


Abstract
Patients with multiple endocrine neoplasia type 1 usually have a combination of endocrine disorders due to lesions in the pancreas, parathyroid gland, and pituitary gland. Functional imaging using different tracers in addition to conventional imaging are applied in localizing the primary sites, determining the disease extent, and characterizing the lesions. We present a diagnosed case of multiple endocrine neoplasia type 1 with interesting incidental imaging findings showing 99mTc-sestamibi and 18F-fluorocholine uptake in addition to 68Ga-DOTANOC uptake in metastatic mediastinal and cervical lymph nodes arising from gastroenteropancreatic neuroendocrine tumor. This case shows the possibility of imaging the neuroendocrine tumors with 3 different tracers, namely 68Ga-DOTANOC, 99mTc-sestamibi, and 18F-fluorocholine.
Functional imaging using different tracers has been applied in localizing primary and metastatic sites, characterizing lesions, and determining the prognosis in patients with multiple endocrine neoplasia type 1 (MEN-1). These patients usually have a combination of lesions in the pancreas, parathyroid gland, and pituitary gland (1). 99mTc-sestamibi and the recently emerging 18F-fluorocholine are known functional imaging agents for localizing the eutopic and ectopic parathyroid lesions, although the mechanism for 99mTc-sestamibi uptake is essentially different from that for 18F-fluorocholine uptake in parathyroid lesions (2,3). Whole-body 68Ga-somatostatin receptor (SSTR) imaging has been efficiently used in detecting neuroendocrine tumors (NETs) with increased SSTR expression (4). However, functional imaging showing avid metastatic disease with these tracers has not, to our knowledge, been reported before. We present a diagnosed case of MEN-1 syndrome with interesting incidental imaging findings showing 99mTc-sestamibi and 18F-fluorocholine uptake in addition to 68Ga-DOTANOC uptake in metastatic cervical and mediastinal lymph nodes arising from gastroenteropancreatic NETs. The possibility of imaging NETs with 3 different tracers having different mechanisms of uptake, namely 68Ga-DOTANOC, 99mTc-sestamibi, and 18F-fluorocholine, may improve our understanding of tumor biology.
CASE REPORT
A 44-year-old man presented with complaints of an increased frequency of stools along with unexplained loss of weight and appetite for the previous 3 months. Biochemical investigations revealed elevated levels of serum parathyroid hormone (110.8 pg/mL; reference value, 15–65 pg/mL), calcium (10.9 mg/dL; reference value, 8.6–10.2 mg/dL), gastrin (>10,000 pg/mL; reference value, 13–115 pg/mL), and chromogranin (>1,400 ng/mL; reference value, 0–98.1 ng/mL) and a lowered level of serum phosphate (1.4 mg/dL; reference value, 2.7–4.5 mg/dL mg/dL). Neck ultrasonography showed a hypoechoic lesion in the superior aspect of the right lobe of the thyroid. Endoscopy-guided biopsy samples of polypoidal lesions in the stomach and duodenum revealed well-differentiated NET. MRI of the brain revealed a lesion in the sella, suggestive of macroadenoma. The diagnosis of MEN-1 syndrome was made with MEN1 gene analysis.
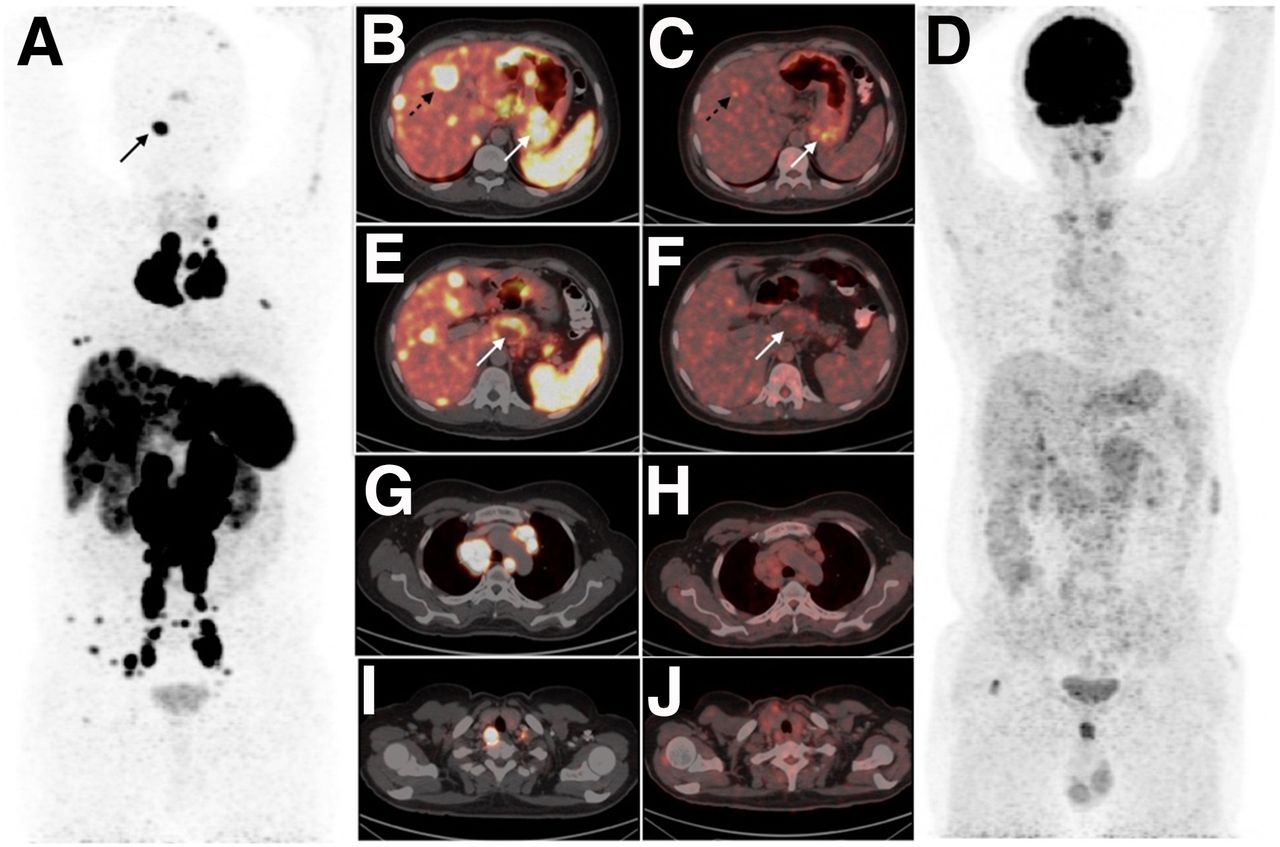
99mTc-sestamibi planar and SPECT/CT imaging performed because of the hyperparathyroidism was suggestive of bilateral superior parathyroid adenomas and showed tracer-avid enlarged mediastinal and cervical lymph nodes (Fig. 1). Regional neck 18F-flurocholine PET/CT performed for further clarification was also suggestive of bilateral superior parathyroid adenomas, as well as showing intense tracer-avid enlarged mediastinal and cervical lymph nodes (Fig. 1). The patient underwent bilateral parathyroidectomy, and histopathologic examination revealed parathyroid adenomas, with normalization of serum parathyroid hormone and calcium levels in the postoperative period.

(A and D) Early and delayed static images of 99mTc-sestamibi scintigraphy performed for hyperparathyroidism showing 2 foci of increased tracer uptake with retention near upper poles of both lobes of thyroid gland (solid arrows). (G and B) Early SPECT maximum-intensity projection image and coronal fused SPECT/CT image localizing increased tracer uptake in 2 lesions in posterosuperior location of both lobes of thyroid gland (solid arrows) suggestive of parathyroid adenomas. (A, B, D, E, G, and H) 99mTc-sestamibi planar and SPECT/CT images showing tracer avidity in the enlarged mediastinal and cervical lymph nodes (dashed arrows). (C, F, I, and J) Regional neck 18F-fluorocholine PET maximum-intensity projection image and cross-sectional fused PET/CT images showing tracer-avid lesions near upper poles of thyroid lobes, suggestive of bilateral superior parathyroid adenomas (solid arrows) along with intense tracer-avid enlarged mediastinal and cervical lymph nodes (dashed arrows).
Whole-body 68Ga-DOTANOC and 18F-FDG PET/CT were performed for extent-of-disease determination and for differentiation and prognostication to plan for peptide receptor radionuclide therapy because of the widespread metastatic disease. 68Ga-DOTANOC PET/CT images showed an SSTR-expressing tracer-avid primary tumor in the stomach and duodenum with extensive metastatic disease, whereas the same lesions showed low-grade 18F-FDG avidity on 18F-FDG PET/CT (Fig. 2).
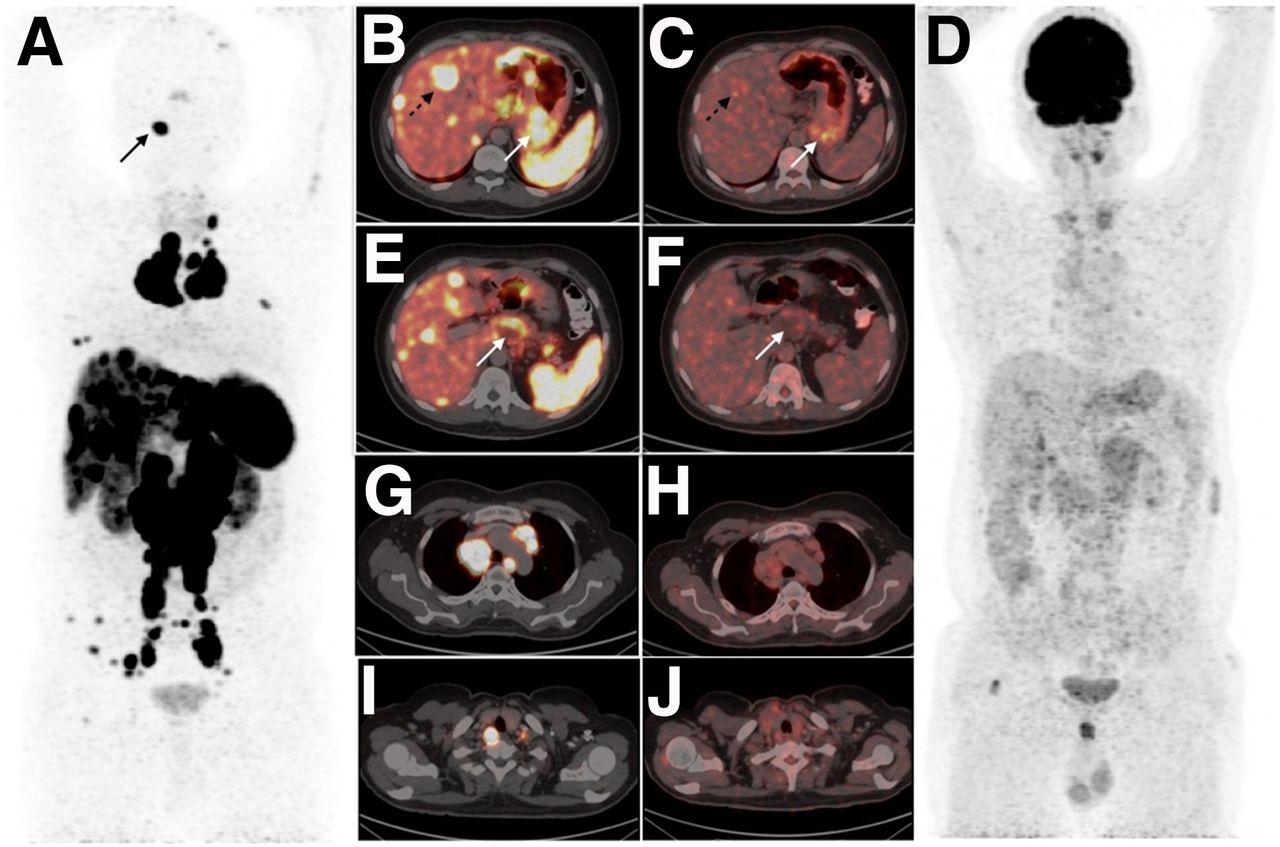
(A) 68Ga-DOTANOC PET maximum-intensity projection image showing SSTR-expressing extensive metastatic disease of neuroendocrine origin. (B, E, G, and I) Transaxial fused 68Ga-DOTANOC PET/CT images showing intensely tracer-avid lesions in stomach and liver (B; solid and dashed arrows); cystic lesion in pancreas (E; arrow); and multiple enlarged lymph nodes in mediastinum (G) and cervical regions (I). (C, D, F, H, and J) 18F-FDG PET maximum-intensity projection image (D) and corresponding transaxial fused 18F-FDG PET/CT images (C, F, H, and J) showing low-grade 18F-FDG avidity in the above-mentioned lesions suggestive of well differentiated nature of the disease.
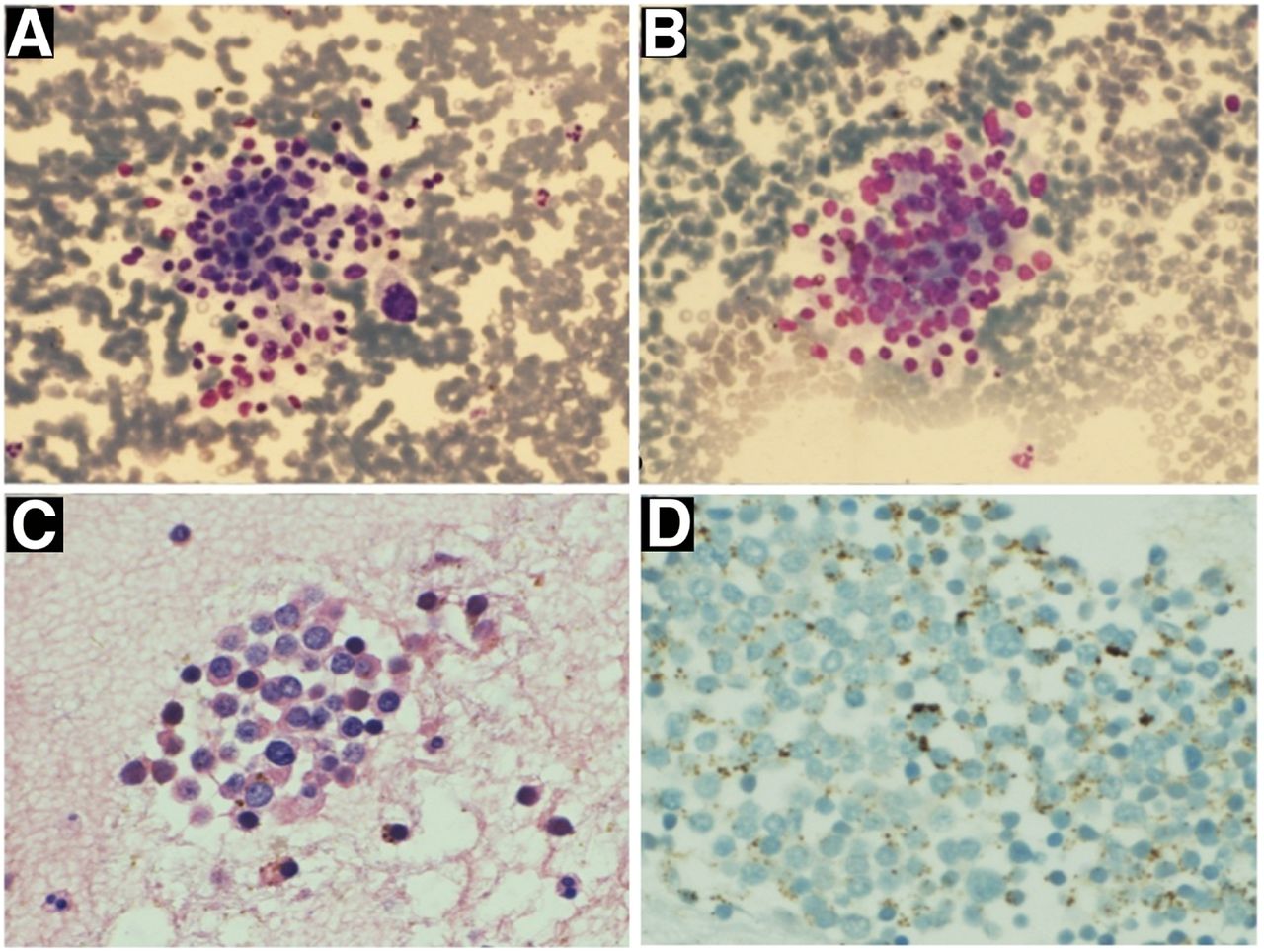
Ultrasound-guided fine-needle aspiration cytology from an enlarged cervical lymph node revealed metastatic NET with a Ki-67 proliferation index of less than 2% (Fig. 3). The patient underwent 2 cycles of 177Lu-DOTATATE therapy (7.4 GBq infusion along with amino acid protection at an 8-week interval). The patient showed significant clinical improvement, was being followed up for further treatment, and had not experienced any adverse renal or hematologic toxicity. The whole-body posttherapy scan showed tracer-avid lesions similar to those seen on the 68Ga-DOTANOC scan (Fig. 4).
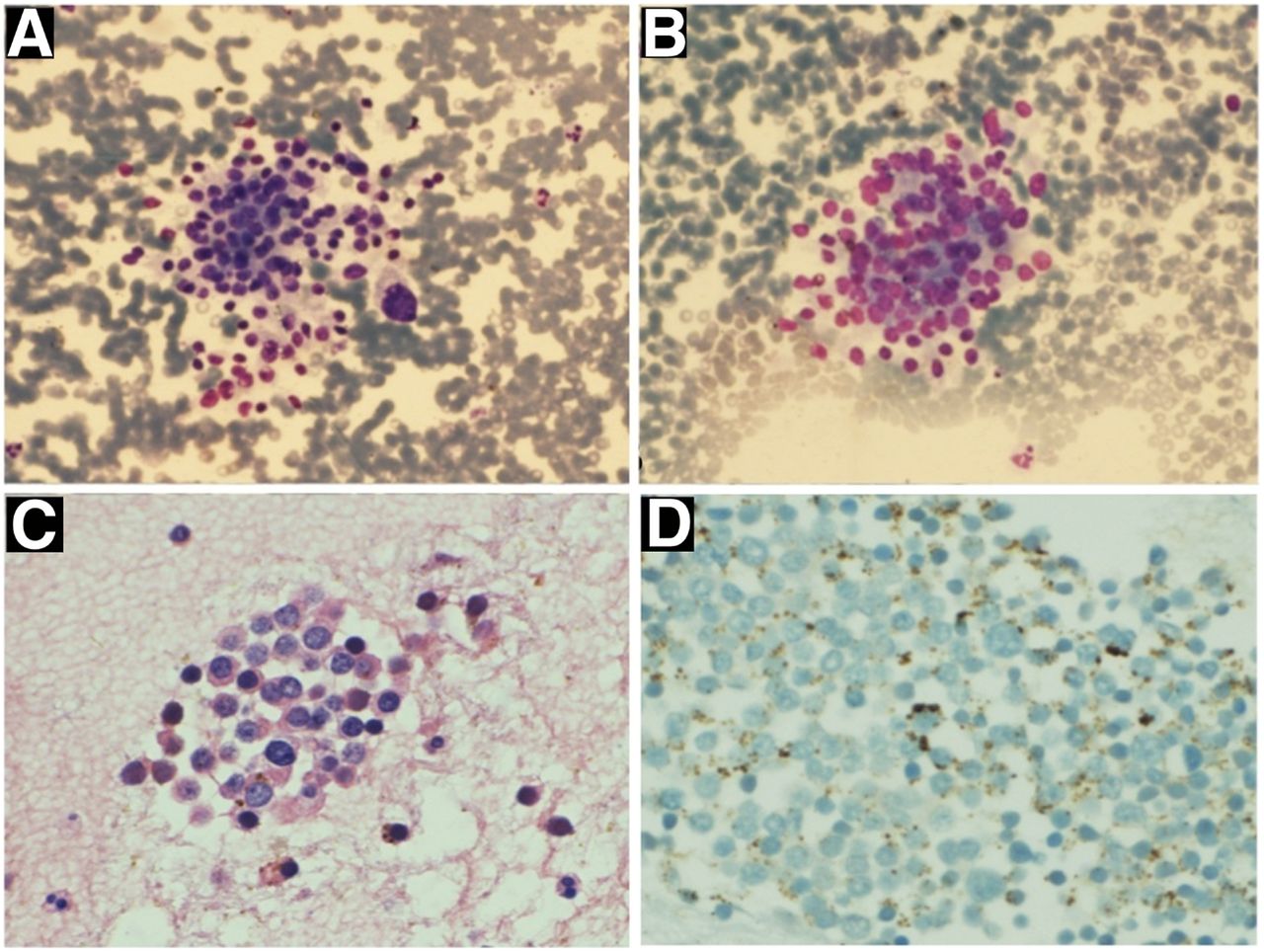
(A and B) Ultrasonography-guided fine-needle aspiration cytology from enlarged cervical lymph node revealing clusters of tumor cells with mildly pleomorphic nuclei, showing sudden anisonucleosis (May–Grünwald staining, ×20). (C) Additional cluster of tumor cells with stippled chromatin and moderate amount of cytoplasm (hematoxylin and eosin staining, ×20) suggestive of metastatic NET. (D) Immunocytochemistry for Ki-67 proliferation index was found to be less than 2%.
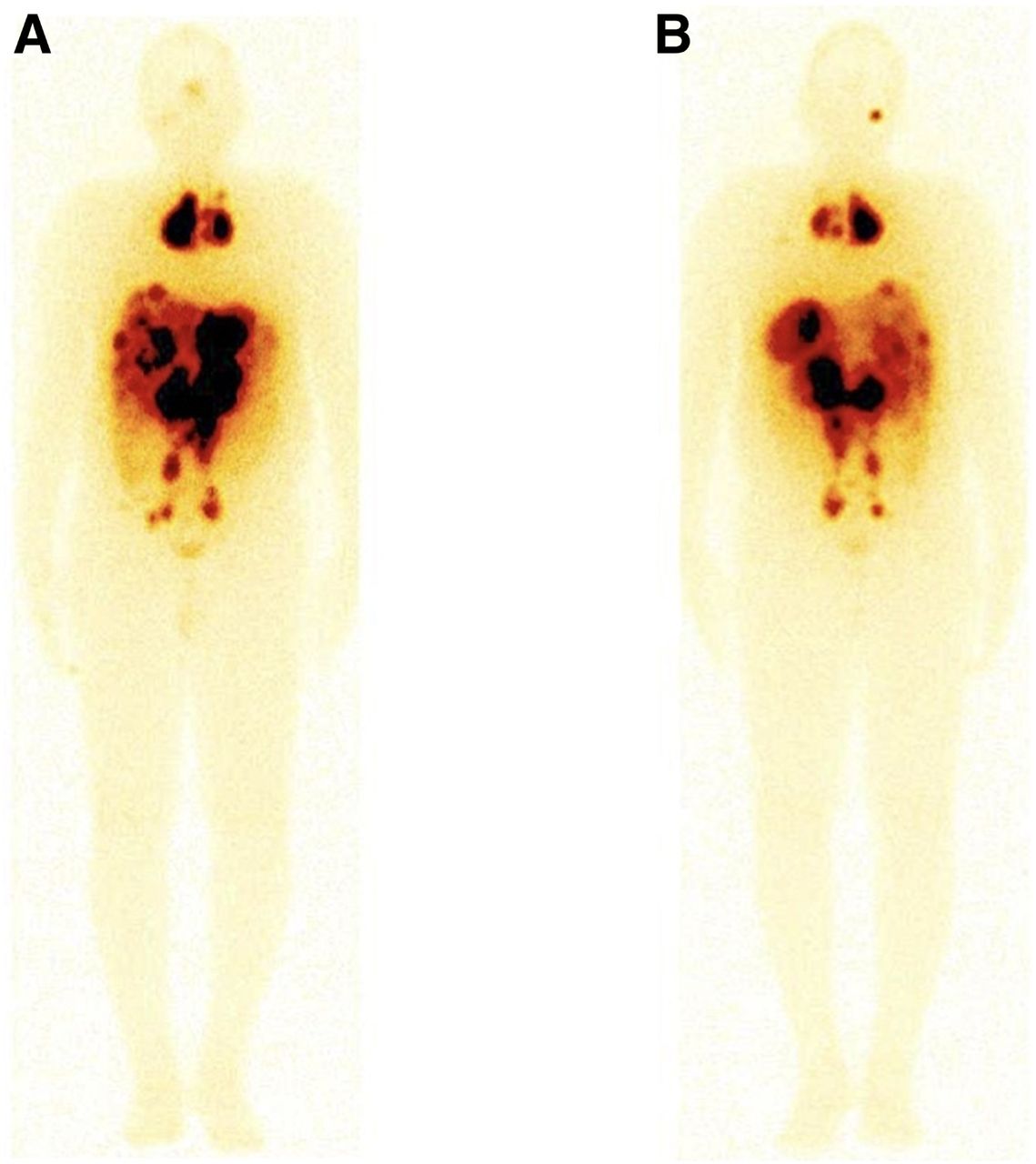
Whole-body anterior (A) and posterior (B) posttherapy images (177Lu-DOTATATE therapy; first cycle) showing tracer avidity in the lesions of metastatic neuroendocrine tumor.
DISCUSSION
MEN-1 is an autosomal dominant disease secondary to mutations of the tumor suppressor gene MEN1, with the occurrence of pituitary, parathyroid, and pancreatic tumors and a wide spectrum of clinical presentations. Evaluation of the organs involved and of the localization and extent of disease is required before the specific therapy can be planned (1).
The different methods of functional imaging reflect the diverse characteristics of the tumor. Cellular 99mTc-sestamibi uptake is dependent on mitochondrial overexpression, whereas 18F-fluorocholine uptake indicates increased choline kinase activity and phosphatidyl choline synthesis. Both tracers have been used for presurgical localization of parathyroid adenoma (2,3). SSTR type 2 overexpression is known to occur in gastropancreatic NETs, making them suitable for theranostics with SSTR-labeled radionuclides (4). 18F-FDG imaging reflects cellular metabolism with a higher metabolic rate, indicating poorer prognosis (5).
Few case reports have shown increased 99mTc-sestamibi uptake in primary malignant and metastatic NETs such as carcinoid tumors, paragangliomas, and primary neuroendocrine neoplasms (6–8). In a case series of 3 bronchial carcinoids having low Ki-67 (nonaggressive neoplasm), 18F-fluorocholine showed tumor avidity, which was secondary to cholinergic autocrine loop overexpression and high turnover of intracellular vesicles (9). We present the current MEN-1 case showing avidity with 3 different tracers (68Ga-DOTANOC, 99mTc-sestamibi, and 18F-fluorocholine) because of different uptake mechanisms, highlighting the diverse characteristics of the tumor.
CONCLUSION
This case report shows that radiopharmaceuticals having different mechanism of uptake in gastroenteropancreatic NET with widespread lymph node metastases may better explain the underlying tumor biology.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Feb. 28, 2020.
REFERENCES
- Received for publication September 25, 2019.
- Accepted for publication December 11, 2019.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.