


Article Figures & Data
Figures
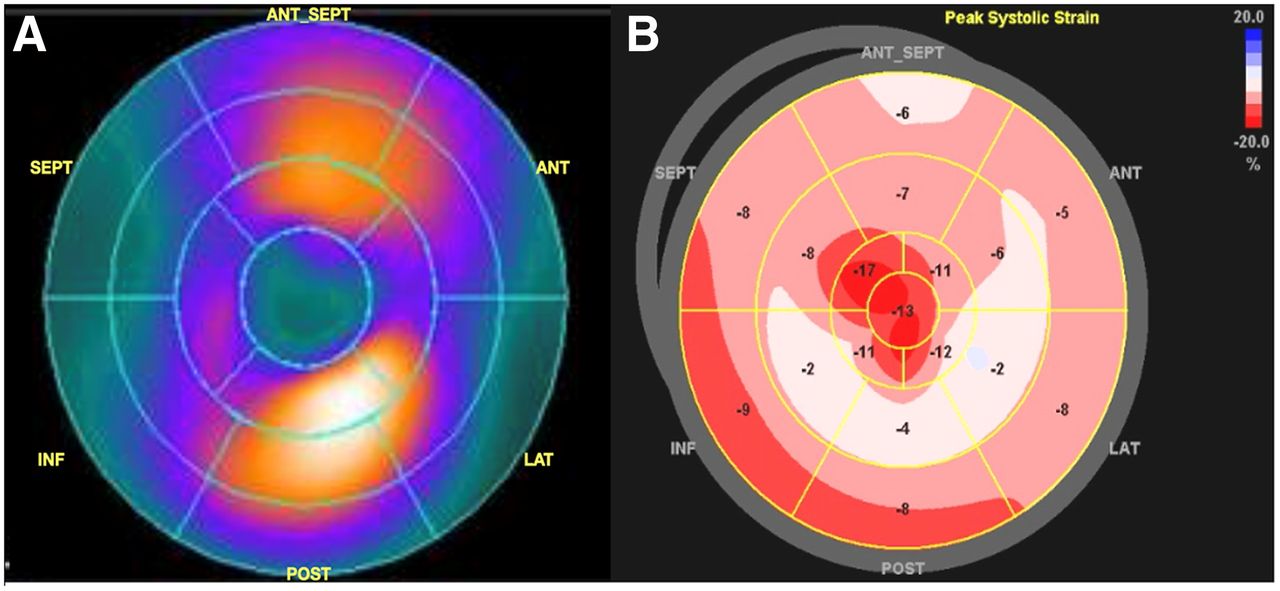
- FIGURE 1.
Side-by-side comparison of American Heart Association 17-segment model bull’s-eye color-mapping plots of 99mTc-PYP scan (A) and speckle-tracking strain imaging (B) in representative case with positive 99mTc-PYP findings. Panel A demonstrates intense LV myocardium uptake in anterior and inferior segments and no uptake at apex. Panel B demonstrates characteristic apex-sparing distribution pattern of peak LV longitudinal systolic strain. In this case, segments with uptake are associated with worse strain function. Values in panel B stand for segmental peak longitudinal systolic strain of each segment. ANT = anterior; INF = inferior; LAT = lateral; POST = posterior; SEPT = septal.
Tables
Demographic PYP+ (n = 22) PYP− (n = 42) Total (n = 64) P Age 81.0 (8.4) 72.0 (13.8) 75.1 (12.9) 0.002* Sex, male 22 (100.0%) 35 (83.3%) 57 (89.1%) 0.09† Body mass index 27.0 (3.5) 27.2 (5.3) 27.1 (4.8) 0.89* Systolic blood pressure (mm Hg) 119.8 (16.4) 136.6 (27.5) 130.6 (25.3) 0.029† Diastolic blood pressure (mm Hg) 73.7 (11.93) 80.5 (15.73) 78.1 (14.74) 0.070† Hypertension 12 (63.2%) 25 (73.5%) 37 (69.8%) 0.536† History of coronary artery disease 6 (31.6%) 10 (29.4%) 16 (30.2%) 1.000† History of diabetes mellitus 2 (10.5%) 10 (29.4%) 12 (22.6%) 0.174† β-blocker 10 (52.6%) 22 (64.7%) 32 (60.4%) 0.559† Calcium channel blocker 1 (5.3%) 9 (26.5%) 10 (18.9%) 0.076† Angiotensin-converting-enzyme inhibitor 3 (15.8%) 5 (14.7%) 8 (15.1%) 1.000† Angiotensin receptor blocker 5 (26.3%) 5 (14.7%) 10 (18.9%) 0.465† Spironolactone 4 (21.1%) 5 (14.7%) 9 (17.0%) 0.706† Amiodarone 0 (0.0%) 1 (2.9%) 1 (1.9%) 1.000† Creatine 1.3 (1.1–1.5) 1.3 (1.1–1.8) 1.3 (1.1–1.7) 0.44‡ N-terminal prohormone B-type natriuretic protein 3,095.0 (1,640.0–7,323.0) 3,097.0 (1,238.5–8,832.5) 3,097.0 (1,407.0–7,447.0) 0.99‡ Low voltage on electrocardiography 6 (28.6%) 5 (11.9%) 11 (17.5%) 0.1575† LV septal wall thickness (mm) 18.3 (2.96) 14.1 (3.43) 15.7 (3.83) 0.0001* LV posterior wall thickness (mm) 16.4 (2.63) 13.1 (2.99) 14.3 (3.28) 0.0004* LV mass (g) 352.3 (108.5) 272.4 (101.5) 300.7 (110.1) 0.005* LV mass index (g/m2) 175.7 (51.8) 137.2 (42.5) 150.4 (49.1) 0.002* LV End-diastolic diameter (mm) 44.5 (6.69) 47.2 (6.95) 46.2 (6.91) 0.143* Ejection fraction (%) 47.9 (15.2) 51.8 (15.2) 50.5 (15.2) 0.34* Stroke volume (mL) 65.6 (25.7) 76.4 (25.1) 72.5 (25.6) 0.1146‡ Cardiac index (L/m2/min) 2.4 (0.83) 2.8 (0.88) 2.6 (0.88) 0.075† Tricuspid annular plane systolic excursion by M-mode (mm) 12.3 (3.30) 17.2 (5.36) 15.8 (5.29) 0.0250‡ Pericardial effusion 8 (36.4%) 6 (14.3%) 14 (21.9%) 0.0584† Heart-to-contralateral ratio 1.7 (0.4) 1.1 (0.2) 1.3 (0.4) <0.001† PYP scale¶ 0 (0.0%) 30 (71.4%) 30 (46.9%) <0.001† 0 2 (9.1%) 7 (16.7%) 9 (14.1%) 1 6 (27.3%) 2 (4.8%) 8 (12.5%) 2 14 (63.6%) 3 (7.1%) 17 (26.6%) 3 0 (0.0%) 30 (71.4%) 30 (46.9%) * Unequal-variance 2-sample t test.
↵†Fisher exact test.
↵‡Wilcoxon rank-sum test.
↵¶Qualitative value for interpretation is determined by comparing uptake in myocardium. Grade 0 = no myocardial uptake, grade 1 = myocardial uptake less than bone uptake, grade 2 = myocardial uptake equal to bone uptake, grade 3 = myocardial uptake greater than bone uptake.
Qualitative data are number and percentage; continuous data are mean and SD or median and interquartile range.
Region PYP + (n = 22) PYP− (n = 42) Total (n = 64) P* Global (%) −10.5 (2.6) −13.1 (4.1) −12.2 (3.9) 0.003 Apex (%) −17.6 (4.7) −19.0 (6.5) −18.5 (5.9) 0.35 Mid (%) −9.6 (4.0) −11.7 (4.4) −11.0 (4.6) 0.07 Basal (%) −4.6 (2.6) −8.8 (4.0) −7.3 (4.1) <0.001 *2-sample t test.
- TABLE 3.
Segment-to-Segment Comparison in PYP+ Vs. PYP− Participants Using 17-Segment Model Individually
PYP− PYP+ Segment Region n Mean (%) n Mean (%) P* Basal Anterior 49 −8.5 (6.82) 12 −5.7 (4.31) 0.17 Anteroseptal 54 −13.3 (7.58) 8 −14.3 (6.86) 0.73 Inferoseptal 50 −19.3 (8.09) 9 −20.3 (7.55) 0.71 Inferior 44 −8.7 (6.44) 16 −3.3 (6.27) 0.006 Inferolateral 46 −11.7 (8.40) 15 −10.9 (6.51) 0.74 Anterolateral 51 −19.7 (8.63) 9 −11.8 (8.57) 0.01 Mid Anterior 45 −8.3 (6.00) 18 −6.3 (4.69) 0.20 Anteroseptal 40 −10 (5.92) 21 −8.4 (4.63) 0.31 Inferoseptal 41 −18.9 (8.91) 22 −18.0 (5.69) 0.61 Inferior 45 −9.4 (8.64) 18 −7.6 (6.12) 0.42 Inferolateral 48 −9.1 (6.12) 14 −7.9 (4.07) 0.52 Anterolateral 49 −16.4 (8.25) 14 −15.6 (6.44) 0.76 Apical Anterior 51 −12.4 (4.80) 12 −10.2 (3.09) 0.15 Septal 41 −13.1 (4.96) 22 −9.9 (2.85) 0.002 Inferior 42 −13.1 (4.90) 21 −9.7 (2.80) 0.001 Lateral 51 −12.4 (4.76) 12 −10.2 (3.31) 0.13 Apex 55 −12.2 (4.67) 8 −10.5 (3.83) 0.33 *2-sample t test.
Data in parentheses are SDs.
Parameter PYP+ (n = 22) PYP− (n = 42) Total (n = 64) P Presence of diastolic dysfunction 17 (77.3%) 15 (36.6%) 32 (50.0%) 0.002* Peak tricuspid regurgitation velocity (m/s) 2.7 (0.44) 2.9 (0.46) 2.8 (0.46) 0.176† Right ventricular systolic pressure (mm Hg) 40.3 (12.7) 44.1 (15.1) 42.8 (14.3) 0.3370‡ E-wave velocity (m/s) 0.9 (0.8–1.0) 0.8 (0.7–1.0) 0.9 (0.7–1.0) 0.70† A-wave velocity (m/s) 0.5 (0.3–0.7) 0.8 (0.6–0.9) 0.7 (0.5–0.9) 0.03† E/A ratio 2.0 (1.1–3.0) 1.2 (0.9–1.8) 1.3 (1.0–2.0) 0.06† E deceleration time (ms) 154.5 (140.0–189.0) 178.0 (139.0–205.0) 170.0 (140.0–205.0) 0.46† Tissue doppler medial e′ > velocity (cm/s) 3.3 (1.9) 4.7 (1.7) 4.2 (1.9) 0.009† Tissue doppler lateral e′ > velocity (cm/s) 4.4 (2.0) 6.3 (2.3) 5.6 (2.4) 0.009† E/e′ ratio medial 32.4 (18.3) 22.0 (12.1) 25.8 (15.3) 0.02‡ E/e′ ratio lateral 21.8 (9.2) 17.0 (10.3) 18.8 (10.1) 0.07‡
Supplemental Data
Files in this Data Supplement:





{kind=link}