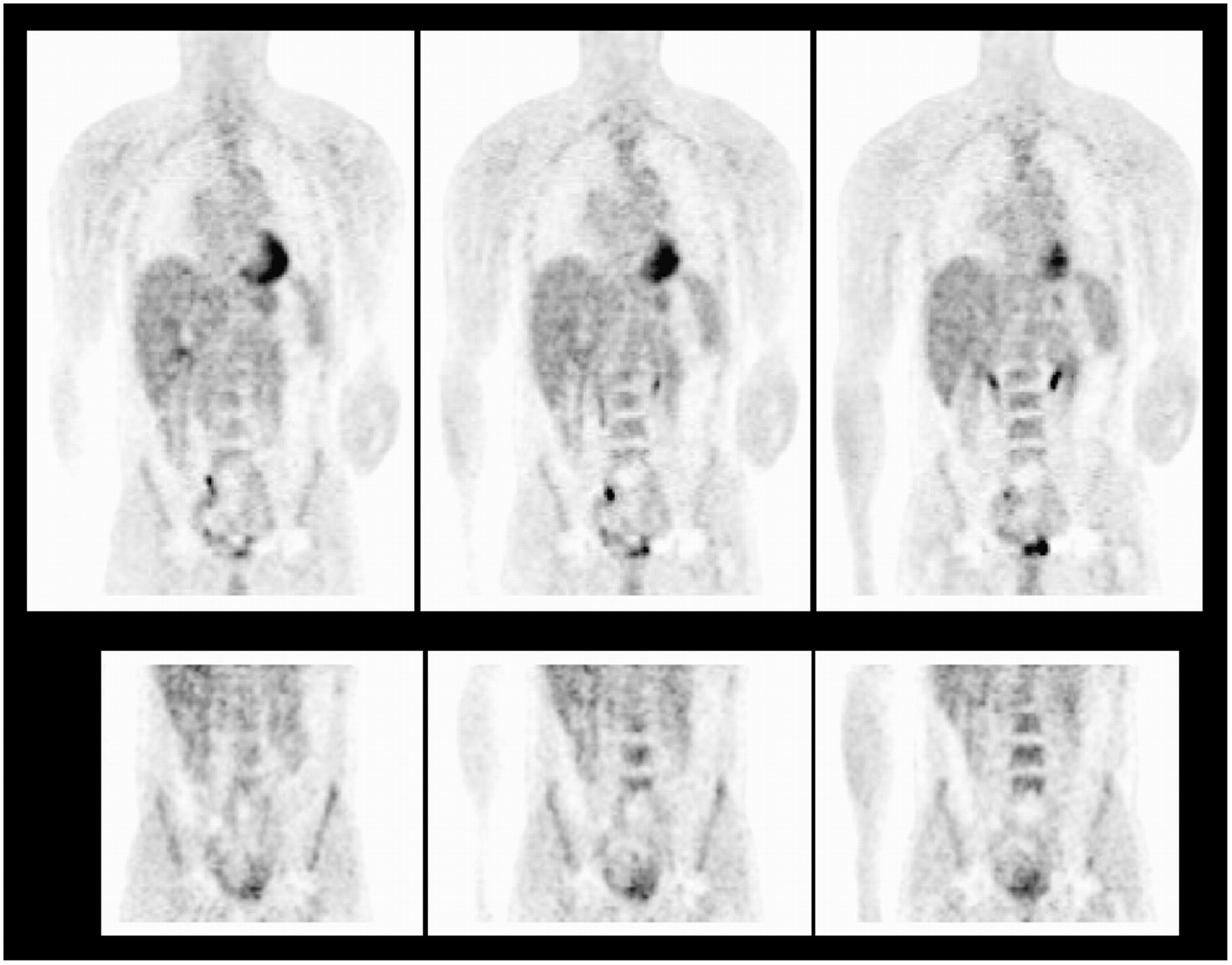
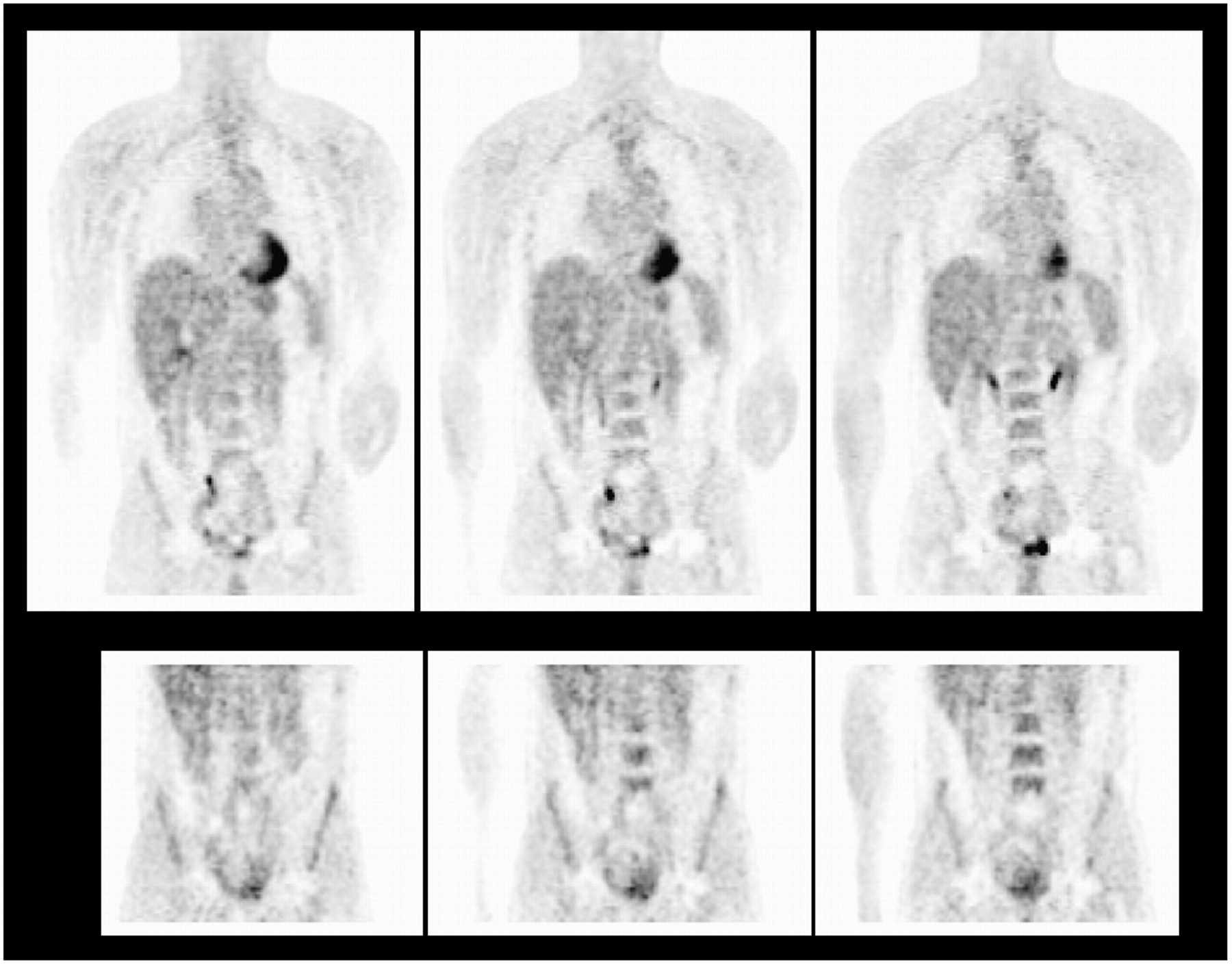
(Top) Whole-body 18F-FDG PET images showing doubtful uptake in right ureter. Node infiltration is suspected. (Bottom) Postfurosemide images showing washout of activity, proving urine retention and ruling out suspected node beside right ureter.

(Top) Whole-body 18F-FDG PET images showing probable urine elimination in right and left ureters. (Bottom) Postfurosemide images showing washout of activity from right ureter due to urine retention and proving lymph nodes adjacent to left iliac chain.
CONCLUSION
From our series of patients undergoing intravenous furosemide injection during PET acquisition, we conclude that the administration of furosemide during the PET examination is efficacious at eliminating artifacts due to the physiologic excretion of 18F-FDG. Furthermore, administering the drug during the scan itself reduces the duration of the examination by avoiding delays. As opposed to injecting all patients before the examination, this approach avoids the administration of furosemide in patients in whom it is not necessary and thus improves the management of oncologic patients. Finally, furosemide administration helps to reduce the need for vesicle catheters or collectors and thus helps to prevent urinary infections and patient discomfort.
Footnotes
-
COPYRIGHT © 2006 by the Society of Nuclear Medicine, Inc.
References
- Received for publication January 19, 2006.
- Accepted for publication May 15, 2006.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Elevated 18F-FDG Levels in Blood and Organs After Angiotensin II Receptor Blocker Administration: Experiment in Mice Administered Telmisartan
- Could Different Hydration Protocols Affect the Quality of 18F-FDG PET/CT Images?
- Preliminary Study of Detecting Urothelial Malignancy with FDG PET in Taiwanese ESRD Patients