


Abstract
We report a bladder diverticular stone with increased 99mTc-methyl diphosphonate uptake on bone scintigraphy and SPECT/CT. Diverticular stone is a known risk factor for bladder malignancy. The deposition of 99mTc-methyl diphosphonate on the crystal surface of the diverticular stone is a rare phenomenon but of clinical significance. Cystolitholapaxy is indicated to remove the diverticular stone and to reduce the risk of bladder cancer.
Uptake of 99mTc-methyl diphosphonate (MDP) in urolithiasis is an uncommon phenomenon and has been postulated as the radiotracer binding to the mineral crystal matrix on the surface of stones, which can be located in any portion of the renal collecting system. Multiple factors, including stone components, urinary stasis, and urinary tract infection, among others, may play a combined role in facilitating tracer accumulation on the surface of the stone, leading to its increased conspicuity on bone scintigraphy (1). We report a bladder diverticular stone with increased 99mTc-MDP uptake on bone scintigraphy and elucidate its clinical significance, which to our knowledge has not been described in the literature.
CASE REPORT
A 67-y-old man with biopsy-proven prostate cancer had a slowly rising level of prostate-specific antigen (PSA) while on androgen deprivation therapy. He was also experiencing symptoms of urinary retention due to prostatomegaly. To reevaluate tumor burden, the patient underwent contrast-enhanced CT of the abdomen and pelvis and 99mTc-MDP whole-body bone scintigraphy for a prostate cancer workup.
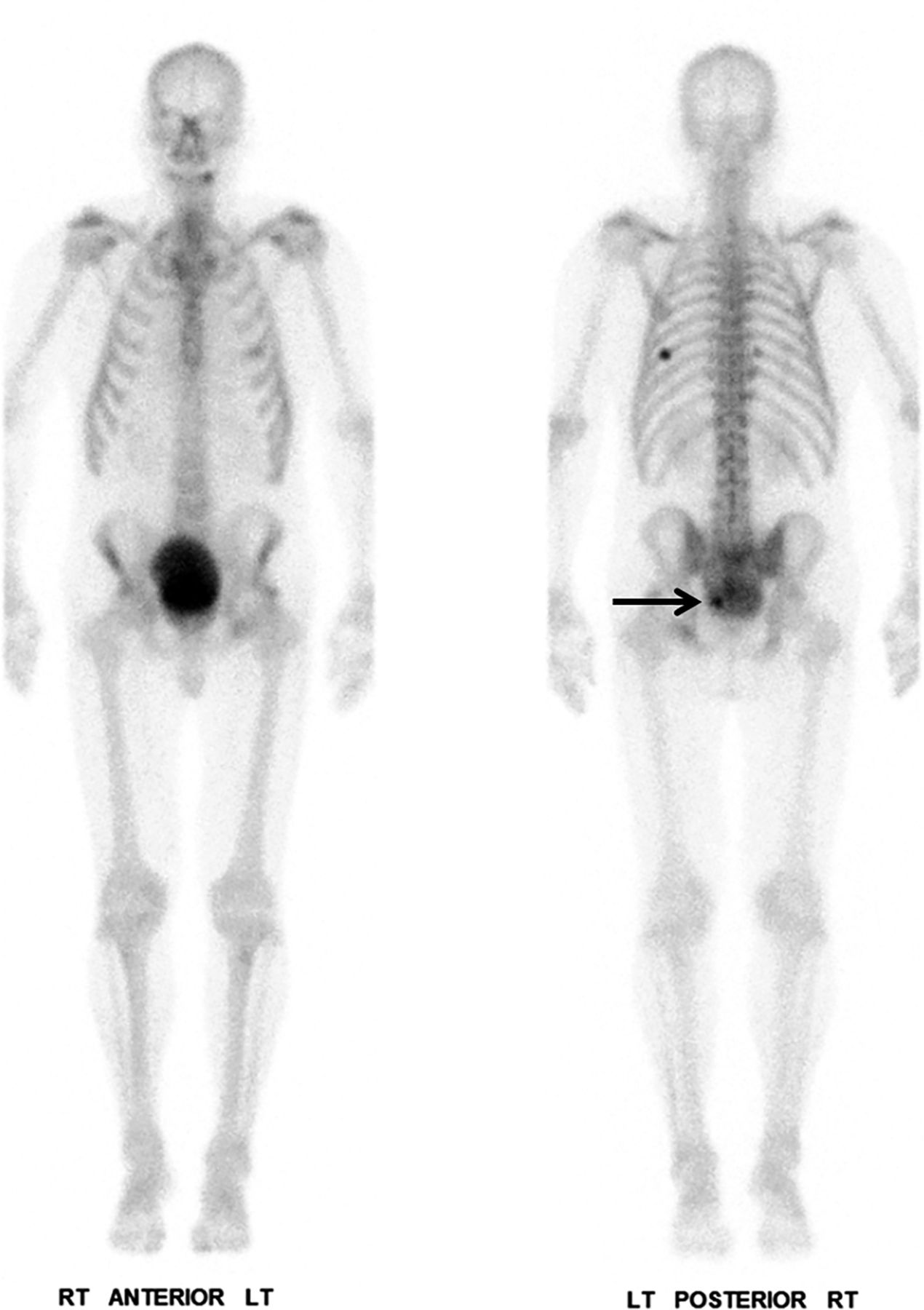
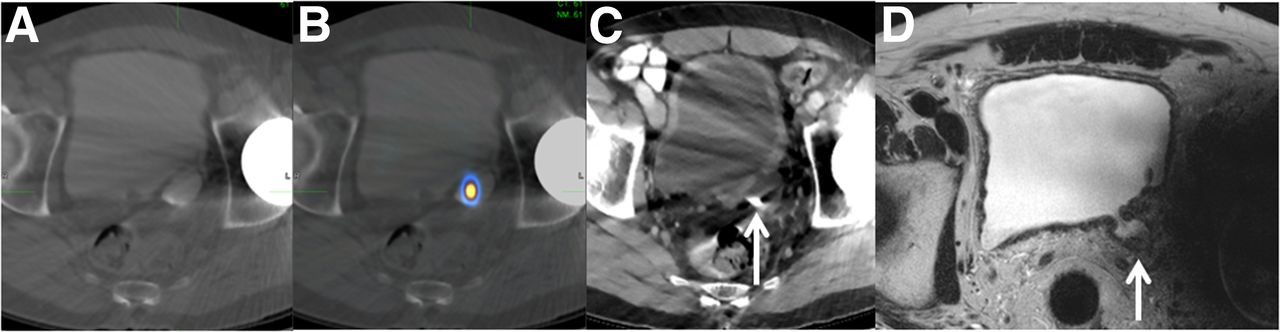
On the 99mTc-MDP planar images, there was focal intense uptake overlying the left part of the urinary bladder on the posterior view (Fig. 1). This focus corresponded to a tracer-avid stone retained in a left posterolateral bladder diverticulum, as seen on SPECT/CT images and pelvic MR images (Fig. 2). The patient subsequently underwent cystoscopy with transurethral resection of the prostate. Multiple bladder diverticula, with a retained stone at the left posterior bladder wall, were identified. Cystolitholapaxy was performed to remove the diverticular stone, followed by transurethral resection of the prostate to alleviate obstruction. Further analysis showed that the diverticular stone comprised 90% calcium phosphate and 10% calcium carbonate.
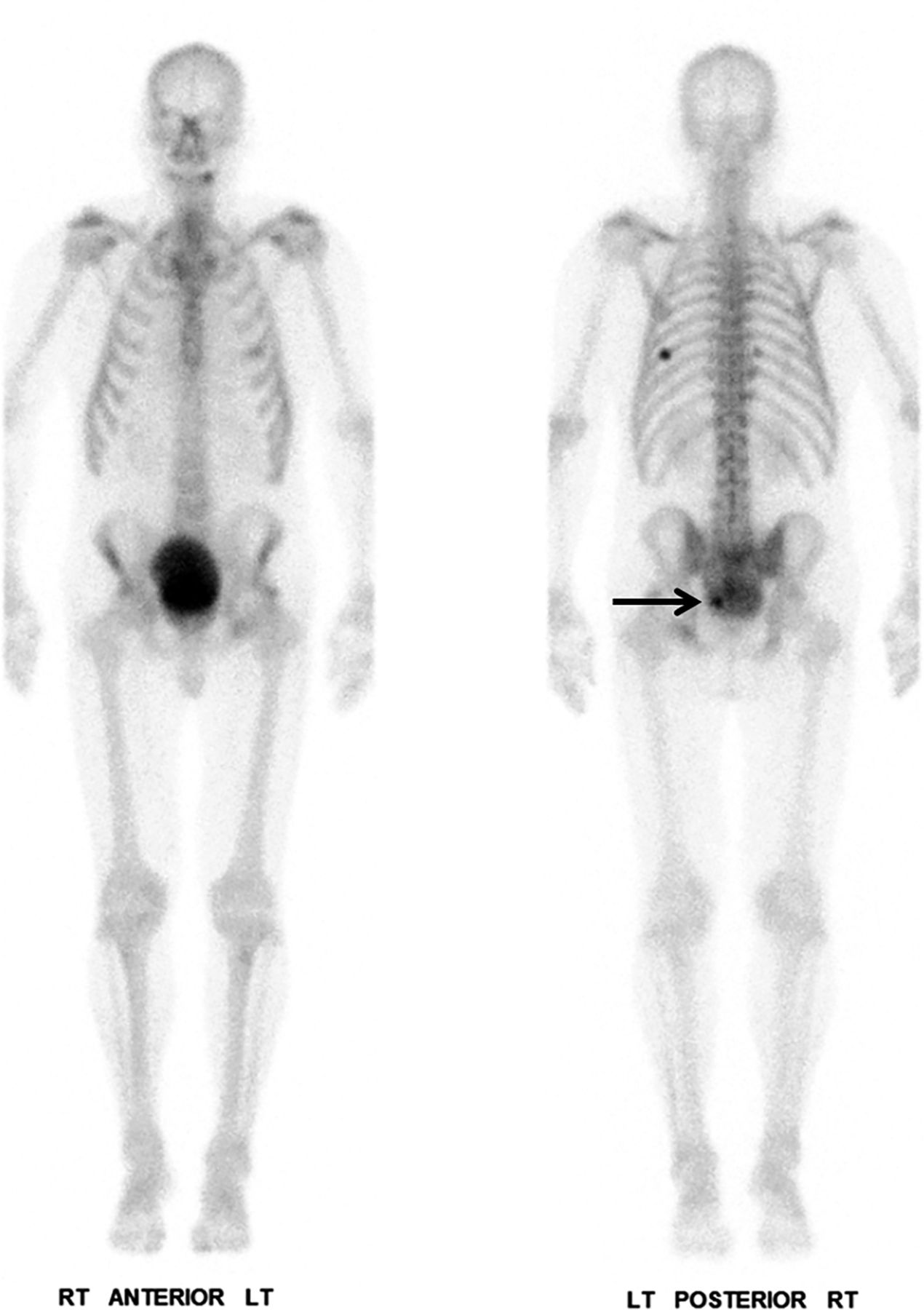
99mTc-MDP whole-body bone scan shows focal intense tracer uptake overlapping left aspect of urinary bladder, more evident on posterior view (arrow). Additional focus with increased tracer uptake in left posterior eighth rib corresponds to healing traumatic fracture.
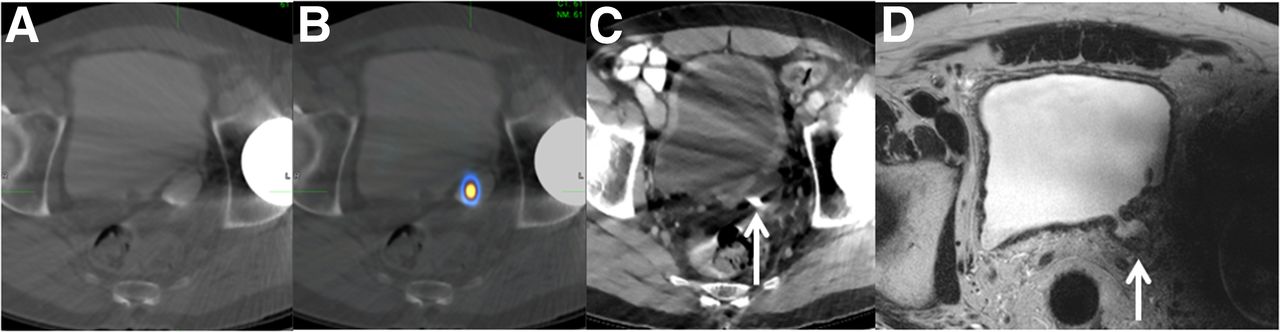
(A–C) 99mTc-MDP SPECT/CT images show excreted iodine contrast medium from earlier CT study filling bladder and diverticulum with focal uptake in diverticulum at left posterolateral bladder wall (A and B), corresponding to 1.0 × 0.8 cm high-density stone on same-day CT study (C, arrow). (D) Prostate MRI demonstrates left posterolateral bladder wall diverticulum (arrow). There is prominent beam-hardening artifact from metal hardware in left hip joint.
DISCUSSION
In adults, a bladder diverticulum may represent late recognition of a congenital process or mucosal herniation secondary to outflow obstruction, with an incidence of 1%–8% (2). The urine stasis in the diverticula may cause stone formation, urinary tract infection, and even tumors. The incidence of tumor in a diverticulum ranges from 2% to 10%, with transitional cell carcinoma being the most common type of malignancy and usually carrying a poorer prognosis due to lack of a smooth muscle layer in the diverticulum (3). There is an increased association between bladder stones and diverticular inflammation, which is recognized as a risk factor for bladder cancer; and long-standing bladder stones leading to chronic mechanical inflammation have been implicated in carcinogenesis (4).
CONCLUSION
In this case, although we could not determine the origin of the diverticular stone, we believe that the urinary stasis in the diverticulum might have advanced the 99mTc-MDP accumulation on the surface of the diverticular stone. The incidentally notable findings aid the urologist in surgical planning and may potentially prevent development of neoplasm.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Jun. 9, 2020.
- Received for publication March 12, 2020.
- Accepted for publication May 14, 2020.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.