


Article Figures & Data
Figures
- FIGURE 1.
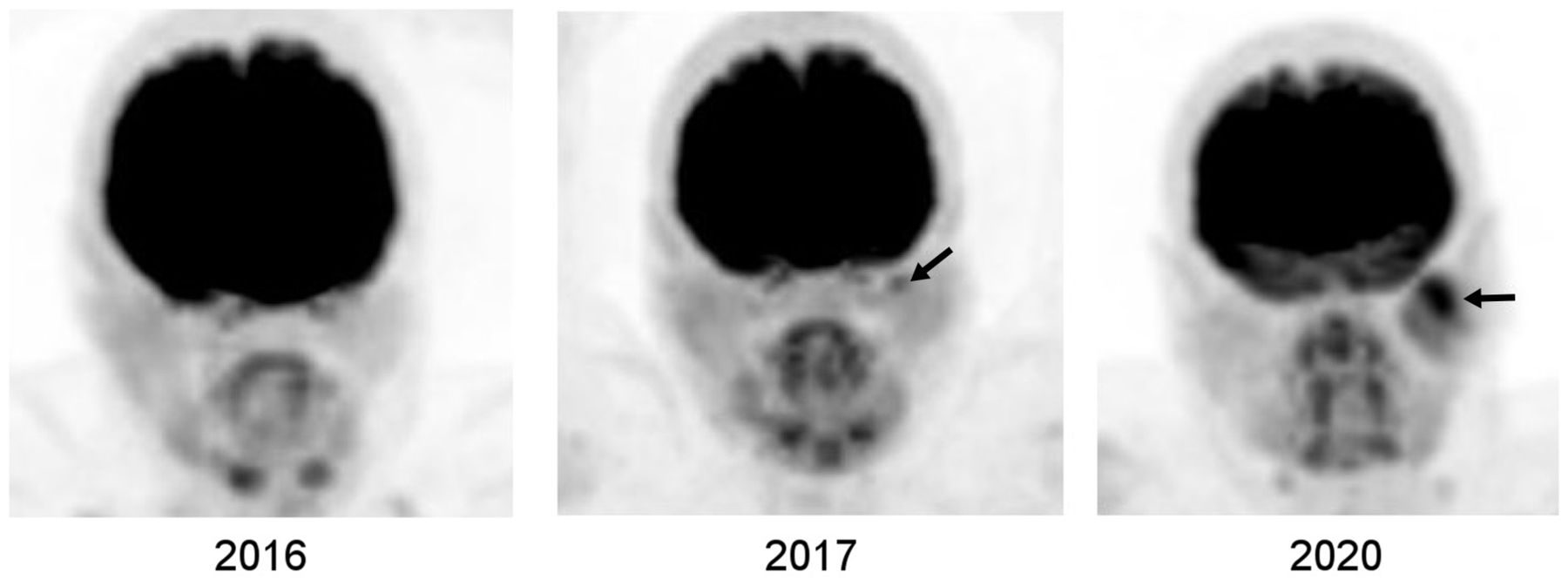
Development of parotid cancer in patient with breast cancer. Selected serial 18F-FDG PET maximum-intensity-projection images of head and neck show that mild focal uptake in left parotid gland in 2017 became larger and more hypermetabolic in 2020 (arrows). Histopathologic examination showed mucoepithelial cancer. There was no abnormal uptake in left parotid gland in 2016, possibly because tumor was either absent at that time or was of microscopic or small volume below PET resolution.
- FIGURE 2.
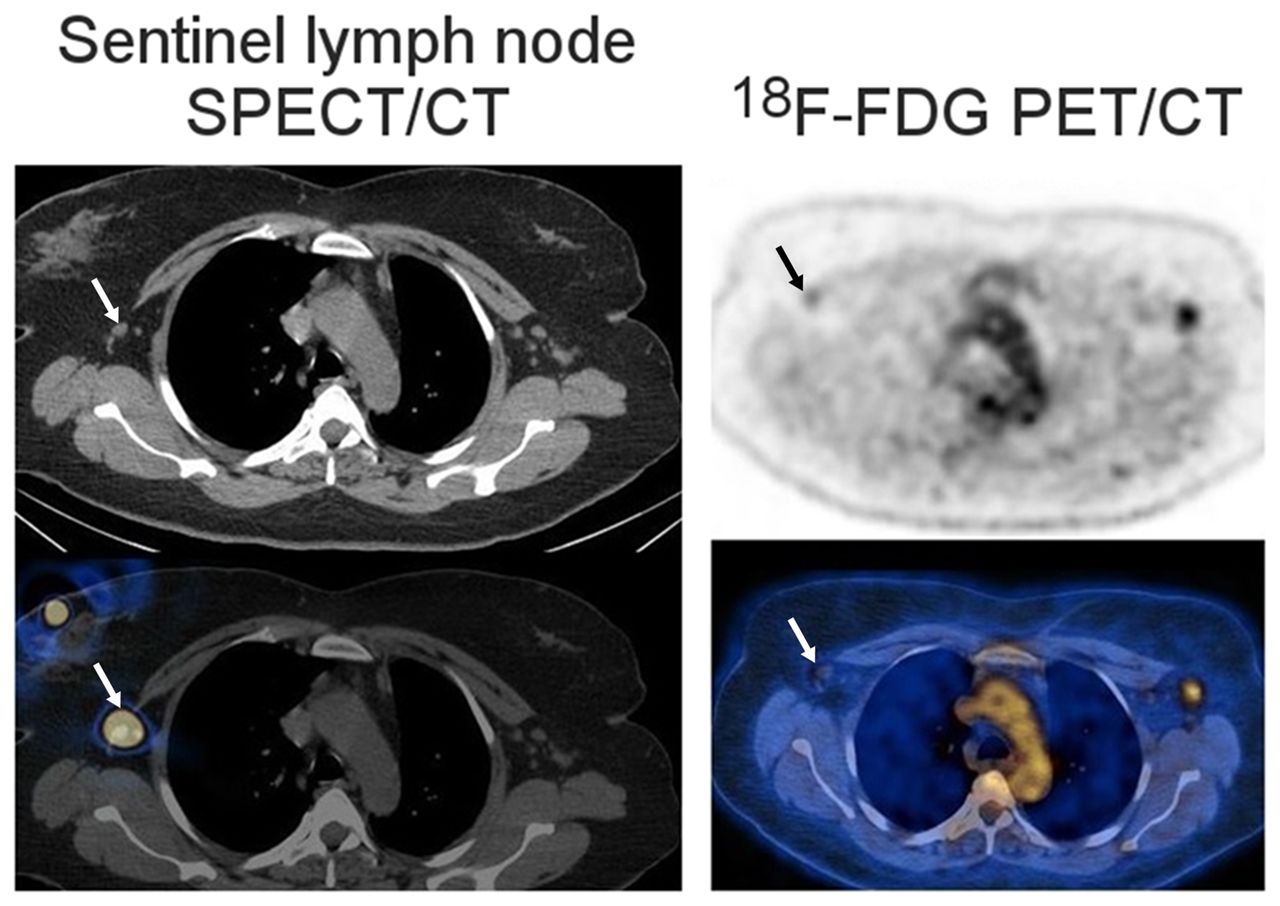
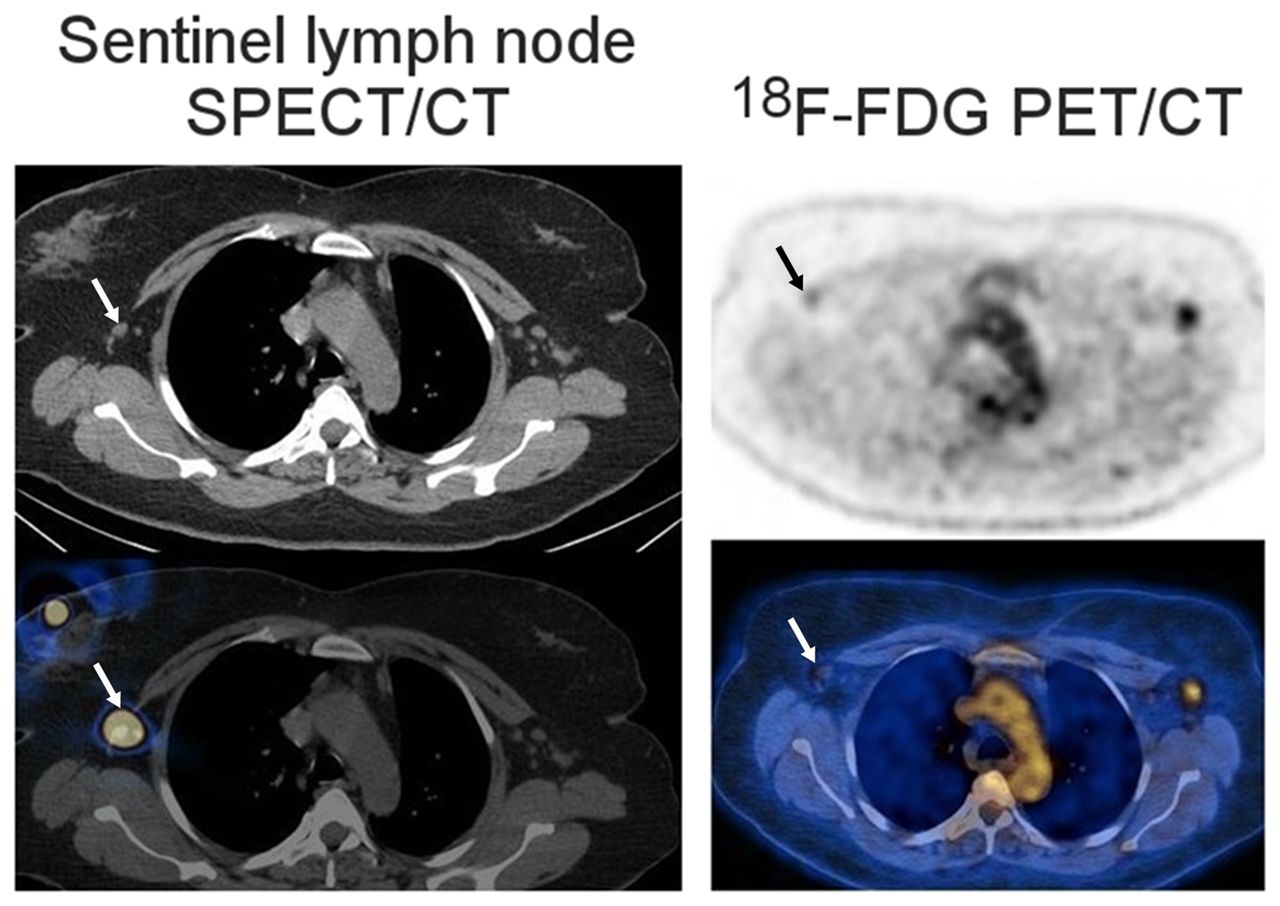
Early metastasis in sentinel lymph node as seen on transaxial SPECT/CT and 18F-FDG PET/CT images of patient with newly diagnosed bilateral invasive lobular breast cancer. SPECT/CT shows right sentinel lymph node (arrows). 18F-FDG PET/CT shows mild uptake in right sentinel lymph node (arrows), found on biopsy to be metastasis. 18F-FDG uptake in left axillary lymph node was also due to metastasis. (Adapted from (38).)
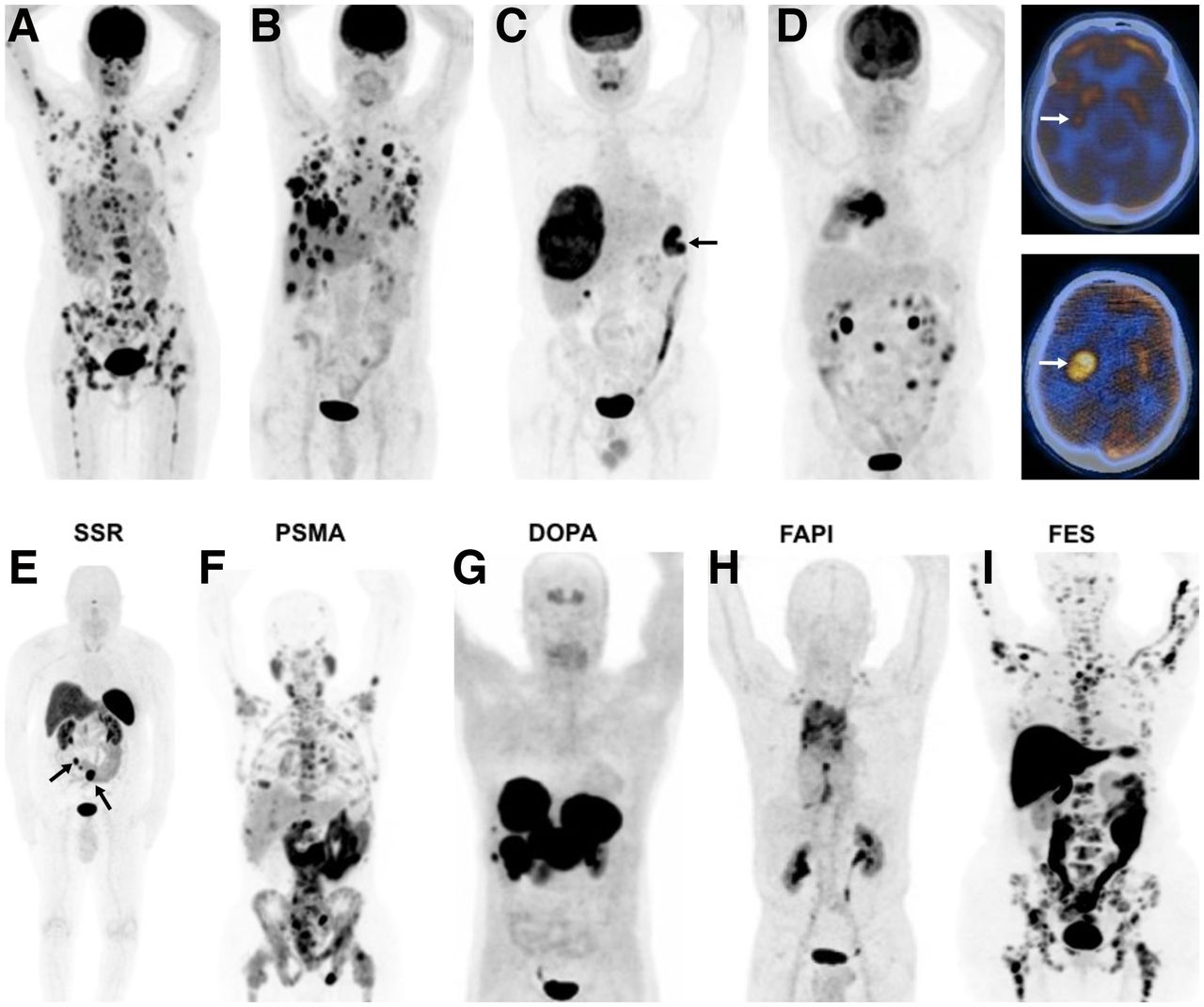
- FIGURE 3.
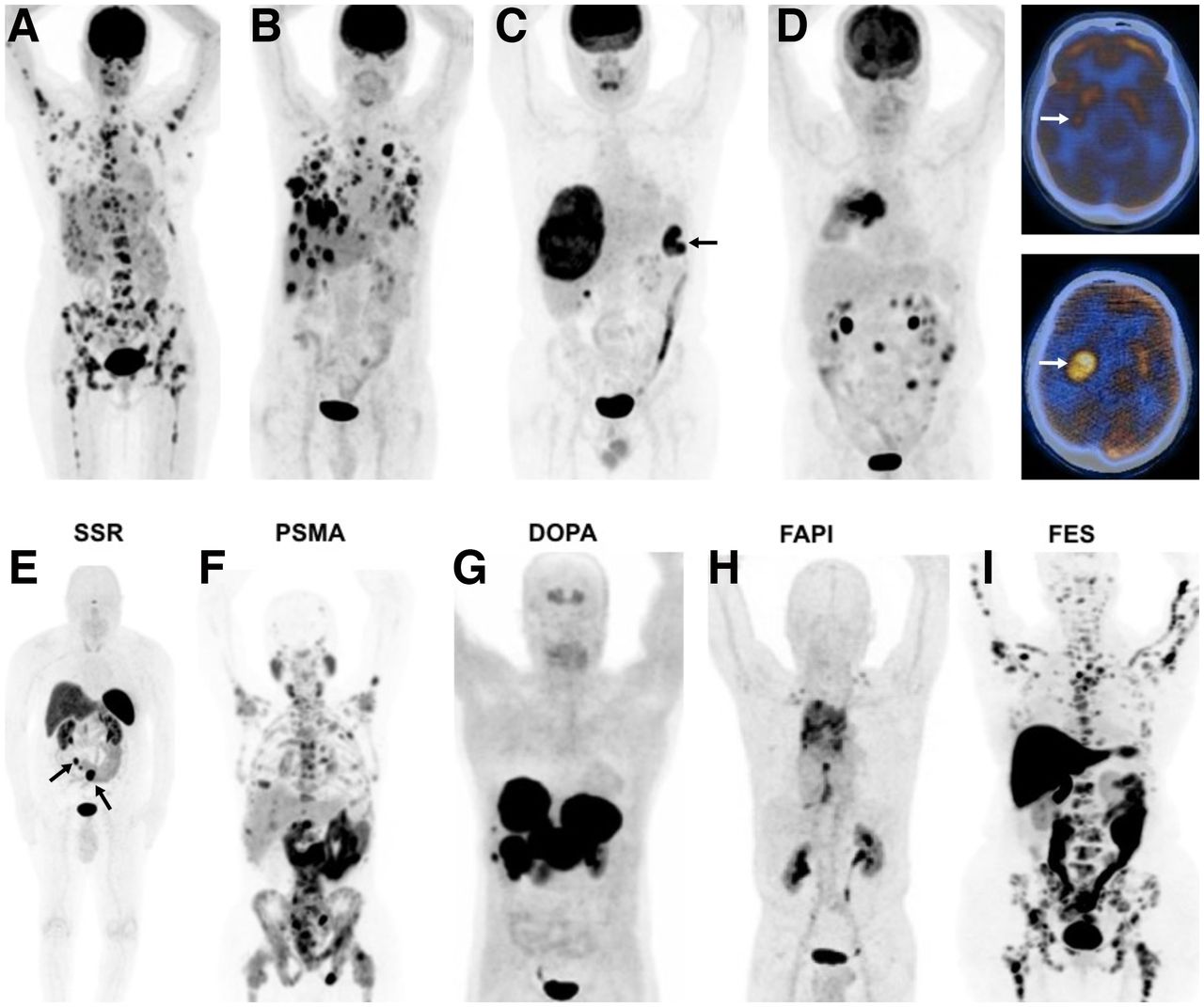
18F-FDG PET images of various cancers and metastases (A–D), and PET images with various other radiotracers (E–I). (A) Right breast cancer (invasive ductal) with multiple metastases in bones, liver, right adrenal, and right axillary lymph nodes. (B) Right breast cancer (poorly differentiated neuroendocrine tumor) with multiple metastases in lungs, liver, and right axillary lymph nodes. (C) Colon cancer in splenic flexure (arrow), with large metastasis in liver. (D) Rapid progression of brain metastasis in patient with cancer in right lung. Whole-body image (left) demonstrated hypermetabolic right lung tumor. On initial PET/CT scan, there was mild focal uptake in tail of right putamen (top right, arrow), but 3 mo later (no treatment), significant increase in size and metabolic activity of metastatic focus in brain was seen (bottom right, arrow). (E) 68Ga-DOTANOC PET image of patient with small-bowel carcinoid, showing primary tumor (left arrow) and multiple mesenteric metastases (right arrow), all with high somatostatin receptor binding. (F) 68Ga-PSMA-11 PET image of patient with prostate cancer, showing diffuse bone and multiple abdominal and pelvic lymph node metastases. (G) 6-18F-fluoro-l-dopa PET image of patient with history of surgically treated well-differentiated ileal neuroendocrine tumor, showing intense uptake in multiple large hepatic metastases. (Adapted from (43).) (H) 68Ga-FAPI PET image of patient with non–small cell lung carcinoma, showing intense uptake in primary tumor and metastatic foci in mediastinum and, bilaterally, in supraclavicular regions. (Adapted from (44).) (I)18F-fluoroestradiol PET image of patient with invasive lobular breast cancer, showing extensive bone and bone marrow involvement with high estrogen receptor binding. (Adapted from (45).)
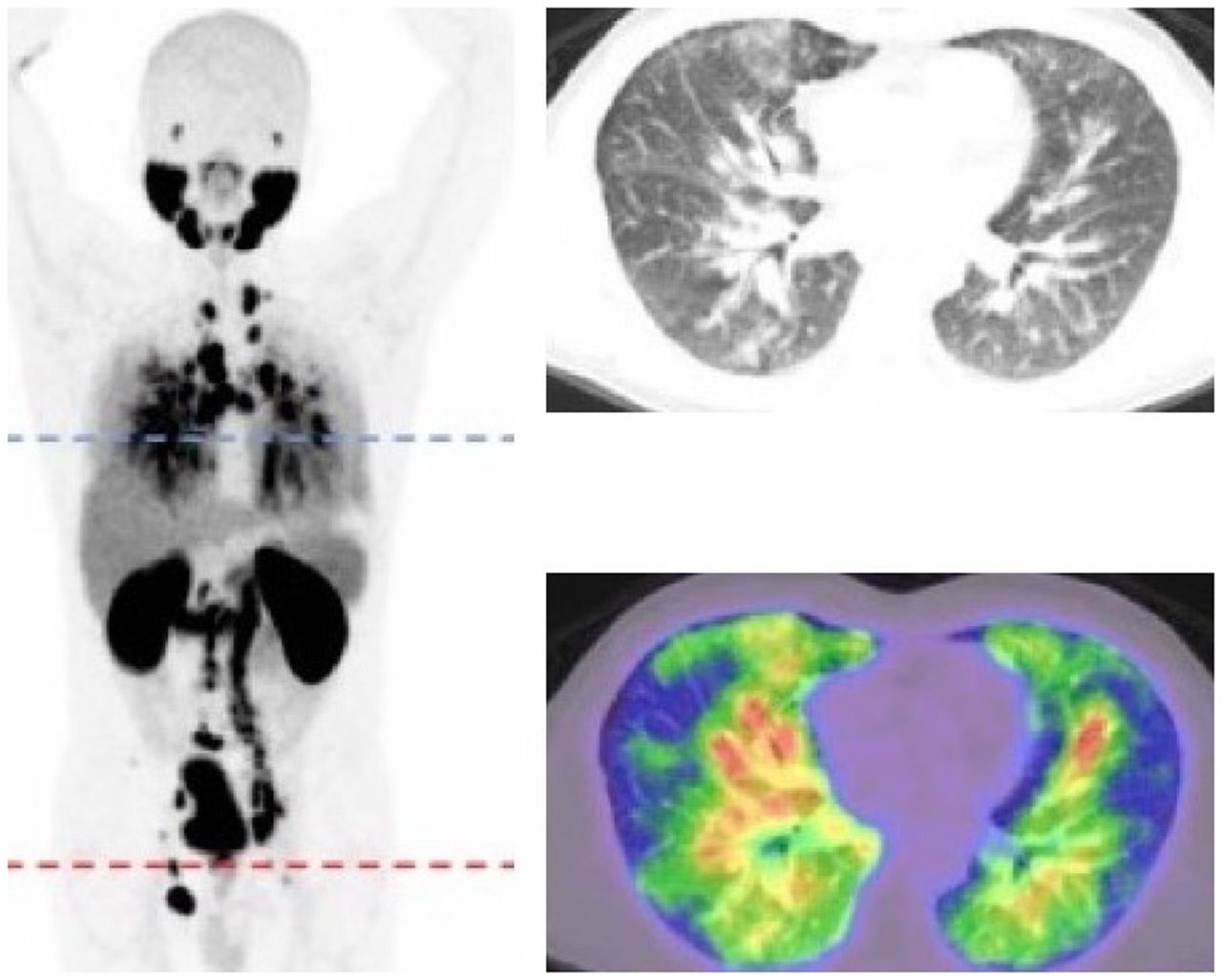
- FIGURE 4.
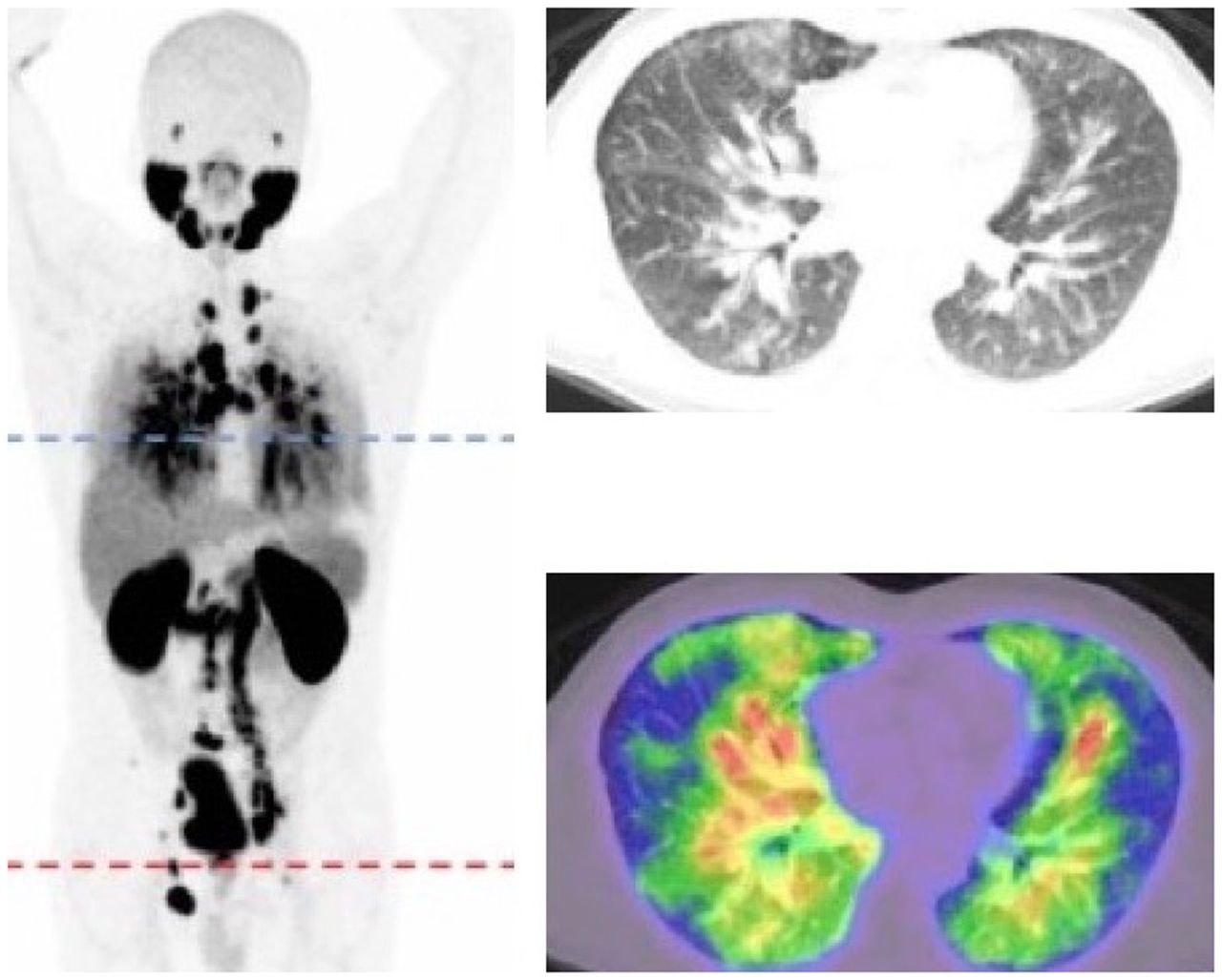
Pulmonary LC in patient with prostate cancer. Whole-body PET and transaxial CT and 68Ga-PSMA ligand images show widespread thickening of interlobular septae and diffusely increased radiotracer uptake. (Adapted with permission of (53).)
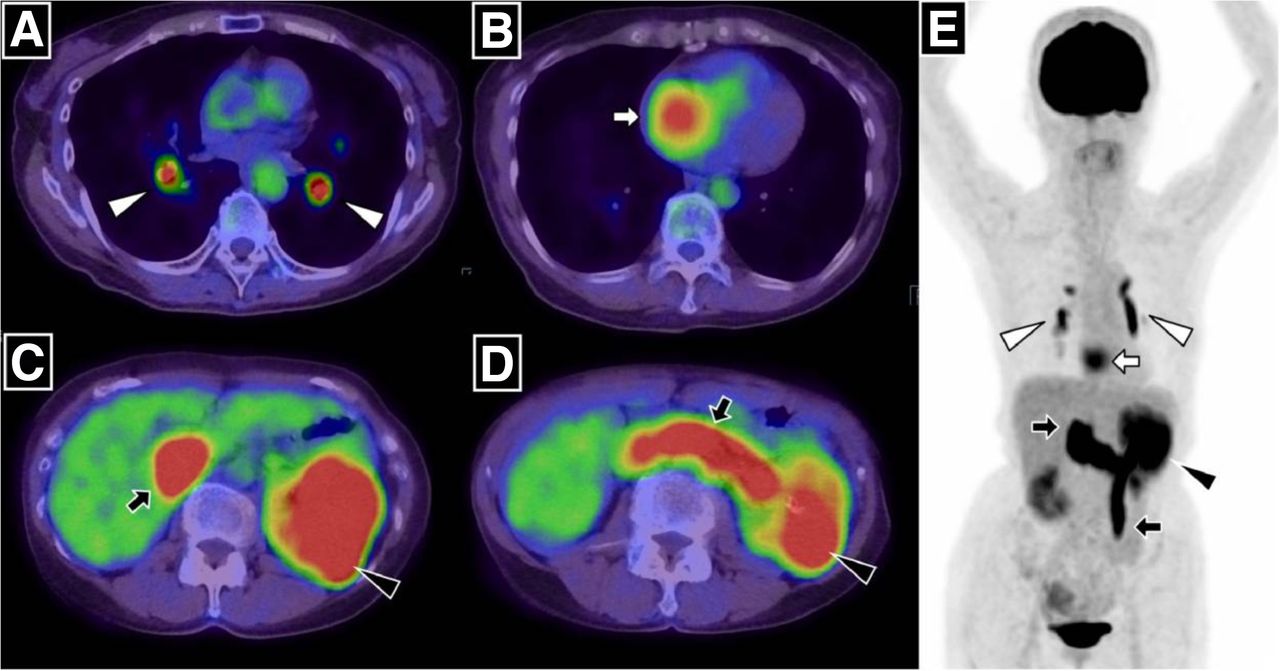
- FIGURE 5.
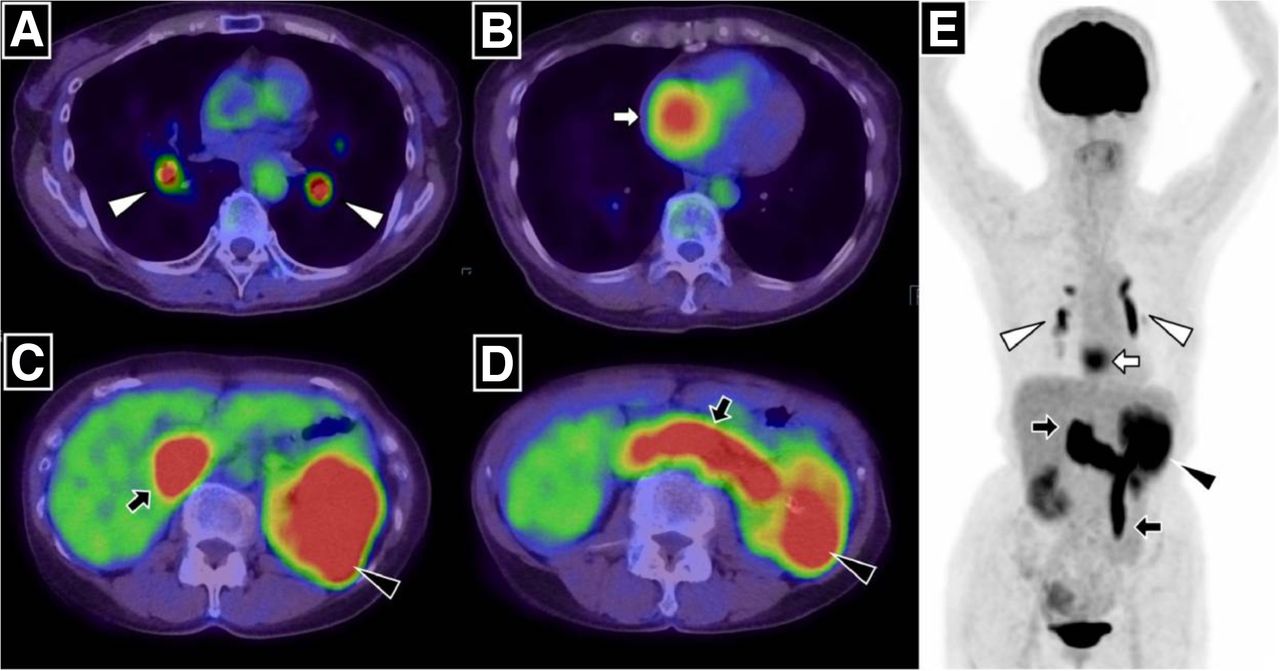
Massive pulmonary tumor emboli from intravascular tumor thrombus in patient with renal cell carcinoma. PET/CT and maximum-intensity-projection images demonstrate 18F-FDG accumulation in left renal tumor, which was continuously observed in left renal vein and extended into infradiaphragmatic inferior vena cava and left ovarian vein (C, D, and E, black arrows). 18F-FDG uptake in left distal pulmonary artery and right and left branches (A and E, white arrowheads) and right atrial cavity (B and E, white arrows) is also seen. (Reprinted with permission of (55).)
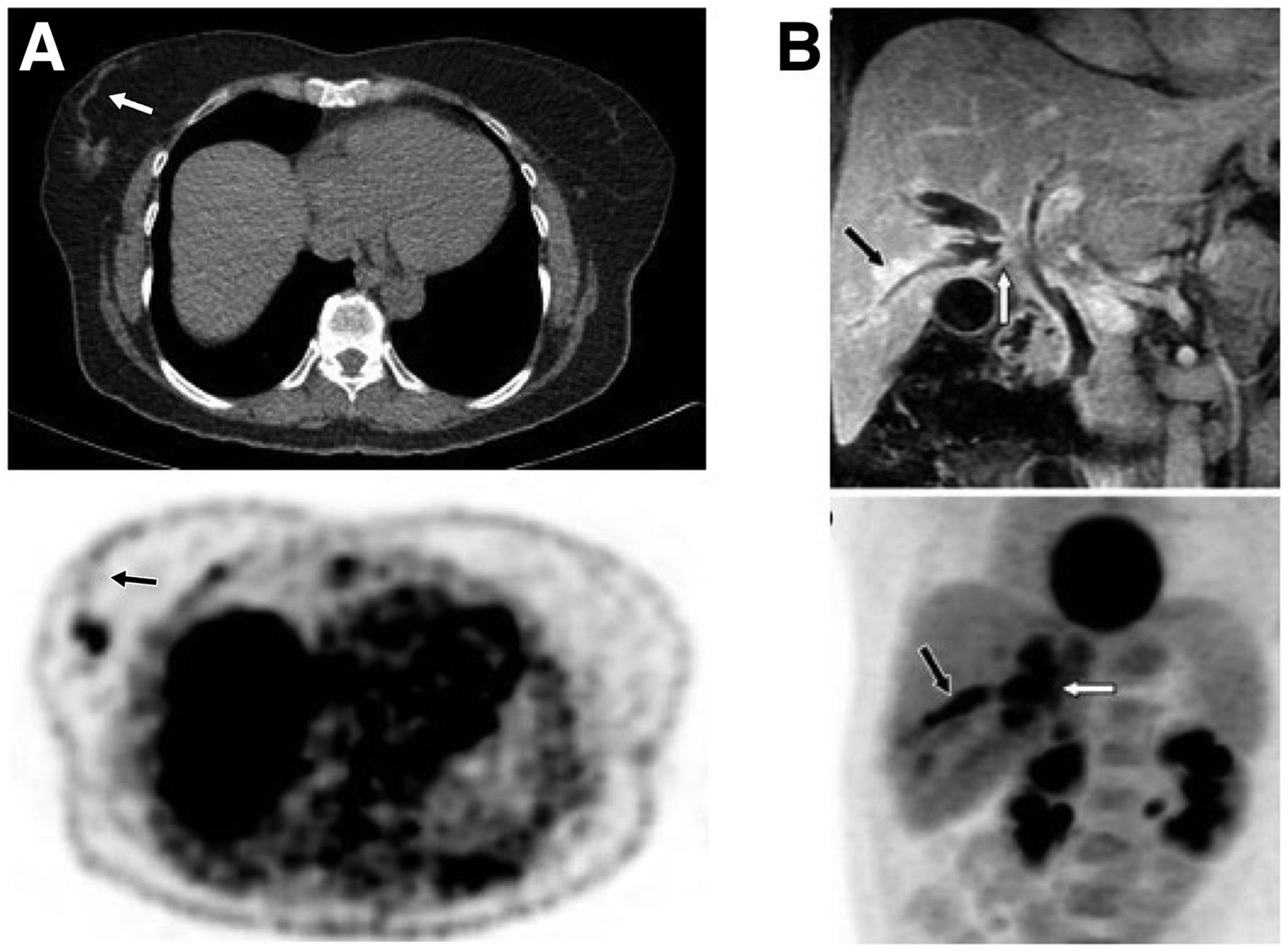
- FIGURE 6.
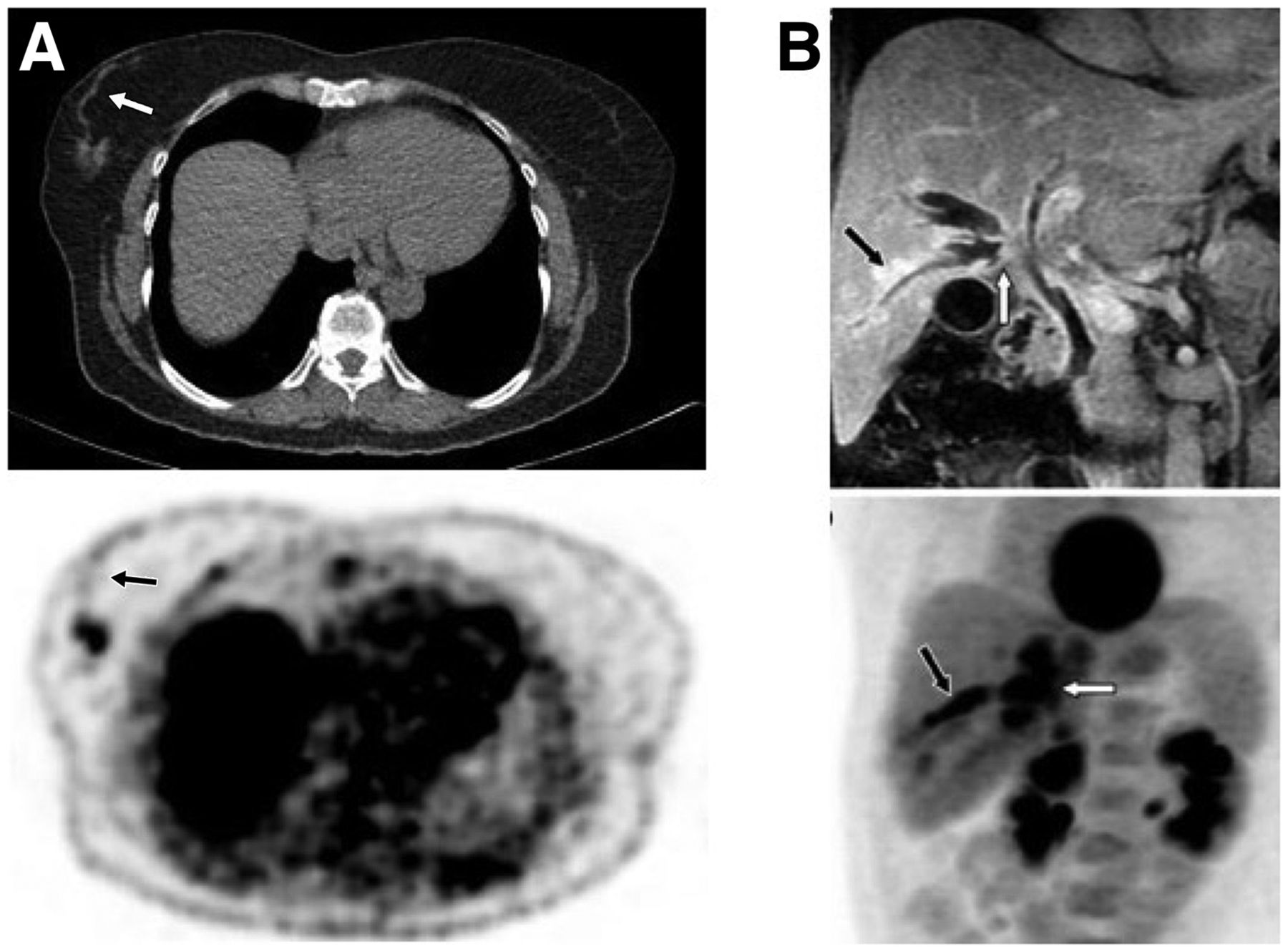
(A) Transaxial CT and 18F-FDG PET images of patient with tubular breast cancer show hypermetabolic primary tumor as well as linear mild activity representing intraluminal tumor uptake either in mammary duct extending to nipple or in lymphatic channel extending to Sappey plexus (arrows). (B) Infiltrating perihilar cholangiocarcinoma with peribiliary extension. Coronal T1-weighted contrast-enhanced MR image (top) shows enhancing tumor of confluence of right ducts (white arrow), intrahepatic ductal dilation, and enhancing right peribiliary extension (black arrow), and 18F-FDG PET maximum-intensity-projection image (bottom) shows 18F-FDG–avid perihilar tumor (white arrow) with peribiliary extension (black arrow). (Adapted from (56).)
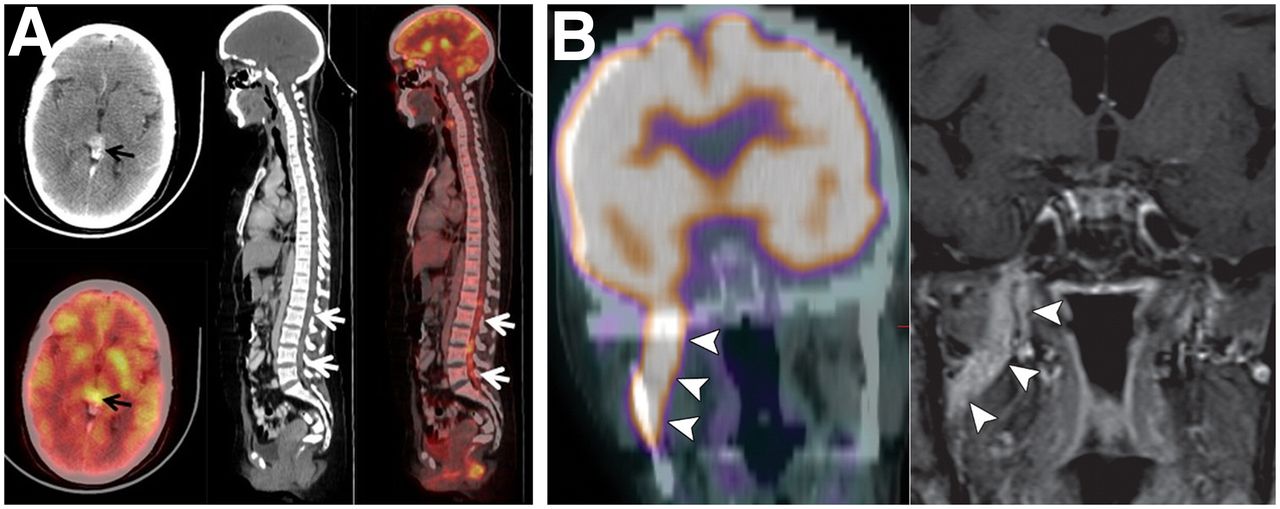
- FIGURE 7.
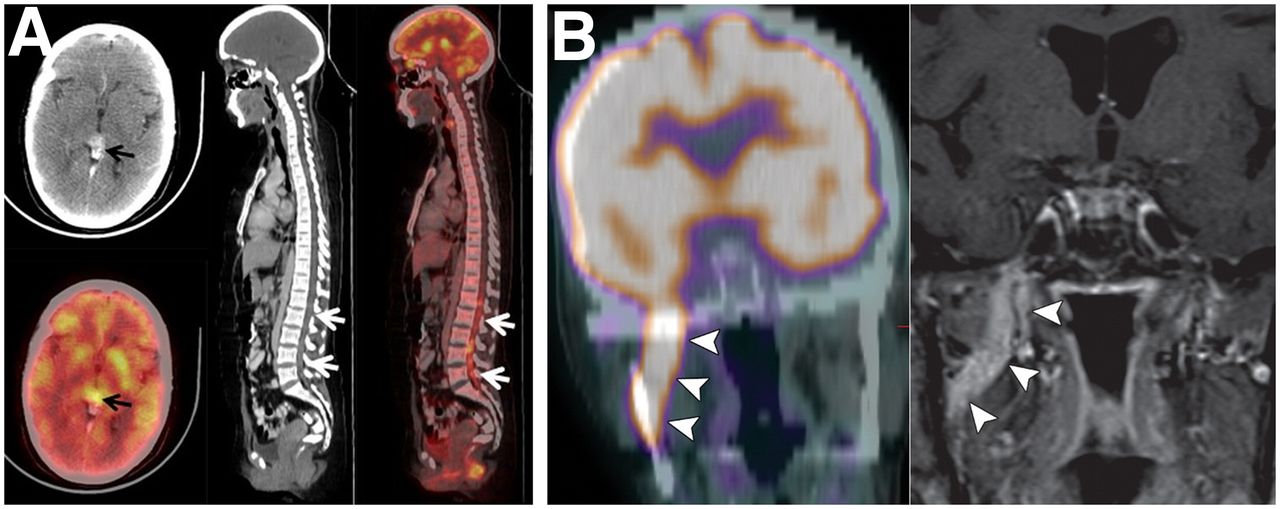
(A) Drop metastases in spinal canal from germ cell tumor of pineal gland. Head CT (top left) and 18F-FDG PET (bottom left) show avidly enhancing hypermetabolic nodular lesion in pineal gland (arrows). Sagittal CT (middle) and 18F-FDG PET/CT (right) show increased uptake in ill-defined densities in spinal canal extending from L1 to L5 (arrows). (Adapted from (58).) (B) Perineural tumor spread along V3 (mandibular) nerve. Coronal 18F-FDG PET/CT (left) and contrast-enhanced T1-weighted fat-saturated MRI (right) show intense 18F-FDG accumulation and abnormal enhancement along V3 (arrowheads). (Adapted with permission of (60).)
Tables
Radiotracer Measures or targets Uptake mechanism Main indications studied Availability 18F-FDG Glucose metabolism (indirect) Is taken up via GLUT1 and phosphorylation by hexokinase Various cancers Widely, routine SSTA Somatostatin receptors Binds mainly to subtype 2 and in lesser degree to subtypes 3 and 5 Well- and moderately differentiated NETs Increasing 68Ga-PSMA Cellular PSMA Binds to cellular PSMA and internalizes Prostate cancer Increasing 18F-NaF Osteoblastic activity Exchanges 18F ions with hydroxyl ions on surface of hydroxyapatite to form fluoroapatite Bone metastases from various cancers Increasing 18F-FLT Cellular proliferation (indirect) Is phosphorylated by thymidine kinase (not incorporated into DNA) Various cancers; NSCLC, lymphomas Limited 18F-FET AA uptake by transporters Enters cells by LAT1 Brain tumors, particularly gliomas Limited 11C-MET AA uptake and protein synthesis Enters cells by LAT1 and is involved in synthesis of proteins and phospholipids Brain tumors, particularly gliomas Limited 18F-FLUC AA uptake by transporters Enter cells by AA transporter ASCT2 and LAT1 Prostate cancer Limited 18F-DOPA 18F-DOPA transport, storage, and metabolism Enters neuroendocrine cells by LAT1, is converted to dopamine by AA decarboxylase, and is trapped in vesicles via VMAT NETs, pheo, neuroblastoma, PG, gliomas Limited 11C-choline and 18F-fluorocholine Cell membrane synthesis or cellular proliferation Is phosphorylated by choline kinase to phosphocholine and converted to phosphatidylcholine Prostate cancer Limited 11C-acetate Cellular proliferation Incorporates into cellular membrane HCC (well-differentiated), renal cancers Limited 68Ga-FAPI Cancer-associated fibroblasts Binds to fibroblast activation protein on cancer-associated fibroblasts Various cancers Limited 18F-FES Estrogen receptor Binds to estrogen receptor Breast cancer, ovarian cancer Limited 89Zr-trastuzumab Human epidermal growth factor Binds to human epidermal growth factor Breast cancer Limited 18F-FDHT Androgen receptor Binds to androgen receptor Prostate cancer Limited 124I Iodine metabolism Is taken up by thyroid follicular cells via Na+/I− symporter, is oxidized by thyroid peroxidase, stays in colloid, or leaves as thyroid hormones Well-differentiated thyroid cancer Limited 124I-MIBG Norepinephrine transporter Is taken up by sympathicomedullary tissue via norepinephrine transporter (uptake-1 system) and stored in neurosecretory granules Pheo, neuroblastoma, PG Limited 18F-FMISO Hypoxia Nitro-group undergoes reduction in hypoxia, forms highly reactive oxygen radicals, and binds to intracellular macromolecules Various cancers, particularly brain and HN Limited 64Cu-ATSM Hypoxia Accumulates in regions with higher CD133+ expression and activates hypoxia inducible factor 1 (possible mechanisms) Various cancers, particularly brain and HN Limited Folate* Folate receptor α Binds to folate receptor-α Various cancers Limited 68Ga-pentixafor CXC motif chemokine receptor 4 Binds to CXC motif chemokine receptor 4 Various cancers Limited 11C-lactate Lactate metabolism Undergoes oxidative phosphorylation Various cancers Limited Immuno-PET* Tumor-associated antigens Monoclonal antibodies bind to tumor-associated antigens Various cancers Limited * Various radiotracers.
GLUT1 = glucose transporter 1; SSTA = 68Ga-SSTAs (somatostatin analogs); NET = neuroendocrine tumor; FLT = fluorothymidine; NSCLC = non–small cell lung carcinoma; FET = fluoroethyltyrosine; AA = amino acid; LAT1 = L-type amino acid transporter; MET = methionine; FLUC = fluciclovine; ASCT2 = alanine, serine, cysteine transporter 2; 18F-DOPA = 6-18F-fluoro-l-dopa; VMAT = volumetric modulated arc therapy; pheo = pheochromocytoma; PG = paraganglioma; HCC = hepatocellular carcinoma; FAPI = fibroblast-activation-protein inhibitor; FES = fluoroestradiol; FDHT = fluorodihydrotestosterone; MIBG = metaiodobenzylguanidine; FMISO = fluoromisonidazole; ATSM = diacetyl-bis(N4-methythiosemicarbazone); HN = head and neck.
Supplemental Data
Files in this Data Supplement:





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}