


Article Figures & Data
Figures
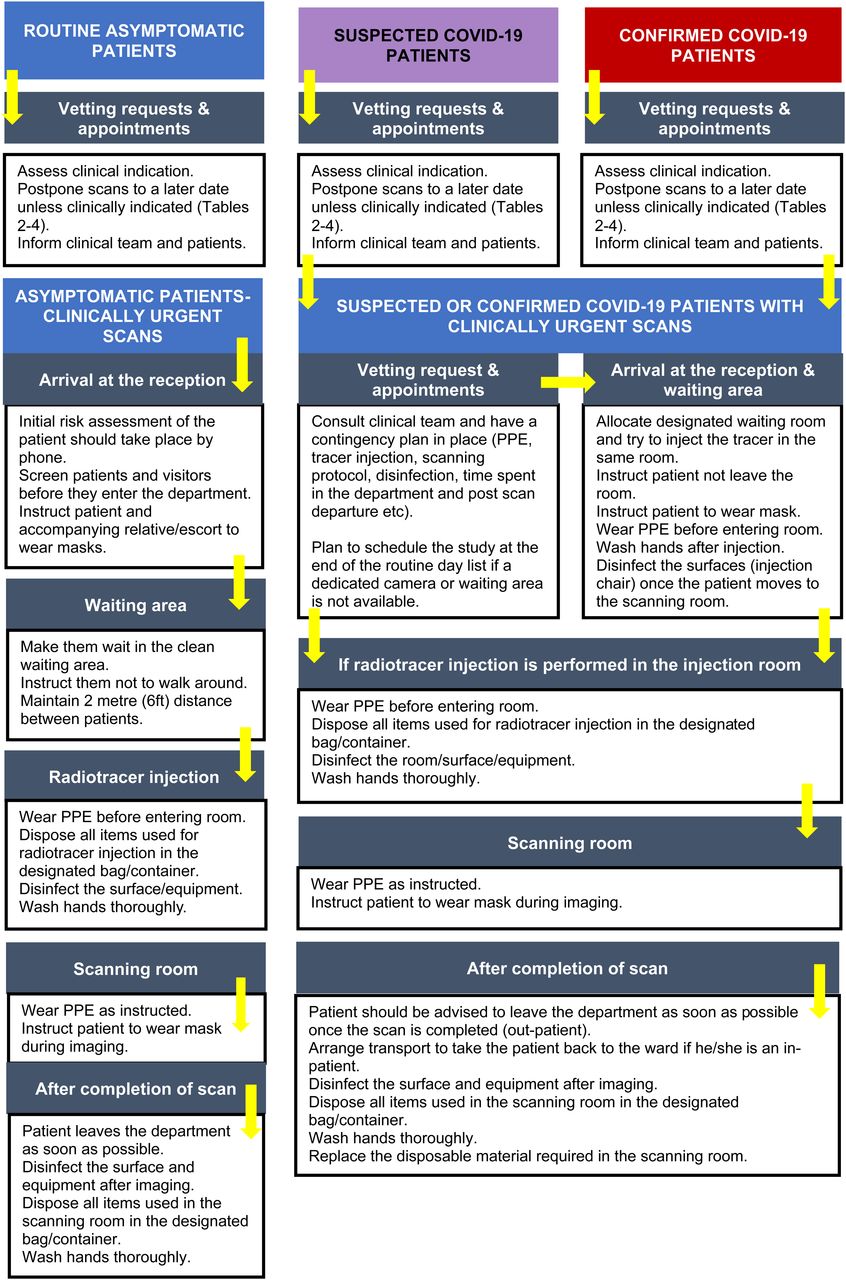
- FIGURE 1.
Basic contingency for nuclear medicine imaging. (Adapted from (41).)
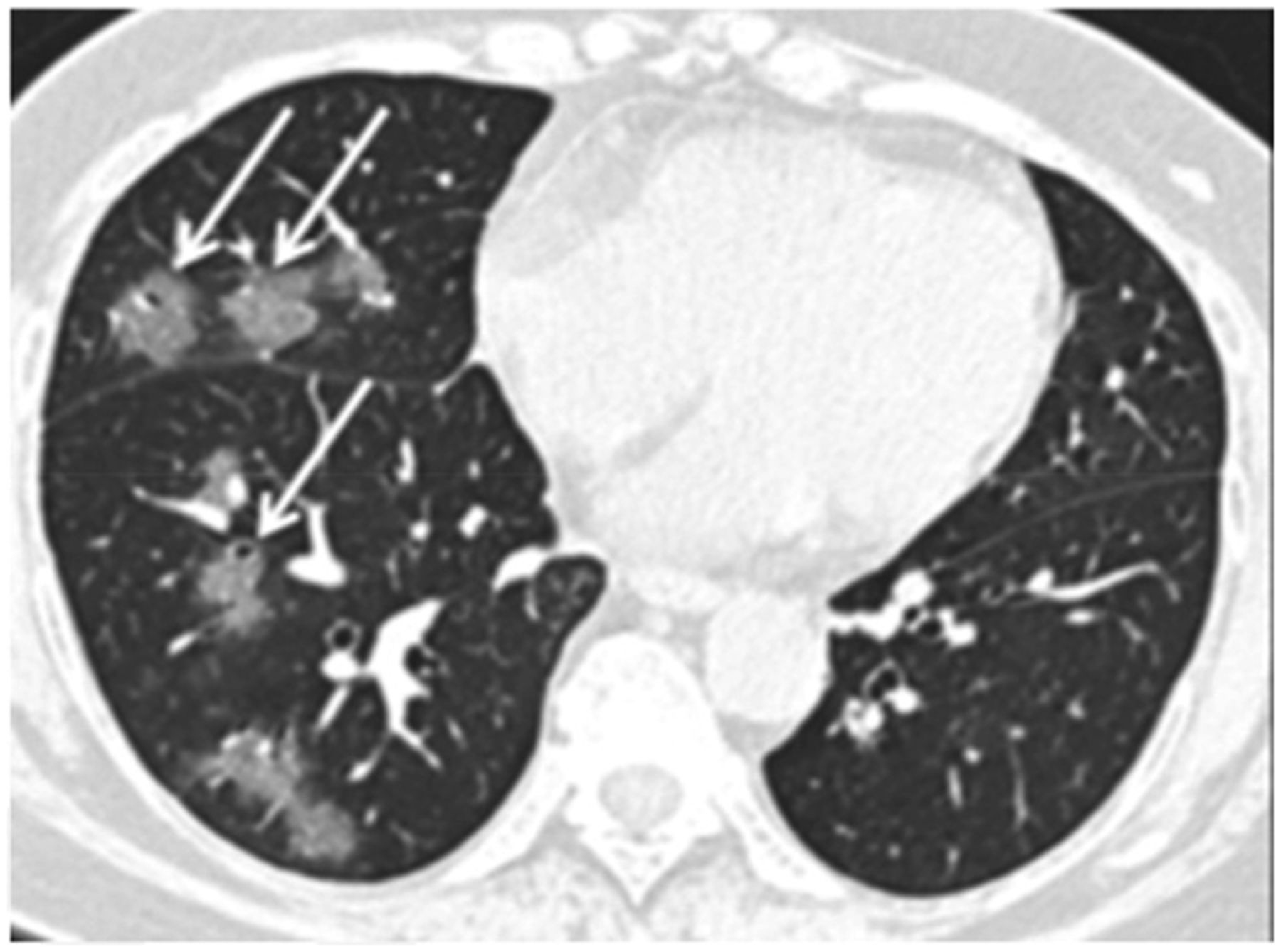
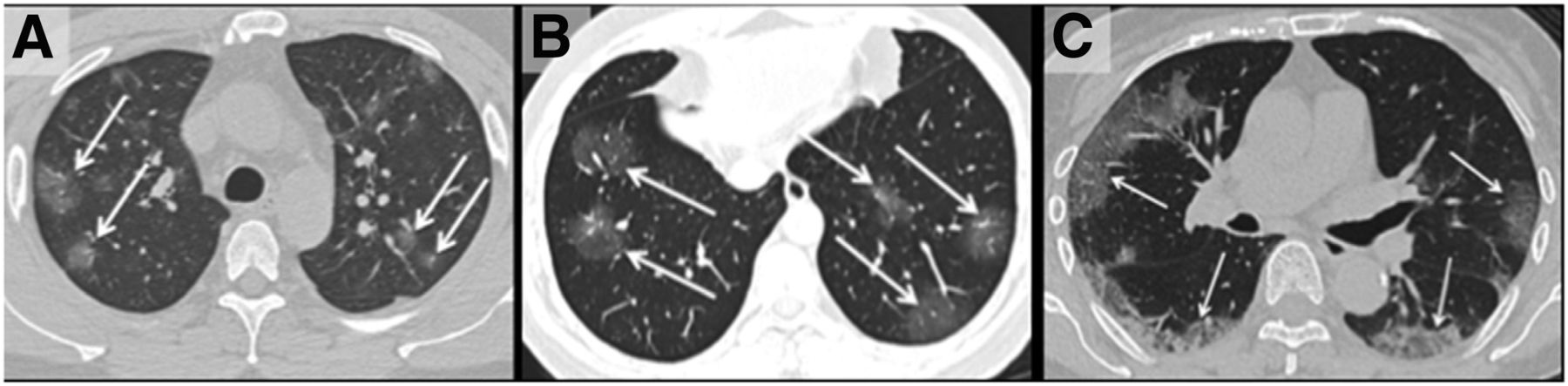
- FIGURE 2.
(A) Unenhanced axial CT image from 36‐year‐old man shows bilateral ground‐glass opacities in upper lobes with rounded morphology (arrows). (B) Axial CT image from 44‐year‐old man shows larger ground-glass opacities bilaterally in lower lobes with rounded morphology (arrows). (C) Axial CT image from 65‐year‐old woman shows bilateral ground‐glass and consolidative opacities with striking peripheral distribution. (Reprinted with permission of (32).)
- FIGURE 3.
Unenhanced axial CT image from 56‐year‐old woman shows ground‐glass opacities with rounded morphology (arrows) in right middle and lower lobes. Left lung was normal. (Reprinted with permission of (32).)
- FIGURE 4.
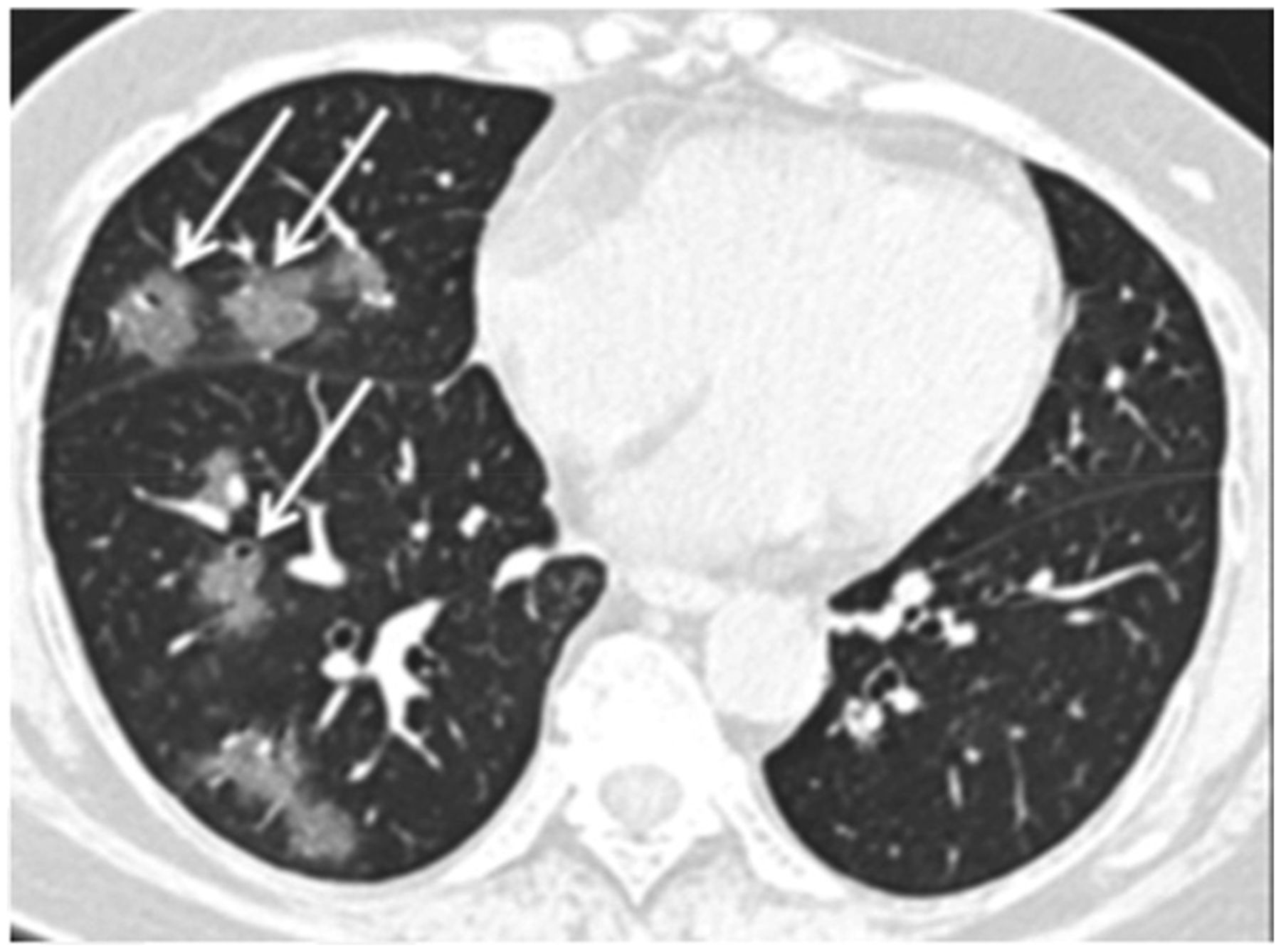
Unenhanced axial CT image from 42‐year‐old man in late time group (10 d from symptom onset to this scan) shows bilateral consolidative opacities with striking peripheral distribution in right lower lobe (solid arrows) and with rounded morphology in left lower lobe (dashed arrow). (Reprinted with permission of (32).)
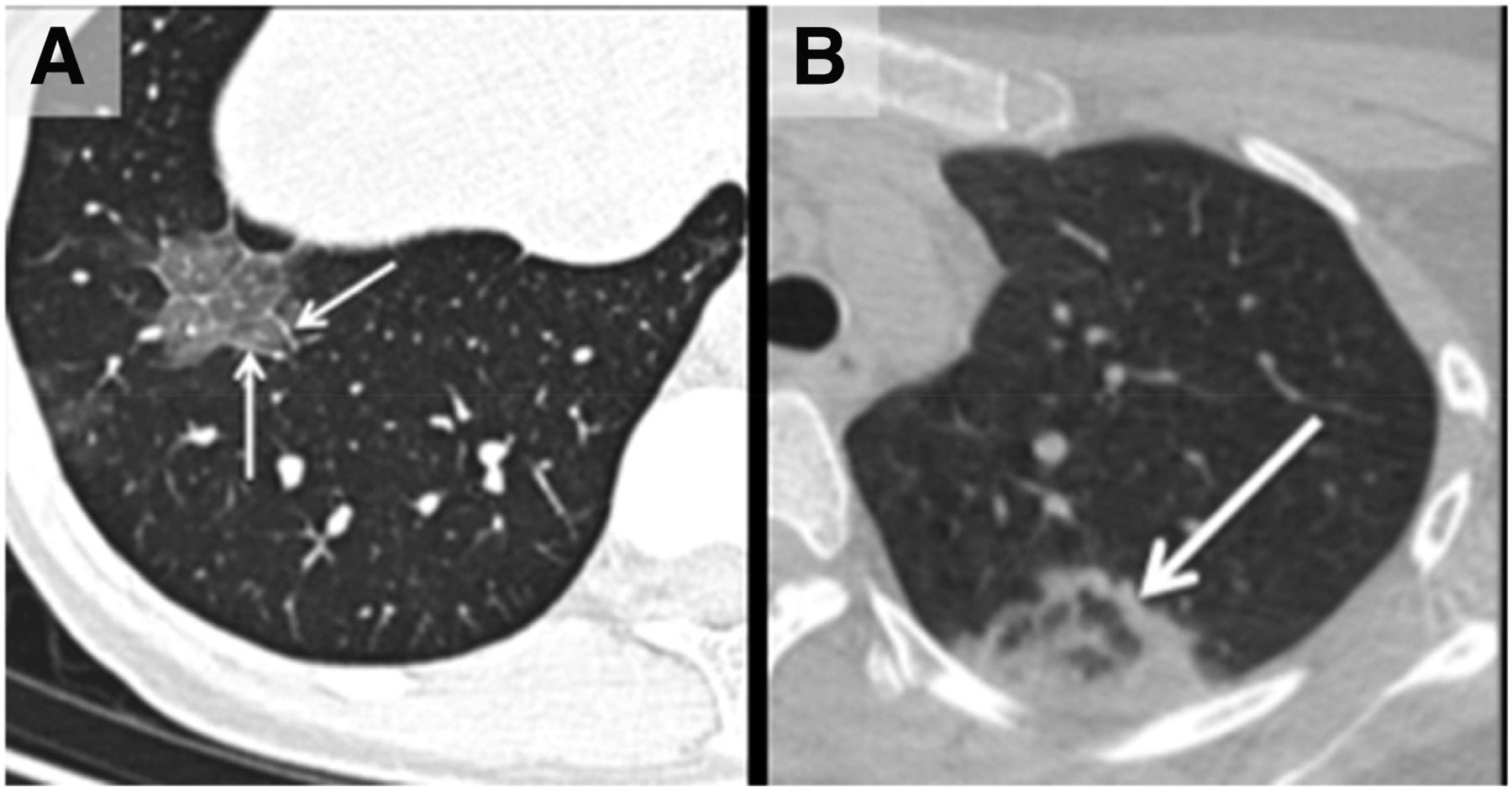
- FIGURE 5.
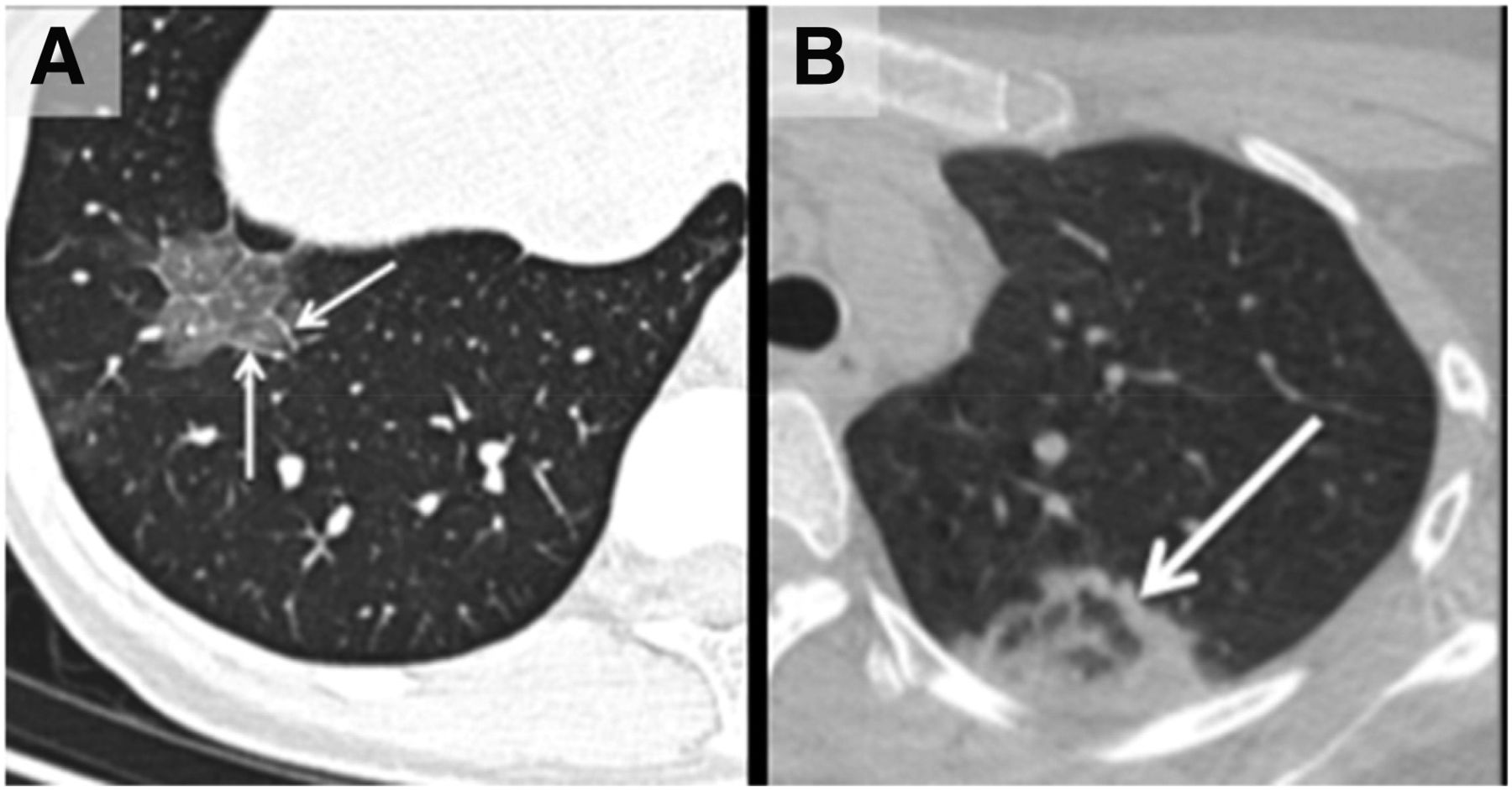
(A) Unenhanced axial CT image from 43-y-old woman shows crazy‐paving pattern as manifested by right-lower-lobe ground‐glass opacification with interlobular septal thickening (arrows) and intralobular lines. (B) Axial CT image from 22‐year-old woman shows area of faint ground‐glass opacification in left upper lobe, with ring of denser consolidation (arrow, reverse halo sign). (Reprinted with permission of (32).)


Tables
- TABLE 1
Consensus Guidance for Nuclear Medicine Departments, Staff, and Patients (6,17,20–25)
Managing nuclear medicine department Nuclear medicine staff Patients attending nuclear medicine center Promote and practice social distancing (2 m or 6 ft) Train in infection control Screen patients and visitors before they enter department Assess risk at local level, with local context taken into consideration (should not replace or reduce ability to provide optimal patient or staff safety) Promote and practice social distancing (2 m or 6 ft) Make initial risk assessment of patient by phone, when possible Coordinate transmission of information between hospital information control department and nuclear medicine department Minimize crowding in workplace (e.g., tea or lunch breaks) Ask patients to inform nuclear medicine department if patient or family members develop symptoms before scheduled appointment Ask referring clinicians to clearly indicate whether scans are urgent or nonurgent when requesting them Maintain (6 ft or 2 m) distance in all patient and staff interactions when possible Display posters in department reception area to promote hand washing and good respiratory hygiene measures Train all staff members to ensure maximum compliance and vigilance in line with local guidance Consider need for contact and droplet precautions (based on nature of task being undertaken) Promote social distancing (2 m or 6 ft) Provide clear guidance to staff on how to proceed when patient COVID-19 status is unknown and COVID-19 is circulating at high levels Practice strict hand hygiene, which should be extended to exposed forearms, after removing any element of PPE Recommend patient use of fluid-resistant surgical face mask (to minimize dispersal of respiratory secretions and to reduce both direct transmission risk and environmental contamination) Establish local policy to reschedule nonurgent appointments Have access to PPE Ask patients to maintain strict hand hygiene Display posters to promote hand washing and good respiratory hygiene measures within department Train on donning and doffing PPE Ask patients to minimize accompanying visitors and patient escorts Allocate or make provision for separate space for patients with suspected or known COVID-19 status Put on appropriate PPE before providing care Give patients telehealth option (teleclinics to provide reassurance and guidance) Develop clear escalation pathway to ensure cases are identified in timely manner and triaged Know what PPE staff should wear for each setting and context Inform and reschedule nonurgent appointments Implement stringent local hospital policy for screening of staff, patients, and visitors before they enter department Adopt single-use policy for gloves and aprons Inform and reschedule elective therapies Implement stringent local hospital policy to minimize nonessential visitors in department Take regular breaks and rest periods Ensure that patients spend minimum time in department (do not allow patients to remain for long periods in waiting area) Provide PPE for staff and patients (because of concern about asymptomatic transmission of COVID-19) Remain connected with rest of staff or with friends and family via group email, e-portal or social media Make sure supplies are available, and check stock every day and during day (centralize storage and distribution) Make sure nuclear medicine physicians or radiologists are familiar with CT appearance of COVID-19 Implement robust policy for cleaning and decontaminating imaging equipment Check PET/CT and SPECT/CT scans for CT changes in lungs before sending patient home Explore options and encourage reporting of scans from remote sites or home, whenever feasible, according to local policy Be supportive and caring; nominate staff to look after staff well-being Encourage use of virtual conference tools for multidisciplinary or educational meetings Provide for flexible staff-schedule rotation (on-site and off-site work, work in small groups) Provide relevant, regular, and reliable updates daily Develop contingency and business continuity plan These are examples based on consensus only, and responsibility lies with each institution or hospital to ensure its written policy adheres to that outlined by national public health guidance in its respective country and hospital.
Type of scan (referrals must be reviewed by nuclear medicine consultant) Scans that can be booked and performed as requested (unless patient is at risk of infection) Scans that require liaison with clinical team for canceling or rescheduling (inform patient) Scans that must be postponed or rescheduled (inform patient and clinical team) Skeletal Bone scans in cancer patients Scans for severe pain pre- and postprocedural orthopedic indications (if there is a question of infection, offer 18F-FDG PET/CT as alternate) Scans for pre- and postprocedural orthopedic indications; metabolic bone disease; inflammatory arthropathy Endocrine 99mTc04 thyroid scans in patients not on antithyroid medications or if question of ectopic or neonatal hypothyroidism 99mTc04 thyroid scans in patients on antithyroid medications; 99mTc-MIBI parathyroid scans for preoperative localization Cardiovascular (avoid exercise nuclear stress testing because of risk of droplet exposure; consider using pharmacologic stress agents; consider 1-d protocols (e.g., stress–rest) Myocardial perfusion scans in cases of recent acute coronary syndrome (moderate- to high-risk patients) for urgent coronary revascularization; scans in patients with new or increasing chest pain; scans for preoperative assessment (moderate- to high-risk patients); MUGA scans in oncology patients (before initiation of or subsequent chemotherapy) Myocardial perfusion scans in patients awaiting liver transplant surgery; scans in patients with stable angina requiring follow-up evaluation; cardiac amyloid DPD scans 123I-MIBG heart scans; myocardial perfusion scans in patients awaiting renal transplant surgery; cardiac amyloid DPD scans for follow-up evaluation Brain DaTscan (123I-FP-CIT) scans Respiratory (discuss decision to proceed with ventilation–perfusion scan with referrer before booking) Lung perfusion scans in pregnant patients; lung shunt scans for 90Y-SIRT Ventilation–perfusion scans in patients with pulmonary hypertension or chronic PE on treatment Ventilation–perfusion scans if question of resolution of PE in patients receiving thromboprophylaxis Gastrointestinal Gastrointestinal-bleed Meckel scans Gastric-emptying esophageal transit scintigraphy; gastroesophageal reflux scintigraphy; SeHCAT small-bowel or colonic transit scans Hepatobiliary HIDA scans in patients with biliary leak HIDA scans if question of acute cholecystitis Liver or spleen scans; HIDA scans in patients with, for example, cystic duct syndrome or sphincter-of-Oddi dysfunction; liver SPECT in patients with hemangioma; 99mTc-denatured RBC scans Genitourinary 99mTc-DMSA scans in patients with radiotherapy to abdomen or prior renal surgery; 99mTc-MAG3 scans in patients with urinary leak or transplant rejection; testicular scans in patients with torsion MAG3 scans if question of obstruction; DMSA scans for donor assessment 99mTc-MAG3 scans for routine follow-up; 99mTc-DMSA scan for follow-up; captopril renogram scans Infection or inflammation Scans if question of sepsis in COVID-19–negative patients (suggest FDG PET/CT); scans if question of infection of prosthesis Lymphatic system Sentinel lymph node injections and scans Lymphoscintigram scans if question of lymphedema Oncology 111In-pentetreotide and 99mTcEDDA/HYNIC-Tyr3-Octreotide scans before PRRT Octreotide/Tektrotyd scans in patients with NET; 123I-MIBG scans in patients with pheochromocytoma or paraganglioma Miscellaneous GFR studies in oncology patients before initiation of or subsequent chemotherapy Dacryoscintigraphy scans; salivary gland scintigraphy; DXA scans Referrals must be reviewed by nuclear medicine consultants or in multidisciplinary setting. These are examples based on consensus only, and responsibility lies with each institution or hospital to ensure its written policy adheres to that outlined by national public health guidance in its respective country and hospital.
99mTc04 = 99mTc-pertechnetate; MIBI = methoxyisobutylisonitrile; MIBG = metaiodobenzylguanidine; DPD = 3,3-diphosphono-1,2-propanodicarboxylic acid; [123I]β-CIT = [123I]2β-carboxymethoxy-3β-(4-iodo-phenyl)tropane; [123I]FP-CIT = [123I]N-ω-fluoropropyl-2β-carbome-thoxy-3β-(4-iodophenyl)nortropane; MUGA = multigated acquisition; SIRT = selective internal radiation therapy; PE = pulmonary embolism; HIDA = hepatobiliary iminodiacetic acid; SeHCAT = selenium homocholic acid taurine; GFR = glomerular filtration rate; MAG3 = mercaptoacetyltriglycine; DMSA = dimercaptosuccinic acid; PRRT = peptide receptor radionuclide therapy; NET= neuroendocrine tumor; DXA = dual-energy X-ray absorptiometry; RBC = red blood cells.
Type of PET/CT scan (referrals must be reviewed by nuclear medicine consultant) Scans that can be booked and performed as requested (unless patient is at risk of COVID-19 infection) Scans that require liaison with clinical team for canceling or rescheduling (inform patient) Oncology 18F-FDG for staging, restaging, response assessment, and radiotherapy planning 18F-FDG, 68Ga-DOTATATE/DOTATOC, 18F-PSMA, 68Ga-PSMA, 18F-choline, 18F-NaF, or 18F-DOPA for follow-up evaluation 18F-PSMA, 68Ga-PSMA, or 18F-choline for biochemical recurrence 68Ga-DOTATATE/DOTATOC for staging, restaging, and selecting patients for PRRT 18F-NaF for bone metastases 18F-DOPA for diagnosis and staging Nononcology 18F-FDG for pyrexia of unknown origin in COVID-19–negative patients, for sepsis, for viability testing in symptomatic patients awaiting CABG, for suspected device or prosthetic infection, or for cardiac sarcoidosis 18F-FDG for known sarcoidosis in patients on treatment, for polymyalgia rheumatica, or for follow-up of known cardiac sarcoidosis in patients on treatment These are examples based on consensus only, and responsibility lies with each institution or hospital to ensure its written policy adheres to that outlined by national public health guidance in its respective country and hospital.
FDG = fluorodeoxyglucose; PSMA = prostate-specific membrane antigen; PRRT = peptide receptor radionuclide therapy; DOPA = 3,4-dihydroxyphenylalnine; CABG = coronary artery bypass grafting; NaF = sodium fluoride.
Therapies might be performed as scheduled. However, each patient must be assessed individually by clinical team or MDT prior to scheduling Therapy requiring cancellation or rescheduling –each patient must be assessed individually, followed by liaison with clinical team or MDT. Inform patient 177Lu-DOTATATE peptide receptor radionuclide therapy for metastatic neuroendocrine tumors (consider marrow depletion after procedure) 131I therapy for thyroid cancer (follow thyroid cancer management guide for various risk categories) Selective internal 90Y radioembolization therapy for hepatocellular carcinoma or liver metastases 131I therapy for benign thyroid disease (most treatments can be postponed; give consideration to patients who cannot tolerate antithyroid medication) 131I-metaiodobenzylguanidine therapy for metastatic pheochromocytoma or paraganglioma Radiosynovectomy for arthritis, hemophilia, and similar conditions 177Lu-prostate-specific membrane antigen therapy for metastatic prostate cancer 225Ac-prostate-specific membrane antigen therapy for metastatic prostate cancer 223Ra therapy for prostate cancer with skeletal metastases (consider comorbidities) Referrals must be reviewed by nuclear medicine consultants or in multidisciplinary setting. These are examples based on consensus only, and responsibility lies with each institution or hospital to ensure its written policy adheres to that outlined by national public health guidance in its respective country and hospital.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
- Article
- SEVERE ACUTE RESPIRATORY SYNDROME CORONAVIRUS 2
- NUCLEAR MEDICINE STAFF AND PATIENTS
- RADIONUCLIDE THERAPIES
- SOCIAL DISTANCING
- IMAGING EQUIPMENT
- RADIOPHARMACEUTICALS
- STAFF WELL-BEING
- CONTINUING MEDICAL EDUCATION AND PROFESSIONAL DEVELOPMENT
- CHEST FINDINGS FOR PET/CT AND SPECT/CT
- CONCLUSION
- DISCLOSURE
- Acknowledgments
- Footnotes
- REFERENCES
- Figures & Data
- Info & Metrics
Related Articles
Cited By...
- Recovery of cardiovascular testing in Asia during the COVID-19 pandemic: findings from the INCAPS COVID 2 study
- The Impact of the Coronavirus Disease 2019 Pandemic on the Clinical Environment
- Post-COVID-19 New Normal for Molecular Imaging Departments: A United Kingdom Perspective
- COVID-19 and Its Impact on Nuclear Medicine