


Visual Abstract

Abstract
The First Nations peoples in the United States, Canada, Australia, and around the world are substantially disadvantaged by colonialization, including health inequity. For nuclear medicine, the cultural competence of the staff and cultural proficiency of the institution are important minimum expectations. This minimum can be achieved through a scaffold of Indigenous cultural training and immersion programs that allow the nuclear medicine department to be a culturally safe environment for Indigenous patients. Development of such programs requires careful planning and inclusivity of Indigenous people as the key stakeholders but, done appropriately, can positively drive the Indigenous equity pipeline. Central to this undertaking is an understanding of Indigenous ways of learning and the nexus of these ways of learning and learning taxonomies. There remain substantial gaps between the most culturally insightful and the least culturally insightful (individuals and institutions)—gaps that can be addressed, in part, by rich immersive professional development activities in nuclear medicine targeting cultural proficiency and creating culturally safe clinical environments. The opportunity lies before us to provide leadership in nation building and in yindyamarra winhanganha: living respectfully while creating a world worth living in.
The First Nations peoples around the world are substantially disadvantaged by colonialization (1–4). The histories of colonialization are similar in Australia, New Zealand, Canada, and the United States (5); however, there are more than 370 million Indigenous people in 70 countries globally (1). Inequity manifests in almost all aspects of the Western perceived quality of life, including health and education. Specifically, the average life expectancy across the world is 10 y lower for Indigenous people than for non-Indigenous people (2) whereas higher suicide rates and poorer general health are characteristic of Indigenous people (1). Key social determinants of health for Indigenous people relate to overcrowded housing, homelessness, lower levels of education (westernized), poorer numeracy and literacy, and lower incomes. Central to health-care inequity is that the Indigenous people’s paradigm (square peg) does not fit the Westernized paradigm (round hole) of health or education. There are disparities between Indigenous and non-Indigenous Australians in chronic disease, communicable disease, infant health and mortality, mental health, and life expectancy (6). This situation reflects social and socioeconomic factors, including inequitable access to health services, lack of Indigenous people in the health-care workforce, leading to delayed attendance and underuse of services even when available, and sociocultural factors that combine with geographic and economic factors to decrease accessibility to health-care (6). A significant cultural issue is that institutionalized medicine provides a western strategy to closing the gap, thus failing to deliver pathways to services that embrace Indigenous beliefs and knowledge (1).
Health-care inequities are sustained, in part, by implicit and explicit racial bias but are also driven by extrinsic and intrinsic barriers to accessing health-care services among Indigenous peoples (2–4). Cultural competence and Indigenous cultural competence more specifically are critical parts of the curriculum for health-care professions—including professions in nuclear medicine—yet health asymmetry continues to be problematic. This difficulty reflects several complex processes associated with difficulties in changing engrained culture using a bottom-up approach (i.e., student education) and a lack of confidence among non-Indigenous health-care professionals in meeting the cultural needs of Indigenous patients (7–9). It is crucial, therefore, to develop—in parallel to the curriculum—initiatives to implement cultural competence in professional activities, continuing professional development activities, and postgraduate activities. The manner in which education providers and professional bodies develop and apply cultural competence to enhance understanding of social, historical, and cultural determinants and then apply this understanding to adapt and implement culturally appropriate health-care is important in the move toward cultural proficiency and equity.
Understanding of Indigenous needs and barriers can create culturally safe and more productive clinical environments for Indigenous patients, Indigenous colleagues, and the broader culturally diverse patient and staff populations. Although this discussion focuses on the Indigenous people of Australia, the knowledge is readily transferable to other Indigenous peoples across the globe and, more generally, to those confronting ethnicity-based social or health-care inequity. Indeed, the Indigenous people of one land may be displaced geographically to another land (i.e., become a refugee), carrying social asymmetry associated with both their Indigenous status and their refugee status. The chasm of social and health inequity is deepened and widened by implicit, explicit, and historical racial bias. These biases reinforce social injustice weaved through the culture and policies of the institution (i.e., the established westernized culture in which implicit and explicit attitudes and behaviors are engrained in the policy and practice of an organization, government, or community collective) to drive systematic disadvantage to those in most need. Yindyamarra winhanganha is Wiradjuri language indigenous to the lands on which many of the Charles Sturt University (CSU) campuses occupy and translates to “living respectfully in a world worth living in.” The phrase promotes “nation” building through respect, equity and unity. Yindyamarra winhanganha provides a sentinel to direct the path toward and a conduit to realize, Indigenous cultural proficiency.
Institution refers to the established westernized culture where implicit and explicit attitudes and behaviors are ingrained in the policy and practice of an organization, Government or community collective. Nation is a community of people who share language, culture and history. This people-focused and planet-focused (with the planet being defined as the land for which Indigenous people are proud stewards) Indigenous context of nation and nation building contrasts with the industrial and economic focus of colonized nation building.
CULTURAL SAFETY
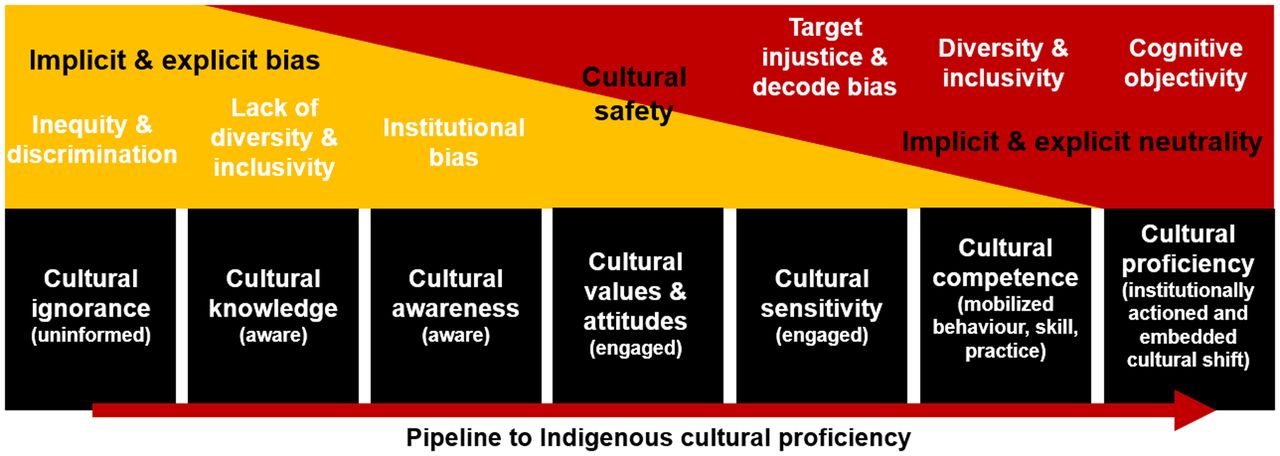
Recent research identified 3 key characteristics valued by Indigenous Australians that are important in the nuclear medicine department and in health-care more generally (10). The first relates to accessibility of services. Nuclear medicine departments are not always open, easy-to-locate, or welcoming spaces. Furthermore, the nature of the services provided in nuclear medicine makes it difficult to colocate with other health services (excepting radiology). Second, consistent with the principle of personalized medicine and even precision medicine, Indigenous people value health-care that is appropriate and responsive to their holistic needs and beliefs. Some cultural norms are not easily accommodated within the nuclear medicine department, driven in part by issues of safety and in part by a lack of insight into cultural beliefs. Third, Indigenous people value culturally safe places where ethnicity and beliefs are respected. To provide a culturally safe environment requires more than cultural knowledge and awareness; it demands engagement through cultural values and attitudes (Fig. 1).
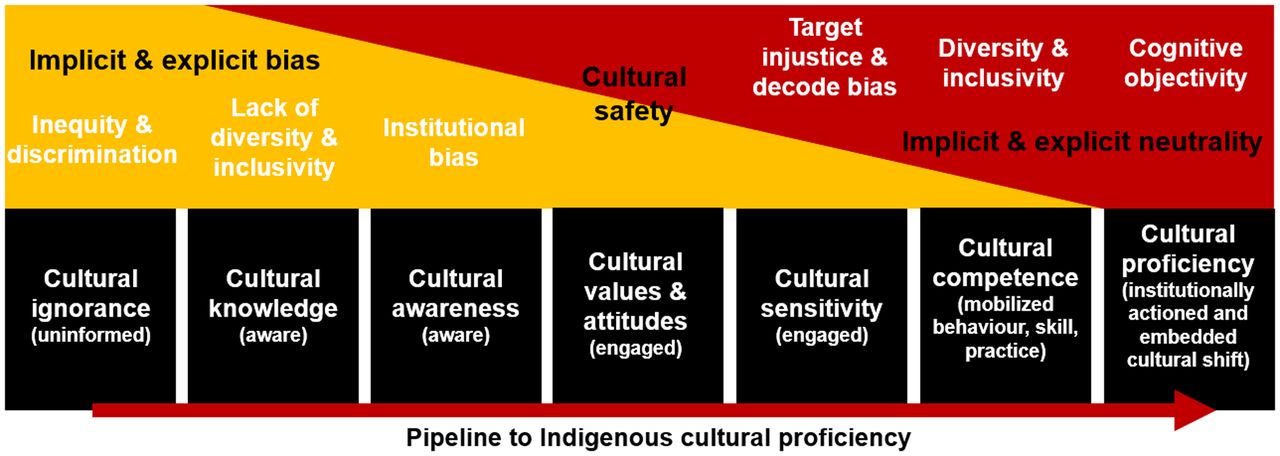
Indigenous cultural proficiency pipeline.
Part of cultural safety in nuclear medicine is related to patient education. The unequal power relationships between health practitioners and Indigenous patients contribute to health inequalities and health asymmetry at the individual and community levels (5). Cultural safety must recognize the historical and contemporary impacts of colonization on Indigenous people’s capacity to trust social, institutional, and political structures (5).
CULTURAL COMPETENCE
Broadly, cultural competence is the capacity to respond to cultural diversity inside health-care systems (11), including understanding and respecting variations in patient health beliefs, values, preferences, behaviors, symptom recognition, thresholds for seeking care, expectations of health-care, compliance, and attitudes about diagnostic procedures (12). Cultural competence is an important strategy for addressing inequities, such as those in health and education, for Indigenous people but requires more than cultural awareness (6). Cultural competence is the attitudes and behaviors, reinforced through policy and practice, that enable effective cross-cultural collegiality and collaboration at the individual and system levels (6).
Endeavors to instill cultural competence in health-care delivery have confronted barriers because of a lack of strategy coherence and because evidence and insight are largely descriptive (6). Success in building a culturally competent health workforce is constrained by a lack of a consistent definition for—and language around—cultural competence, a lack of evidence of the impact of interventions, and a lack of identification of appropriate performance indicators. Cultural competence requires being capable of cultural self-assessment, valuing diversity, managing cultural dynamics, having cultural knowledge, adapting one’s actions through cultural understanding, recognizing cultural differences, and understanding the impact that such differences make.
Recognizing cultural differences and understanding the value that those cultural differences bring to a community or team are an important part of cultural competence (Fig. 1). This quality allows easy demarcation from lower levels of cultural development—levels at which cultural differences might be seen as an opportunity for exploitation and discrimination or are recognized but either ignored or inappropriately responded to.
CULTURAL PROFICIENCY
Cultural proficiency requires, at the individual and institutional levels, the following: knowledge and skills to work effectively in cross-cultural environments; esteem for all forms of cultural difference; cultural reflection and self-assessment around values, beliefs, and bias; cultural humility; commitment to and valuing of diversity and justice; management of cultural dynamics; learning of cultural practices; adaptation of beliefs, systems, policy, and actions through cultural understanding; recognition and facilitation of bidirectional cultural conduits; and knowledge of how to learn about cultural differences.
Beyond the capabilities of cultural competence, cultural proficiency recognizes cultural differences and is equipped to respond effectively and affirmingly both individually and institutionally (Fig. 1). Cultural proficiency is a journey, not an endpoint.
TRAINING IN CULTURAL COMPETENCE AND PROFICIENCY
There have been initiatives and research outlining the value of stand-alone cultural competence workshops for health-care workers. Such workshops are often seen as a tick-the-box mentality that satisfies some tokenistic metric to build awareness. Research in Australia found that most industry-based Indigenous cultural training was at the cultural awareness level—well below the expected level of health-care practitioners (13). Conversely, university-sector Indigenous cultural training tended to provide a foundation of knowledge and awareness that scaffolded to values, attitudes, sensitivity, empathy, and entry-level cultural competence (14). Even when research indicates participants are now more confident working with Indigenous patients, confidence in this aspect of medicine, as in medicine generally, should not be mistaken for competence. Indeed, confidence in the absence of competence can produce deleterious and paradoxic effects. More effective programs include cultural immersions because they develop stronger insights into the connection between culture, history, tradition, beliefs, values, and the interplay with health and health behaviors. Through these rich and deep cultural experiences, a better understanding can be gained of barriers to health and health engagement and of language and communication styles, and potential strategies can be developed to better meet the health-promotion, health-education, and health-safety needs of Indigenous patients.
The journey through cultural awareness to enlightenment and cultural competence or proficiency is tortuous at best and demands commitment, patience, respect, empathy, and perseverance. The task for non-Indigenous health professionals is to challenge the ways of knowing, with the goal of decolonizing their attitudes, beliefs, and actions—a task that is tortuous and challenging yet rich and revelatory (1). There are challenges to confront as a result of historical injury to Indigenous people or cultural incompatibilities. Short-term strategies or changes in policy do not instill trust and confidence among Indigenous people. Strategies driven by well-intended white policy makers confront resistance and overlook the insights of the Indigenous people. Indeed, the idea that policy makers know what is best to improve the health and well-being of Indigenous peoples leaves a sense of tokenism and inevitable failure. Worse is the political point scoring of policy makers that parachute in and disrupt any real progress being made.
HEALTH-CARE INEQUITY
Inequity and bias associated with Indigenous health-care might manifest as a lack of diversity in the teams of health-care professionals. Diversity in the health-care team enables creative problem solving and implementation of solutions better suited to Indigenous patients. Inequity may also manifest from policy developed with homogeneous patient data (lacks Indigenous inclusivity). It is critical that data reflect diversity and be inclusive of Indigenous people; otherwise, there is a significant risk of widening health-care inequities for Indigenous populations.
There are numerous examples of bias that drives the Indigenous health-care inequity gap. Implicit bias or intrinsic bias relates to the attitudes and stereotypes that can unintentionally prejudice or bias. Explicit bias or extrinsic bias is our conscious attitudes and stereotypes that intentionally cause prejudice and bias, of which racial bias is prominent. Both implicit bias and explicit bias cause harm in society and health-care, and both can be deeply engrained in health-care culture and policy. Institutional bias refers to that which is weaved into the culture of the “institution” (a western paradigm) and creates a systematic advantage typically to those already enjoying advantages via social asymmetries. Historical biases are a type of institutional bias in which implicit or explicit bias has shaped historical records. As a result, when those records are used, the biases not only are learned by health-care workers and policy makers but are reinforced. Cognitive bias, a systematic bias common in human health interactions, is that in which observations from the environment around a patient are used in judgment and decision making. These observations can be discriminatory and rely heavily on intuition, which, in turn, is shaped by the personal experiences of the observer. Health-care is neither neutral nor objective; rather, it is embedded in and driven by social, political, and economic agendas. Indeed, health-care policy is frequently designed with parameters for discrimination and amplification of social inequalities. An essential element of the professional development and undergraduate training of nuclear medicine professionals is to develop the capability for critical reflection that reveals intrinsic bias to ensure not only that Indigenous people find nuclear medicine a culturally safe place but also that they encounter health-care professionals who exhibit the attitudes and behaviors of cultural competence. In turn, learning from structured and hidden curricula, and through cultural mentoring, will reengineer the cultural framework of the institution and produce cultural proficiency, thus debugging policy and practice from historical bias.
Indigenous health-care, including in nuclear medicine, confronts issues associated with accessibility to, and opportunity for, access when services are available. Many of the barriers are intrinsic to Indigenous people (e.g., lower uptake of available services), but it remains an expectation that health-care professionals will bridge any divides and work with Indigenous communities to develop culturally safe and appropriate spaces. In turn, this work will increase Indigenous access to and use of expertise and assets. Inclusive in this effort is the obligation to make careers in health, including nuclear medicine, attractive and achievable for Indigenous people. In rural and remote Western Australia, the nuclear medicine needs of Indigenous Australians (oncology, cardiology, and renal services) are provided using a fly-in, fly-out service to provide access to remote communities. Indigenous people in these communities have a 30 times higher myocardial infarction rate than non-Indigenous people and a 50% lower 5-y cancer survival rate. But the success comes from culturally proficient nuclear medicine teams who are committed to closing the inequity divide and who work with the Indigenous community to meet its needs. Accessibility creates equality, but equity also demands opportunity. Well-thought-out strategy by culturally proficient teams is essential to ensure opportunity. Taking the services to the patient in communities that would otherwise not sustain a nuclear medicine service, and using telemedicine, overcome the cultural and socioeconomic barriers to services. A study in Western Australia showed comparative hospital services between metropolitan and regional communities (900 beds with 5,700 staff in the metropolitan hospital and 800 beds with 6,000 staff in the regional hospital) and revealed disparities (15). In metropolitan services, only 0.9% of the staff and 0.8% of the patient population were Indigenous. For regional services, 3.7% of the staff and 8% of the patient population were Indigenous. Although the study indicated that Indigenous people are underrepresented in the workforce of regional services, it also signaled that metropolitan services are lacking in cultural preparedness for local Indigenous patients and for those referred from lower-tier regional sites for specialist services. Also of note, health policy, including funding and rebates, is driven by metropolitan teaching hospitals whose data not only overlook the unique features of regional and rural communities but, expressly and grossly, underrepresent Indigenous people.
THE INDIGENOUS EQUITY PIPELINE
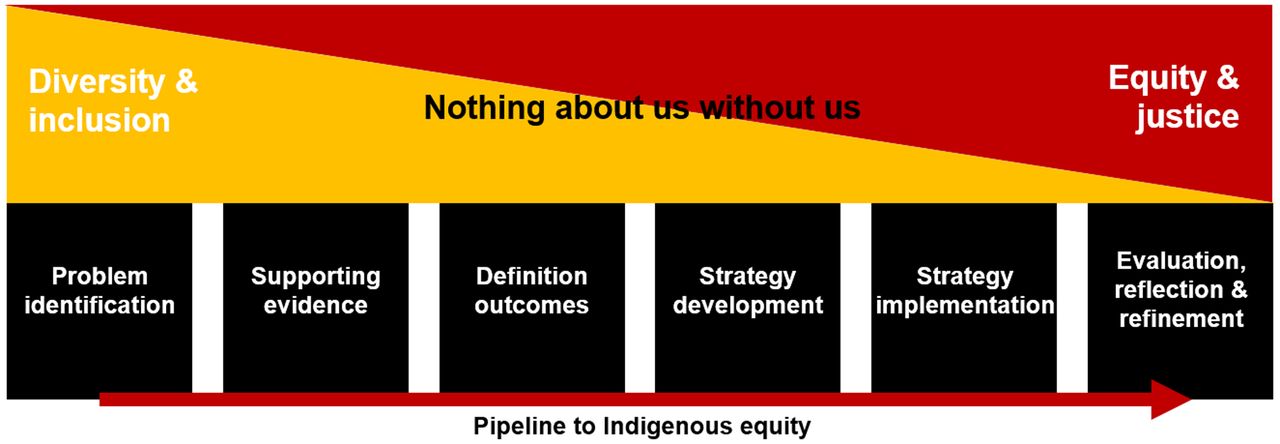
Traditionally, health and education institutions have lacked vertical and horizontal diversity, and it is only in recent decades that a shift has been seen to more inclusivity to overcome barriers to diversity. In health-care generally and nuclear medicine specifically, the philosophy is to “first do no harm” (nonmaleficence) and then improve outcomes (beneficence). To that end, development and implementation of a strategy to close the gap in health-care equity should not create or potentiate inequities but rather should actively mitigate inequities. The equity pipeline can be broken into 6 steps (Fig. 2):

Focus of bias associated with the equity pipeline, beginning with underlying problem of diversity in data and development teams and transforming into outcomes of inequity.
1. Identifying the problem
2. Gathering supporting evidence
3. Defining outcomes
4. Developing a strategy
5. Implementing the strategy
6. Evaluating, reflecting, and refining
Problem identification can be driven by political, commercial, or economic forces. Institutional bias can be engrained in identifying the problem, gathering the evidence, and defining the outcomes. In health-care, the first 3 of these steps are frequently focused on issues associated with the health needs of those already advantaged or privileged. Policy-driving data generally reflect a metropolitan major teaching hospital cohort and seldom include socially or geographically isolated communities. There can also be censoring of data in a way that drives minority underrepresentation and lack of diversity in the data and demands more considered data curation. Outcomes associated with health-care costs discriminate against patients with, for example, higher degrees of morbidity, which in turn create inequity and bias associated with Indigenous groups with higher levels of morbidity. In essence, this discrimination redirects resources away from those in most need, perpetuating the inverse-care law. Strategy and policy development will reflect the diversity, or lack thereof, of the development team and any associated biases. Particular care is needed to ensure that policies do not embed and reinforce the lack of neutrality of the institution and data. There is a potential for bias and inequity when lack of objectivity influences performance metrics. Strategy implementation needs careful consideration and ongoing evaluation to ensure appropriateness for Indigenous populations. In the absence of evaluation of postimplementation performance and appropriate identification of those performance indicators, significant inequity and social injustice may emerge. Among the 6 steps in the pipeline, a spectrum for both diversity and inequity provides clues to cause and solution (Fig. 2). Central to the entire Indigenous equity pipeline is the mantra “nothing about us without us.” Indigenous equity in health-care requires key-stakeholder engagement and inclusivity; too often, the institution rather than the nation is identified as the key stakeholder.
INDIGENOUS LEARNING
In nuclear medicine and health more generally, communication with Indigenous people is a key cultural competence skill but is also a valuable tool in creating a culturally safe environment for all patients. Understanding Indigenous ways of learning will drive improved promotion of health and improved dissemination of patient information, which in turn will drive trust, compliance, and increased health-care engagement. Understanding Indigenous ways of learning or knowing will also provide valuable insight to help the non-Indigenous health practitioner more deeply understand Indigenous barriers to health and health equity. Reflecting meaningfully on Indigenous ways of learning is a conduit to cultural proficiency. The first principle to consider, perhaps more broadly in health promotion than specifically in nuclear medicine, is the barriers to Indigenous learning. If Indigenous patients do not find that hospitals or clinical departments are a culturally safe place for learning, then health professionals need to venture into culturally safe places to better deliver key messages. At a macro level, this venture means engaging with Indigenous people in their communities—an effort that would be helped by including Indigenous members on the health-care team. At a micro level, this venture might be reflected by an individual health-care practitioner who exercises cultural proficiency skills in negating a culturally inappropriate physical space and providing the Indigenous patient with a culturally safe emotional and cognitive environment. In principle, such skills should be no different from the emotional intelligence and cultural competence skills that health-care practitioners use to create safe places for all patients, each with a unique suite of cultural needs. If patients do not learn where we teach, let us teach where they learn.
Likewise, when examining the ways by which Indigenous people learn or acquire knowledge, it is easy to focus on the unique media for the learning, and perhaps the challenges associated with them, rather than appreciating that the core philosophies are largely universal for all learning. Consider the following list of 8 ways of learning for Indigenous people (https://www.8ways.online/); perhaps with the exception of number 8, these are all important tools for learning regardless of ethnicity.
1. Story telling: use of a narrative to make a better connection with the patient and the information being communicated
2. Learning maps: mind maps that draw on the visual nature of learning to create visual pathways and connections among bits of information
3. Nonverbal communication: a vital tool in engagement and in conveying the importance of information
4. Symbols: metaphors or images that are used to reinforce understanding of concepts
5. Nonlinear learning: a way to accommodate lateral thinking and synthesis of new knowledge
6. Deconstruction-and-reconstruction models (learning in whole: watch one, do one, teach one) or scaffold learning (learning in parts)
7. Community links: use of the community to contextualize the value of learning and to provide a repository for sharing of learning within the community
8. Land links: connection of learning to local land, nature, and places, as captured perhaps in part by an emphasis on sustainability in general learning
Valuable insight comes from community engagement and cultural immersion. Australian Indigenous people tell dreamtime stories that survive intact over thousands of years. Like Indigenous people across the globe, Australian Indigenous people tell stories through a cultural bubble of song, dance, ceremony, art, and family that preserves the integrity of the message. If learning is weaved into cultural significance, we create not only a richer understanding and appreciation of the learning but also a map to guide us back to unremembered learning. Cultural acuity, competence, and proficiency are capabilities that health-care practitioners and educators alike should develop so that learning can be crafted into a cultural bubble for enhanced understanding by Indigenous and non-Indigenous patients and students.
TAXONOMIES OF INDIGENOUS CULTURAL PROFICIENCY
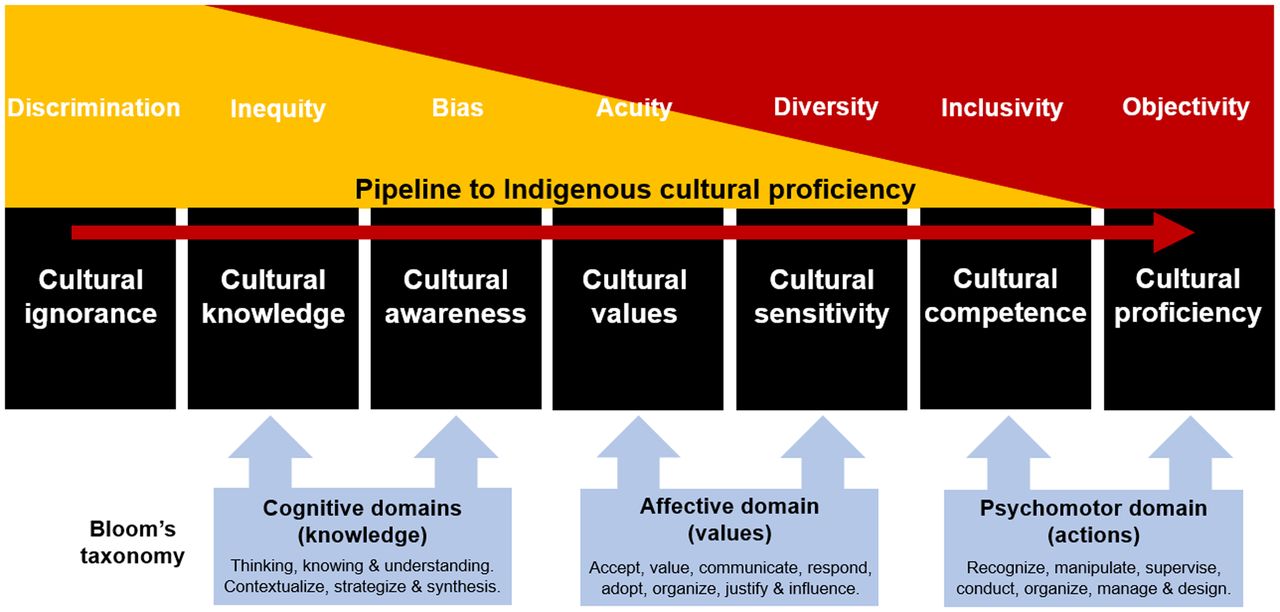
The journey to Indigenous cultural proficiency requires deep insight into Indigenous culture, Indigenous ways of learning, and one’s own ways of learning. The journey is less tortuous through a cultural immersion style of learning and through appreciating the impact of learning taxonomies. Bloom’s cognitive taxonomy can provide a valuable framework for learning that is widely cited in the educational literature. As learning outcomes are developed in university courses, Bloom’s cognitive taxonomies are used to scaffold the learning from lower-order capabilities such as knowing and understanding through to higher-order capabilities such as evaluation and synthesis. Indeed, the knowledge domain that the cognitive taxonomies apply is also scaled from factual information through to metacognitive. This 2-dimensional taxonomy of learning is the very foundation of formal education yet simply affords early capabilities in the Indigenous equity pipeline (Fig. 3). In some regards, it is easy to understand why a focus on cognitive and knowledge domains, even collectively, reinforces bias and inequity. Progression to cultural safety and sensitivity (acuity) along the pipeline requires attention to the less-often-discussed affective domain of Bloom’s taxonomy, in which feelings, attitudes, and values are scaffolded from receiving and responding through to internalized values. The step to cultural competence and proficiency requires command of the capabilities of Bloom’s taxonomies in the psychomotor domain. Here, the emphasis is on behaviors, skills, and what individuals actually do and has a scaffold from perception through to adaption and organization (Fig. 3). The key point here is that overcoming barriers might be viewed as an insurmountable task but that the decolonized mind easily identifies the synergies between ways of learning and the application of westernized education taxonomies. It is not a case of abandoning or reengineering western approaches to learning but rather of adopting a more objective view of similarities to refine and integrate into an approach that is better for all.

Bloom’s taxonomy mapped against Indigenous cultural proficiency pipeline.
THE CSU EXPERIENCE
CSU is a culturally proficient organization built on genuine respect for and engagement with our Indigenous communities. At an institutional level, Indigenous culture is authentically and visibly weaved through strategy, philosophy, and branding. Indigenous culture is respected during the course of any event, meeting, or class. At major university events, Indigenous elders perform a welcome-to-country address, which acknowledges the land and cultural significance of the meeting place. All meetings, whether in person or virtual, include an acknowledgment of country and a paying of respect to Indigenous elders and people—past, present, and future. At its inception, this comprised the meeting chair’s reading an institutionally approved script. Today, meeting chairs deliver their own version of the original acknowledgment that reflects their own values and experiences. This is an authentic insight into the growing of cultural competence and proficiency through personal engagement with Indigenous cultural competence initiatives. The start of each class begins the same: for some, with the formally crafted statement, and for many others, with a personalized acknowledgment that embraces the cultural identity of Indigenous people.
The growth in the Indigenous cultural competence of the CSU staff is driven intrinsically by the strategy and branding of the university and extrinsically by programs designed to enrich Indigenous cultural proficiency. At an entry level, CSU offers an online Indigenous cultural competency program for all staff and students focused on the lower-order taxonomies of enhancing awareness and sensitivity. The significant impact of this program is the development of CSU as a culturally safe place for Indigenous staff and students. The program decolonizes thinking and helps individuals feel more confident about their contribution to closing the inequity gap. Beyond this foundation program, several staff members undergo enrichment through Indigenous cultural immersions. This might be, for example, participation in a traditional smoking ceremony that, for some, provides a cultural epiphany. For others, an overnight or 2- to 3-d immersion in an Indigenous community provides insight not only into how to develop cultural proficiency but also into barriers Indigenous communities confront that drive social asymmetry. In turn, this exercise arms participants with the rich insight they need to become effective policy makers in health, education, and other areas of governance. Students too, in some programs, are afforded the opportunity to undertake enrichment programs as primary health workers or educationalists in Indigenous communities. Such programs impart insights, values, and capabilities that can drive change in communities where Indigenous people are minorities.
CSU staff, students, and members of local, national, and professional communities can undertake postgraduate studies in the Wiradjuri language, culture, and heritage. The program creates awareness and motivation to reverse the colonization, dislocation, and dispossession of Indigenous people with immersion in and celebration of the Wiradjuri nation. All coursework programs at CSU—undergraduate and postgraduate—are mandated to include at least 1 subject (12.5% of an annual full-time study-load equivalent) approved as an Indigenous subject by the Indigenous Board of Studies. This requirement drives awareness in some students who are at a foundational level (cognitive domain) whereas other students, who have already mastered the cognitive foundation, may be driven to engage more deeply. One key performance indicator that speaks to the success of these programs is that CSU is the Australian university with the highest proportion of Indigenous students and, more importantly, with the highest retention and completion rates. One observation is that the increase in the proportion of students who are Indigenous reflects both an absolute increase in Indigenous enrollment and an increase in students identifying as Indigenous who might otherwise not share that identity. In either case, it speaks to the strategies that create culturally safe environments and reflect institutional cultural proficiency.
CSU has also invested in physical resources that support cultural safety and mirror Indigenous ways of learning—resources that are excellent for all students and staff. At the Wagga Wagga campus, open native spaces, including a large amphitheater, are often used for outdoor classes. Wagga Wagga campus also hosts an Indigenous food garden that not only provides an education resource but also supports biodiversity in a rich habitat. Each campus has a First Nations student center to bring Indigenous students together and provide culturally safe places. The Bathurst campus has a vibrant space dedicated as a meeting place for Wiradjuri elders. On the Port Macquarie campus, outdoor spaces include a lecture space (Fig. 4 background) and a fire pit that allows meeting and teaching in a yarning circle around the fire (Fig. 4). The significance of the yarning circle is equity (all facing the center), engagement, and open communication.

Outdoor learning space in Port Macquarie campus of CSU, with tiered lecture theater seating in background and covered yarning circle around fire pit for open discussion and meeting in foreground.
CONCLUSION
The divide associated with Indigenous inequities, despite the efforts of individuals, corporations, and policy makers, continues to be problematic. This divide reflects 2 maxims: that the health-care system is only as strong as its weakest link and that, unfortunately, there is a substantial gap between the most culturally insightful and the least culturally insightful. In turn, this gap perpetuates the inverse-care law, by which those in most need of health-care have disproportionately decreased access to it. Indigenous health-care without diversity and inclusivity in the workforce, and without rich immersive professional development activities targeting cultural proficiency using cognitive, affective, and psychomotor taxonomies, is counterintuitive to the first-do-no-harm mantra of western medicine and nonmaleficence. More importantly, such immersive strategies toward Indigenous cultural training and toward diversity and inclusivity help create culturally safe clinical environments for patients, helping reduce social and cultural barriers to Indigenous people accessing medical services. The commitment of non-Indigenous health-care professionals to developing cultural competence and proficiency is the essence of nation building and of living respectfully in a world worth living in: yindyamarra winhanganha.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online July 30, 2021.
REFERENCES
- Received for publication April 13, 2021.
- Revision received June 12, 2021.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}