


The new coronavirus pneumonia (coronavirus disease 2019 [COVID-19]) was first reported in Wuhan, China, in December 2019; the virus was extracted from lower-respiratory-tract samples from humans (1). The World Health Organization officially announced COVID-19 to be a pandemic on March 11, 2020 (2).
This novel coronavirus is spreading rapidly despite precautions. The most common symptoms of COVID-19 include severe pneumonia (fever, dry cough, dyspnea) and fatigue (1). Sore throat, headache, loss of taste and smell, rhinorrhea, and diarrhea can occur uncommonly (1). Lymphopenia is common (3,4). The mean incubation period is reported to be 5.2 d, and transmission can occur during that period in asymptomatic patients (5). The virus is reported to be transmitted via respiratory droplets and fomites during unprotected close contact with an infected individual (6,7).
Spread of the infection has been reported in 212 countries and regions (2). Throughout time, humans have encountered epidemics and pandemics, and several of these have changed the course of history. Pandemics increase morbidity and mortality and cause significant economic, political, and social disruption (8).
The aim globally is to encourage physical distancing in order to slow disease transmission and avoid increased strain on local health-care systems. The significant health-care challenges are in the production, supply, and availability of equipment for patient care and staff during this pandemic. A coordinated response and responsibility should be emphasized and implemented on time to maintain public health awareness and information, reduce transmission, and care for and treat the patients with COVID-19 (2). Significant gaps, misunderstandings, and challenges exist in global pandemic preparedness. To compound the problem further, the guidance and recommendations are rapidly changing as new evidence emerges and evolves. Local policy should be adopted in consensus with national and international recommendations. People must follow the recommendations and restrictions of the local government or health department.
Hospitals and departments should have a standard operating procedure in place for staff who image patients suspected or confirmed to have COVID-19, and systems should be in place to ensure that these procedures are regularly updated. This article is based on the currently available literature. Our purpose is to discuss and review precautions and safety measures for nuclear medicine department staff in managing patients with known or suspected COVID-19. The situation is changing rapidly, and there is every chance that discussion stemming from this article will change over the coming days and weeks. The responsibility lies with each institution or hospital to ensure its written policy adheres to that outlined by national public health guidance in its respective country.
SEVERE ACUTE RESPIRATORY SYNDROME CORONAVIRUS 2
COVID-19 is caused by a novel β-coronavirus (1) that has been given the name “severe acute respiratory syndrome coronavirus 2” (SARS-CoV-2) (2). It belongs to the Coronaviridae family and is an enveloped positive-strand RNA virus (1,9). Coronaviruses are named for the crownlike spikes on their surface (9,10). The most likely origin of the novel coronavirus is zoonotic, given it has a genome 96% identical to that of a severe acute respiratory syndrome–like coronavirus found in bats (6,11). The novel virus has been detected in respiratory, fecal, and blood specimens of infected patients (6,11) and is reported to remain viable as an aerosol for up to 3 h (12). There are reports that transmission can occur via ocular surfaces, as infected droplets and bodily fluids might contaminate the human conjunctival epithelium (13). The virus was reported to be found in upper respiratory samples 1–2 days before the onset of symptoms (14) and is thought to be spread mainly via asymptomatic carriers (5,15,16).
NUCLEAR MEDICINE STAFF AND PATIENTS
In terms of personal protective equipment (PPE), the World Health Organization recommends taking contact and droplet precautions before entering the room of a suspected or confirmed COVID-19 patient. These include wearing disposable gloves to protect the hands; a clean, nonsterile, long-sleeved gown to protect clothing; medical masks to protect the nose and mouth; and eye protection such as goggles or a face shield (17,18). Respirators (e.g., N95) are recommended for aerosol-generating procedures (17). With the increasing number of cases and the shortage of testing kits for COVID-19, there should be greater emphasis on infection-control and social-distancing measures for both the public and staff members in the health-care environment. Effective and efficient use of both staff and equipment in nuclear medicine departments is crucial for patient care and workplace safety. Several national and international bodies have reported numerous measures that might be implemented nationally and regionally (2,17–19). However, the policies and their implementation will vary from region to region. Departments should be aware of their national or local hospital policies and follow them accordingly. Numerous articles about radiology procedures on COVID-19 patients have appeared, but there is limited advice and information related to nuclear medicine services. Compared with conventional radiological imaging, the requirements and logistics for nuclear medicine imaging are relatively complex, such as scheduling appointments, contacting patients, maintaining regulatory compliance, prioritizing procedures, limiting the duration of scans, and preventing infection (Table 1) (20–25). Our top priorities should be ensuring the personal wellness of our staff and providing sufficient training and staff coverage to manage patients with suspected or confirmed COVID-19.
The team should be made aware that there are asymptomatic carriers of the virus, and a good contact history is of use. We should also ensure that, in the waiting areas, patients have access to alcohol gel, hand-washing facilities, tissue boxes, and masks. Nuclear medicine reception staff should self-protect and be vigilant at all times and encourage patients to self-declare if they or any family members have symptoms or have recently traveled from places affected by COVID-19. The staff should ask specific and direct questions such as about a history of fever, dry cough, dyspnea, and fatigue. Patients should be encouraged to follow basic hygiene practices (26). The patient waiting area should be large enough for patients to maintain distance while seated, or patient appointments should be scheduled so as to avoid having too many patients in the waiting area at a given time.
In general, the nuclear medicine staff, which includes technologists, nurses, and health-care assistants, are at risk of exposure to COVID-19. Unlike radiologic procedures, nuclear medicine procedures require radiotracer injection, and contact between the staff and patient is essential. In most cases, nuclear medicine procedures are outpatient-based; under limited circumstances, they are inpatient-based. Inpatients will be a combination of oncology and nononcology patients. There is a probability that patients with COVID-19 may be asymptomatic at the time they are in the department for their scan. Furthermore, it is possible that not all inpatients have been tested for COVID-19 before they are sent to the department for their scan. These scenarios pose a risk for all staff, from the reception area to the scanning room. In general, most nuclear medicine scanners are not portable, unlike radiography or ultrasound devices; therefore, the need for patients to come to the department for their scan is inevitable. Consequently, we should have a stringent mechanism in place to protect our staff and patients, as well as a contingency plan if staff are temporarily absent because of illness or quarantine, which might affect regular work in the department.
Under the current circumstances, most departments based in hospitals that are COVID-19 hubs are postponing routine elective scans while continuing to provide urgent nuclear medicine scans (e.g., PET/CT scans for oncology patients) (Tables 2–4). Given the widespread transmission and the increased risk of asymptomatic patients, staff should use PPE according to the local policy. The PPE items must be donned before entering the patient area, and the donning and doffing procedure should be performed correctly. In general, the team should minimize the number of staff in each clinical encounter to reduce unnecessary movement into and out of injection or scanning rooms, and staff should wear PPE while escorting patients.
Scheduling Nuclear Medicine Procedures That Use SPECT Tracers
Scheduling Nuclear Medicine Studies That Use PET/CT
Airborne transmission of COVID-19 continues to be debated. There is an ongoing dilemma on whether to do ventilation–perfusion scans. It is reported that airborne viruses can spread in air-conditioning and ventilation systems. Medical procedures associated with the generation of aerosols, such as ventilation scans and oxygen supplementation, might carry an increased risk of transmission. Therefore, some have suggested stopping ventilation–perfusion scan services because the ventilation scan is aerosol-based. In addition, the use of perfusion-only scans is unlikely to be of any benefit if COVID-19 is suspected, as the COVID-19 response might alter the macroaggregated albumin distribution (20).
Others have proposed several alternatives, such as performing only perfusion imaging in, for example, pregnant patients or performing perfusion SPECT or SPECT/CT. Overall, it depends on the local conditions. Decisions should be based on national or regional policies (22), and special precautions, especially for personnel conducting these tests, must be taken. A chest radiograph should be mandatory before a ventilation–perfusion scan. The current reports suggest that asymptomatic COVID-19 carriers may have positive chest radiography results after 14 d of quarantine, even with no reverse-transcription polymerase chain reaction testing for COVID-19 (27). The chest radiography findings in COVID-19 patients are reported to frequently show bilateral lower-zone consolidation (peaking at 10–12 d from symptom onset) (28).
RADIONUCLIDE THERAPIES
Nuclear medicine departments perform various radionuclide therapies for both benign and malignant disease. The hospital and department providing these services should have a practical and realistic solution. The multidisciplinary team (MDT) must make a pivotal decision to continue or stop therapy service temporarily. The radionuclide therapy service depends on multiple factors, such as whether the treatment is outpatient or inpatient, the availability of beds for inpatient-based treatments, regular supply and delivery of radiopharmaceuticals, the risk of a patient contracting COVID-19 during the hospital stay, the staff skill mix (in case therapy staff is infected with the virus and substitute staff must be enlisted), robust selection criteria, and treatment of elderly cancer patients with comorbidities. Finally, when patients are treated, they should additionally consent to the risk of COVID-19 during their stay in the hospital, and the need for radionuclide therapy should balance against the risk of contracting COVID-19 (Table 4).
SOCIAL DISTANCING
Physical isolation or distancing of staff from one another is crucial to prevent transmission from asymptomatic carriers. In the scan-reporting rooms, it is suggested that the workstations be separated by at least 2 m or 6 ft (23–25). First, the department should consider providing alternative technologic solutions that allow remote or off-site work for nuclear medicine consultants and residents (e.g., reporting of scans and protocolling procedures). Second, multidisciplinary meetings or case discussions should be web-based or teleconferenced (23–25). Several departments have opted for flexible rotations or schedules, such as by working in small teams or by working for 1 wk on-site and then 1 wk remotely. Establishing a group email list or a social media group to keep in touch and communicate effectively is essential.
IMAGING EQUIPMENT
Local hospitals should have clear policies and procedures in place for nuclear medicine staff who image suspected or confirmed COVID-19 patients. The standard operating procedures of the department or health-care system should be updated regularly as evidence evolves. van Doremalen et al. (12) have studied how long the virus survives in the air and on surfaces. They confirmed that the novel coronavirus remained active for 48–72 h on plastic and stainless steel surfaces, 24 h on cardboard, and 4 h on copper (12). However, these times will vary under real-world conditions and might depend on the temperature, humidity, ventilation, and amount of virus deposited (12).
The most important COVID-19 factors related to nuclear medicine include clean imaging techniques and decontamination of imaging equipment (e.g., SPECT/CT and PET/CT scanners), in addition to decontamination of any surface that may have come into contact with respiratory droplets. In general, after the patients are scanned, the scanner and room surface should be disinfected to prevent potential spread, and appropriate training of environmental maintenance staff is recommended (Fig. 1) (20). Public Health England has published guidance entitled, “COVID-19: Cleaning in Non-Healthcare Settings” (29). The risk of infection depends on several factors, such as the type of surfaces contaminated, the amount of virus shed from the individual, the time the individual spent in the setting, and the time since the individual was last in the environment (29). All surfaces that the symptomatic person might have come into contact with must be cleaned and disinfected (e.g., visible body fluids, imaging equipment, chair, bathrooms, door handles, telephones, and grab-rails in corridors and stairwells) (29). The PPE should be worn for cleaning an area where a person with possible or confirmed COVID-19 has been (29). Public Health England recommends the use of a combined detergent disinfectant solution at a dilution of 1,000 parts per million available chlorine; if an alternative disinfectant is used within the organization, this alternative should be checked to ensure that it is effective against enveloped viruses (29).
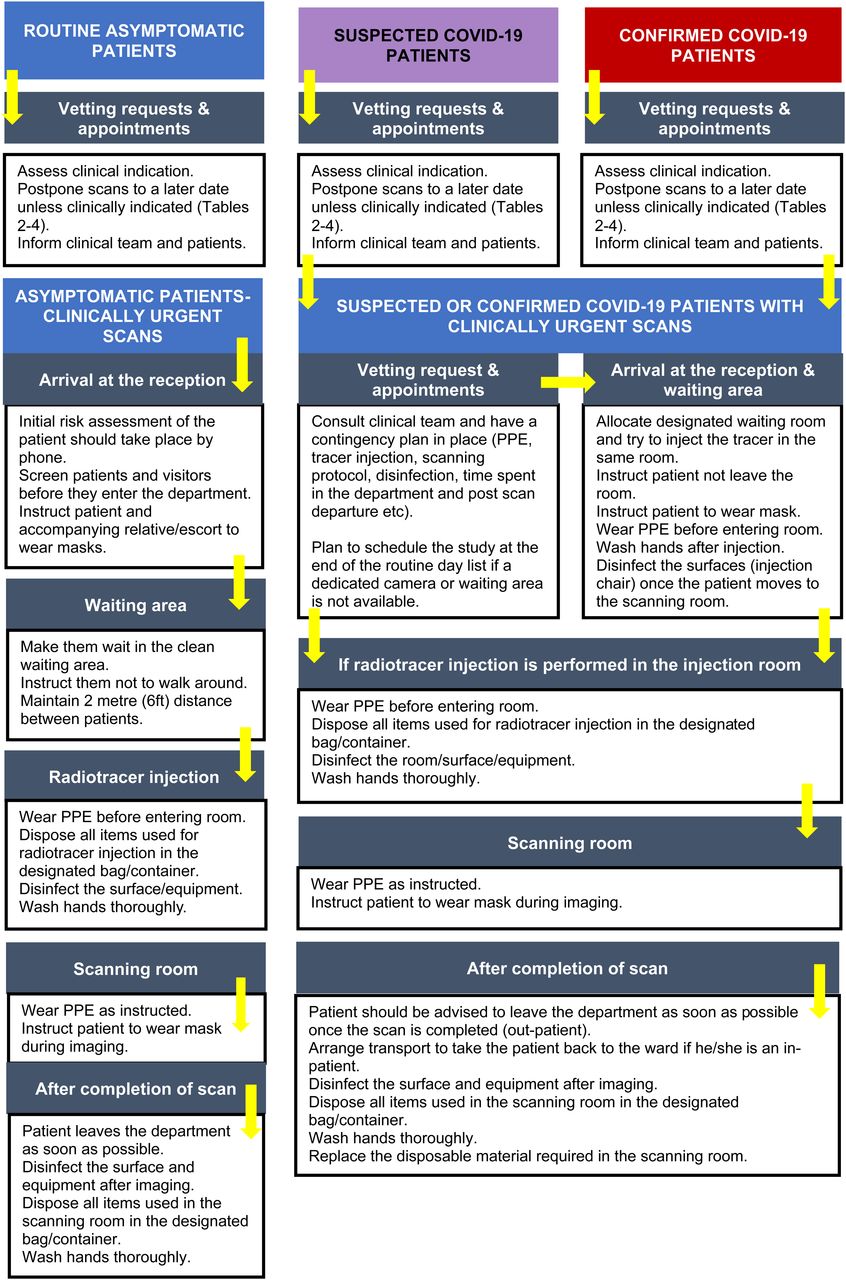
Basic contingency for nuclear medicine imaging. (Adapted from (41).)
The British Society of Thoracic Imaging has produced action cards to assist with designing local radiology standard operating procedures for patients who have or are at risk of COVID-19 (e.g., transferring a patient to a CT scanner or performing a CT scan) (30). These action cards might be applied to nuclear medicine departments as well. However, they are examples only, and the responsibility lies with each institution or hospital to ensure that its written policy adheres to the national public health guidance in the respective country.
RADIOPHARMACEUTICALS
The functioning of nuclear medicine procedures depends on the availability of radioisotopes and kits. These are not always locally produced; nuclear medicine centers might have to rely on obtaining them from national or international supply-and-distribution channels. In the current scenario, with land and air traffic lockdowns, a shortage of radioisotopes and kits is expected, and it is difficult to predict when the shortage will occur or for how long. For efficient use of kits, block booking of specific procedures should be envisaged. Alternately, PET/CT scans can be used in place of single-isotope methods for some indications (e.g., bone imaging with 18F-NaF and infection imaging with 18F-FDG). Myocardial perfusion imaging can be performed as a 1-d protocol (stress–rest). Local radiopharmacists or managers of nuclear medicine departments should contact the suppliers and update the local team so that bookings can be planned accordingly. In comparison to SPECT services, PET centers with local cyclotrons might continue to function as usual in most cases. For departments without cyclotrons, the availability of 18F-FDG will depend on local conditions.
STAFF WELL-BEING
The current scenario might cause psychologic distress, social insecurity, and financial insecurity. Staff coming to work at the hospital are concerned that they might contract the virus and expose their friends or family. We should try to provide relevant and reliable information to allay their fears (e.g., social distancing, infection control, and self-quarantine). There should be specific local guidelines for viral testing of staff returning to work after illness. The team should remain connected with one another or with their friends and families by such means as group email, e-portals, and social media.
CONTINUING MEDICAL EDUCATION AND PROFESSIONAL DEVELOPMENT
Departments that are active in teaching and training can use online teaching material and webinars, which are available from most national and international nuclear medicine societies, as an alternative to face-to-face interaction and learning. National organizations should make some of their online education material available free to its members. Research work will be challenging during the current circumstances (except for research related to COVID-19), as most institutions have suspended their projects, and alternative ways of collaborating should be envisaged to prevent disruption of vital projects (23,25).
CHEST FINDINGS FOR PET/CT AND SPECT/CT
Incidental parenchymal lung abnormalities on chest images have been reported for patients with COVID-19, and prompt recognition may be useful for timely isolation and treatment (Figs. 2–5) (1). The chest radiographic and CT appearance of COVID-19 has been reported to overlap significantly with the findings for other types of coronavirus infections (31–33).

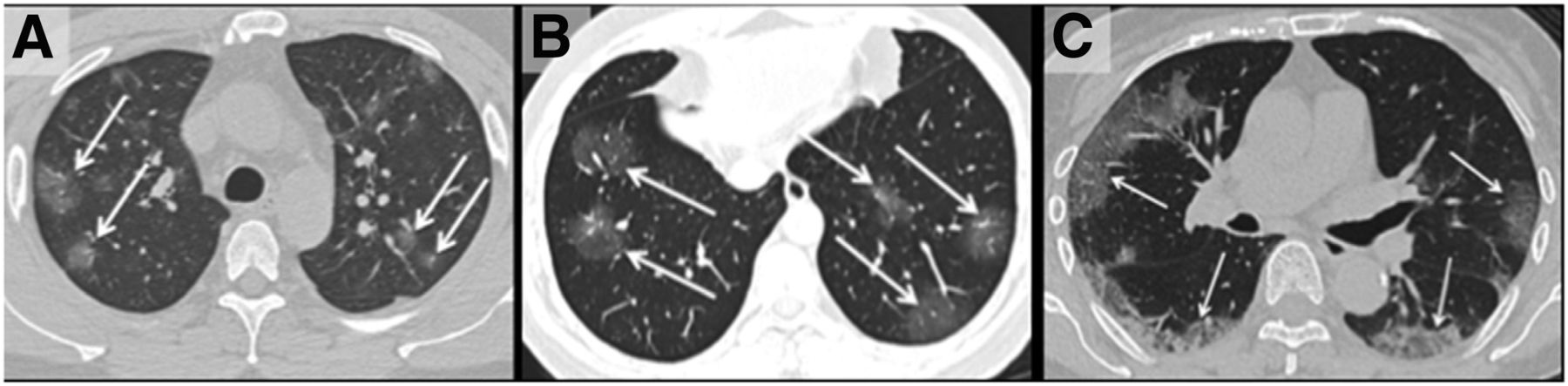
(A) Unenhanced axial CT image from 36‐year‐old man shows bilateral ground‐glass opacities in upper lobes with rounded morphology (arrows). (B) Axial CT image from 44‐year‐old man shows larger ground-glass opacities bilaterally in lower lobes with rounded morphology (arrows). (C) Axial CT image from 65‐year‐old woman shows bilateral ground‐glass and consolidative opacities with striking peripheral distribution. (Reprinted with permission of (32).)
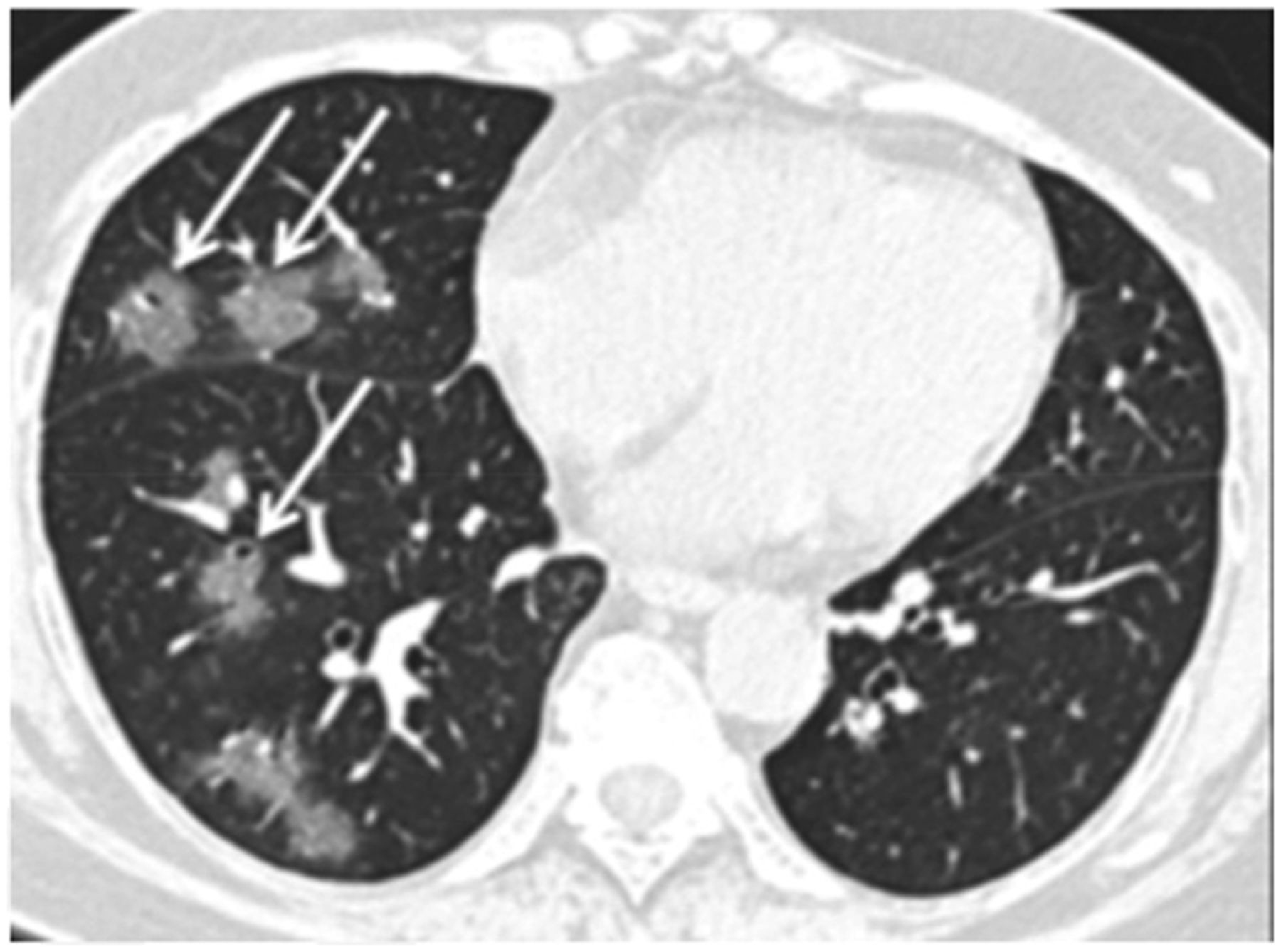
Unenhanced axial CT image from 56‐year‐old woman shows ground‐glass opacities with rounded morphology (arrows) in right middle and lower lobes. Left lung was normal. (Reprinted with permission of (32).)

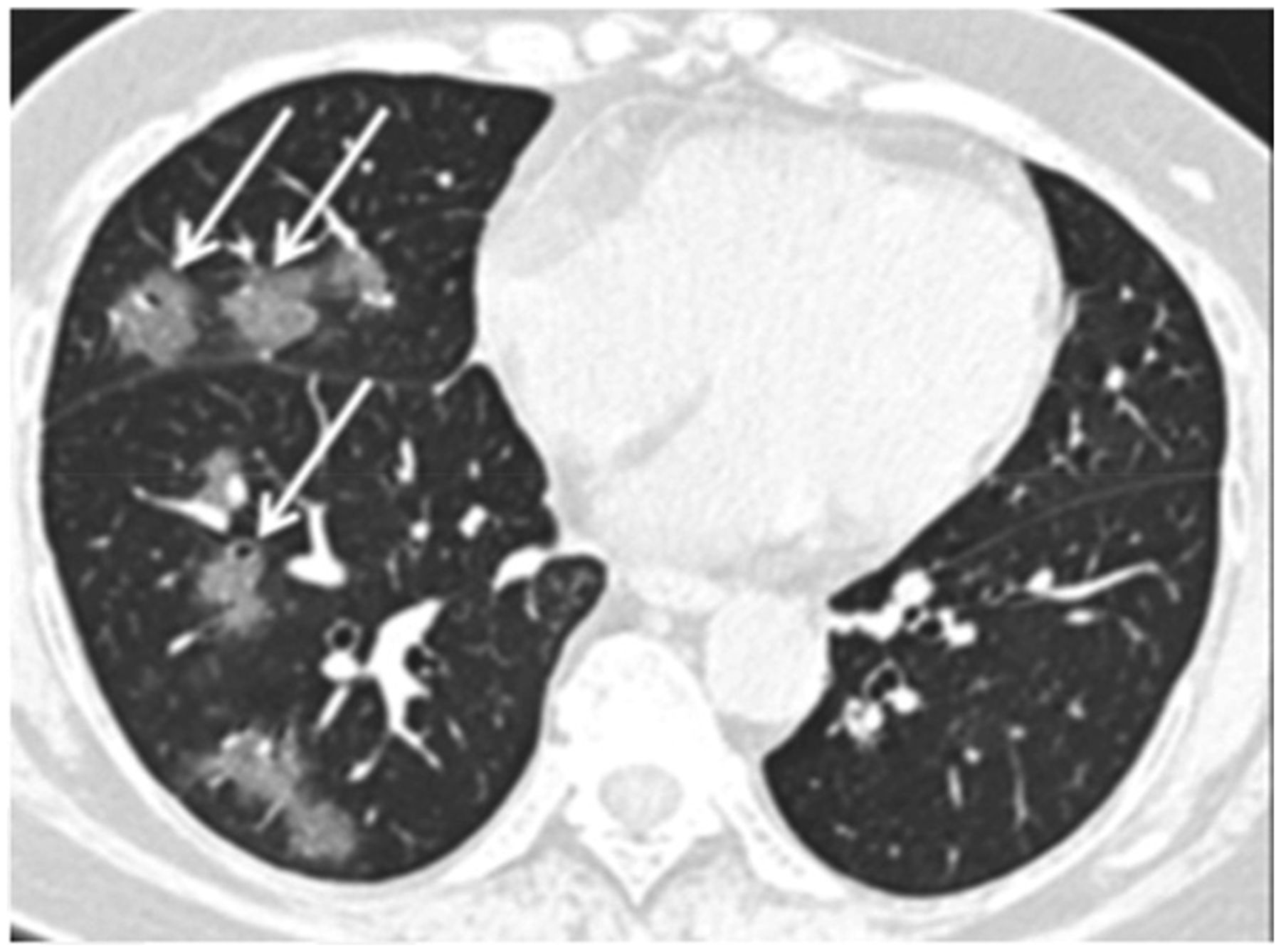
Unenhanced axial CT image from 42‐year‐old man in late time group (10 d from symptom onset to this scan) shows bilateral consolidative opacities with striking peripheral distribution in right lower lobe (solid arrows) and with rounded morphology in left lower lobe (dashed arrow). (Reprinted with permission of (32).)
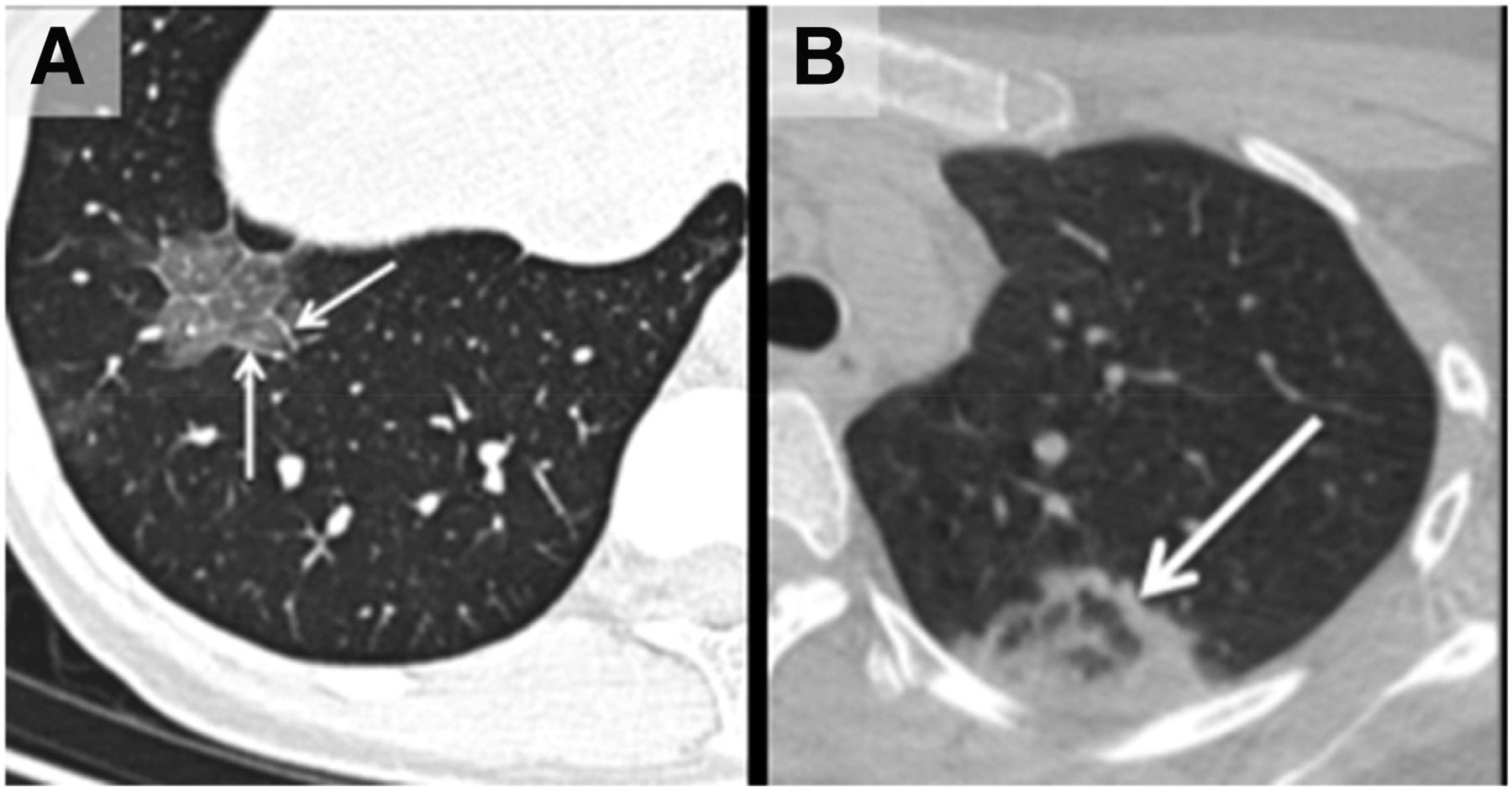
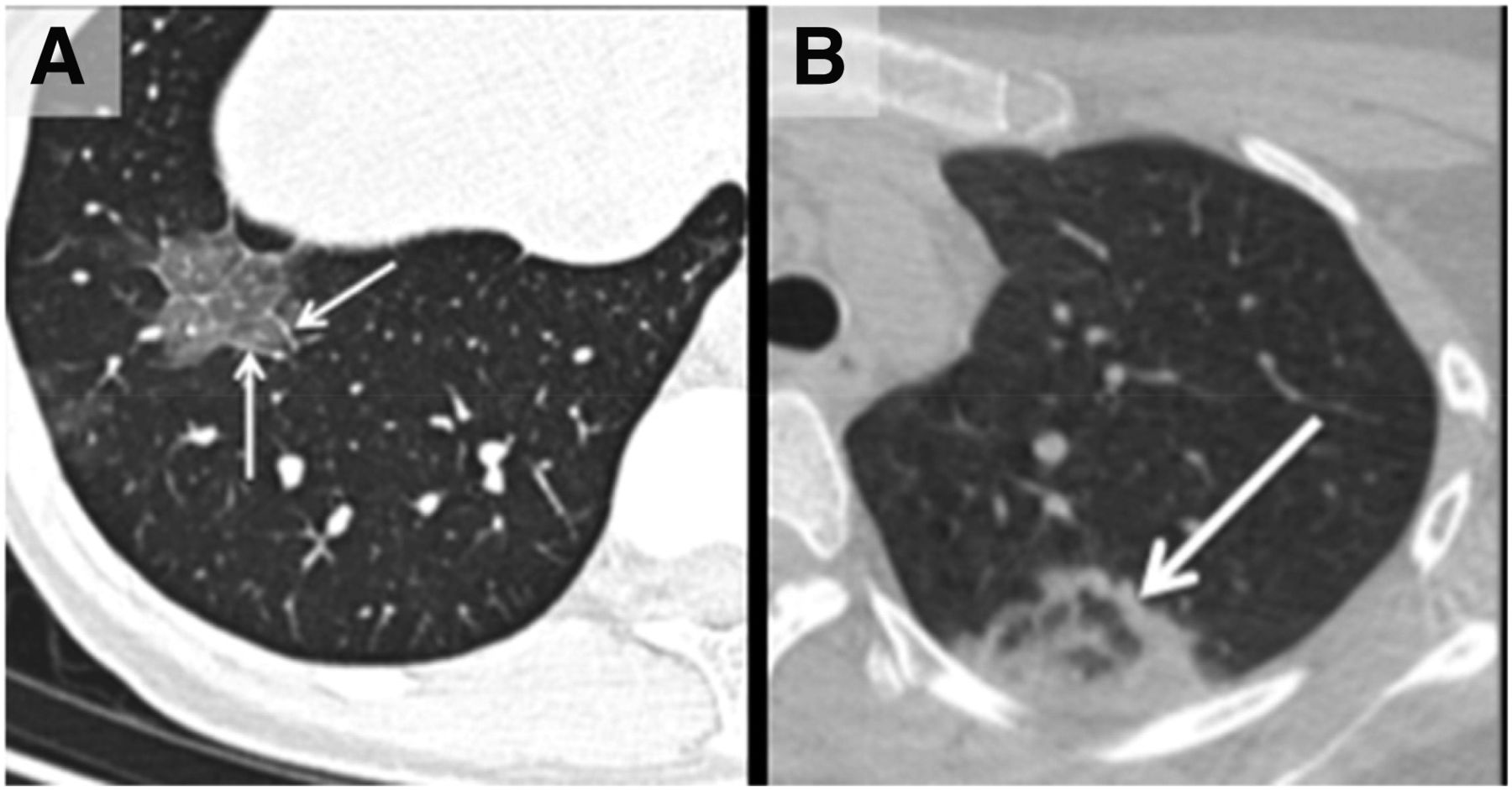
(A) Unenhanced axial CT image from 43-y-old woman shows crazy‐paving pattern as manifested by right-lower-lobe ground‐glass opacification with interlobular septal thickening (arrows) and intralobular lines. (B) Axial CT image from 22‐year-old woman shows area of faint ground‐glass opacification in left upper lobe, with ring of denser consolidation (arrow, reverse halo sign). (Reprinted with permission of (32).)
Chest CT is reported to be an essential component in the diagnostic algorithm for patients with suspected COVID-19 (32,33). The reported sensitivity of chest CT in detecting COVID-19 at the initial presentation is 56%–98% during the early stages of disease development (34,35), and the specificity is low (25%) (36).
Chest CT has limited sensitivity and a low negative predictive value early after symptom onset and is unlikely to be used as a reliable independent tool to rule out COVID-19 (32).
The initial findings in infected patients from Wuhan have shown bilateral lung opacities. The typical features include lobular and subsegmental areas of consolidation (31,32). Other groups have reported high rates of ground-glass opacities and consolidation, sometimes with a rounded morphology and peripheral lung distribution (31,37). The more extensive disease is reported to be seen on CT approximately 10 d after the onset of symptoms (37).
The frequency of CT findings is related to the infection time course (31,32). On the basis of the current evidence, there are ground-glass abnormalities in the early disease phase, followed by crazy paving and increasing consolidation later in the disease course (32,37).
Multifocal involvement is reported to be common, and the CT signs gradually improve approximately 14 d after symptom onset (31,32,36,37).
The hallmark of COVID-19 on CT is ground-glass opacities and consolidation or pulmonary opacities (often with a bilateral and peripheral lung distribution) (31,32). Bernheim et al. have reported the absence of ancillary CT findings such as pleural effusions, lung cavitation, pulmonary nodules, and lymphadenopathy (31,32). Bai et al. have assessed the performance of U.S. and Chinese radiologists in differentiating COVID-19 from viral pneumonia on chest CT and found high specificity but moderate sensitivity (38). The British Society of Thoracic Imaging has published reporting guidance and a proforma document (which might help to report findings with speed and accuracy) (39), as well as a teaching library. Its content will be accessible without a log-on via the British Society of Thoracic Imaging website (39). COVID-19–suspected pneumonia is 18F-FDG–avid and might be detected as an incidental finding in asymptomatic patients undergoing PET/CT (40). The nuclear medicine community should be vigilant about looking for other unexpected scan findings that might reflect the effects of COVID-19 exposure or infection.
CONCLUSION
COVID-19 has changed the way we work. We should stay informed, support each other, and provide practical solutions for safety and social well-being during these uncertain times. We should adhere to our national and international recommendations. The health-care system and professionals must aim to deliver safe patient care, maintain a safe workplace, and ensure personal wellness.Life imposes things on you that you can’t control, but you still have the choice of how you’re going to live through this.
—Celine Dion
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank all medical and nuclear medicine professionals worldwide for their dedication and commitment to publishing numerous documents and sharing their experience to fight COVID-19.
Footnotes
Published online Apr. 20, 2020.
Immediate Open Access: Creative Commons Attribution 4.0 International License (CC BY) allows users to share and adapt with attribution, excluding materials credited to previous publications. License: https://creativecommons.org/licenses/by/4.0/. Details: http://jnm.snmjournals.org/site/misc/permission.xhtml.
REFERENCES
- Received for publication April 13, 2020.
- Accepted for publication April 16, 2020.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
- Article
- SEVERE ACUTE RESPIRATORY SYNDROME CORONAVIRUS 2
- NUCLEAR MEDICINE STAFF AND PATIENTS
- RADIONUCLIDE THERAPIES
- SOCIAL DISTANCING
- IMAGING EQUIPMENT
- RADIOPHARMACEUTICALS
- STAFF WELL-BEING
- CONTINUING MEDICAL EDUCATION AND PROFESSIONAL DEVELOPMENT
- CHEST FINDINGS FOR PET/CT AND SPECT/CT
- CONCLUSION
- DISCLOSURE
- Acknowledgments
- Footnotes
- REFERENCES
- Figures & Data
- Info & Metrics
Related Articles
Cited By...
- Recovery of cardiovascular testing in Asia during the COVID-19 pandemic: findings from the INCAPS COVID 2 study
- The Impact of the Coronavirus Disease 2019 Pandemic on the Clinical Environment
- Post-COVID-19 New Normal for Molecular Imaging Departments: A United Kingdom Perspective
- COVID-19 and Its Impact on Nuclear Medicine