


Abstract
We report a rare case of incidental diffuse hot liver on 99mTc-macroaggregated albumin lung perfusion scanning done to exclude pulmonary embolism. This scintigraphic finding suggested synchronous obstruction of the superior and inferior venae cavae, later confirmed on CT angiography. Although many cases of focal hepatic uptake have been reported, reports of diffuse uptake because of vena cava obstruction are scarce in the literature.
- lung perfusion scintigraphy
- diffuse hepatic uptake
- synchronous SVC and IVC obstruction
- portosystemic shunt
Extrapulmonary accumulation of 99mTc-macroaggregated albumin is uncommon in lung perfusion scans. In the absence of interfering hemodynamic disease, 95% of 99mTc-macroaggregated albumin particles localize in the lungs during the first pass through the pulmonary capillaries because of capillary blockade. In right-to-left or portosystemic shunts, 99mTc-macroaggregated albumin particles enter the systemic circulation and cause capillary blockade in highly perfused organs, visualized as increased organ uptake.
CASE REPORT
A 22-y-old woman with a history of end-stage renal disease on peritoneal dialysis, paraplegia, and recurrent deep vein thrombosis was referred for lung scintigraphy because of tachypnea and desaturation.
A 99mTc-macroaggregated albumin lung scan (Fig. 1) acquired after intravenous injection of 111 MBq (3 mCi) of radiotracer showed diffuse hepatic uptake suggesting that most of the 99mTc-macroaggregated albumin had passed into the liver, initiating suspicion of vena cava obstruction. Both lungs showed only minimal uptake even with a longer scan time to increase the count density. A follow-up CT scan showed obstruction of the superior and inferior venae cavae (Figs. 2A and 2B), with extensive venous collaterals (Fig. 3). The second-pass phase of the CT scan showed passage of contrast to the pulmonary vasculature through a patent suprahepatic inferior vena cava (Fig. 4), explaining the minimal activity in the lungs on prolonged scintigraphic imaging.

Planar scintigraphic images including chest and abdomen in anterior and posterior projections show diffuse hepatic uptake (oblique arrows). Minimal uptake is seen bilaterally in lungs (horizontal arrows).

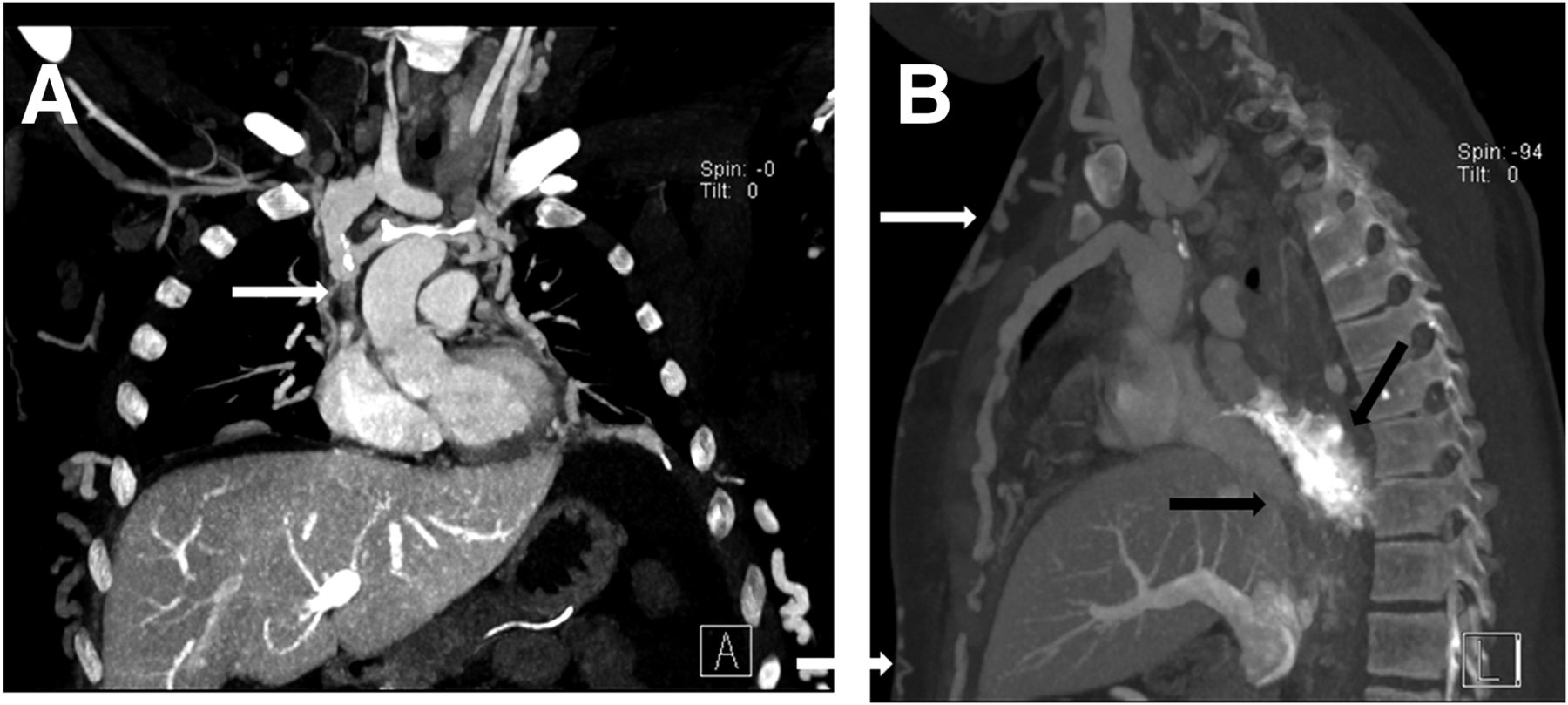
Contrast-enhanced CT scan of thorax and upper abdomen. (A) Coronal reformat shows superior vena cava obstruction (arrow). (B) Sagittal reformat shows inferior vena cava obstruction (horizontal black arrow) posterosuperior to liver. Bulk of tortuous collateral veins (oblique black arrow) drains toward left atrium, and multiple subcutaneous collaterals can be seen (white arrows)
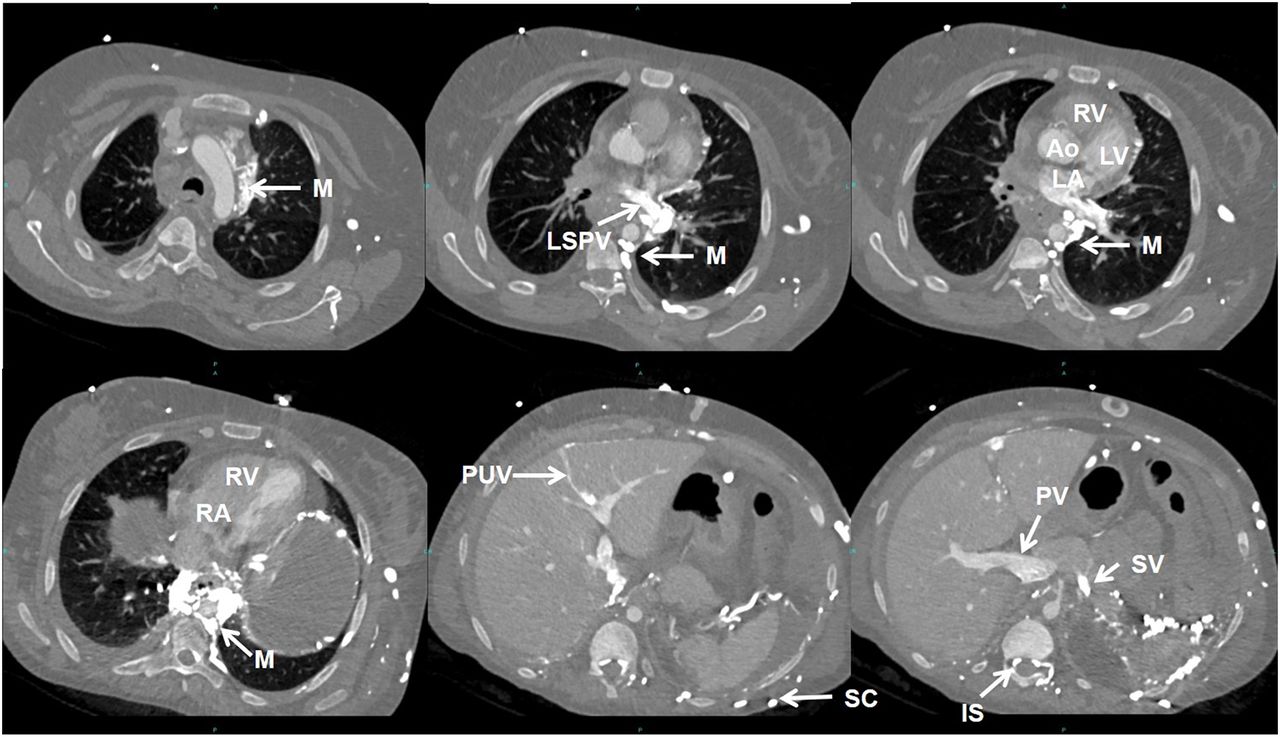
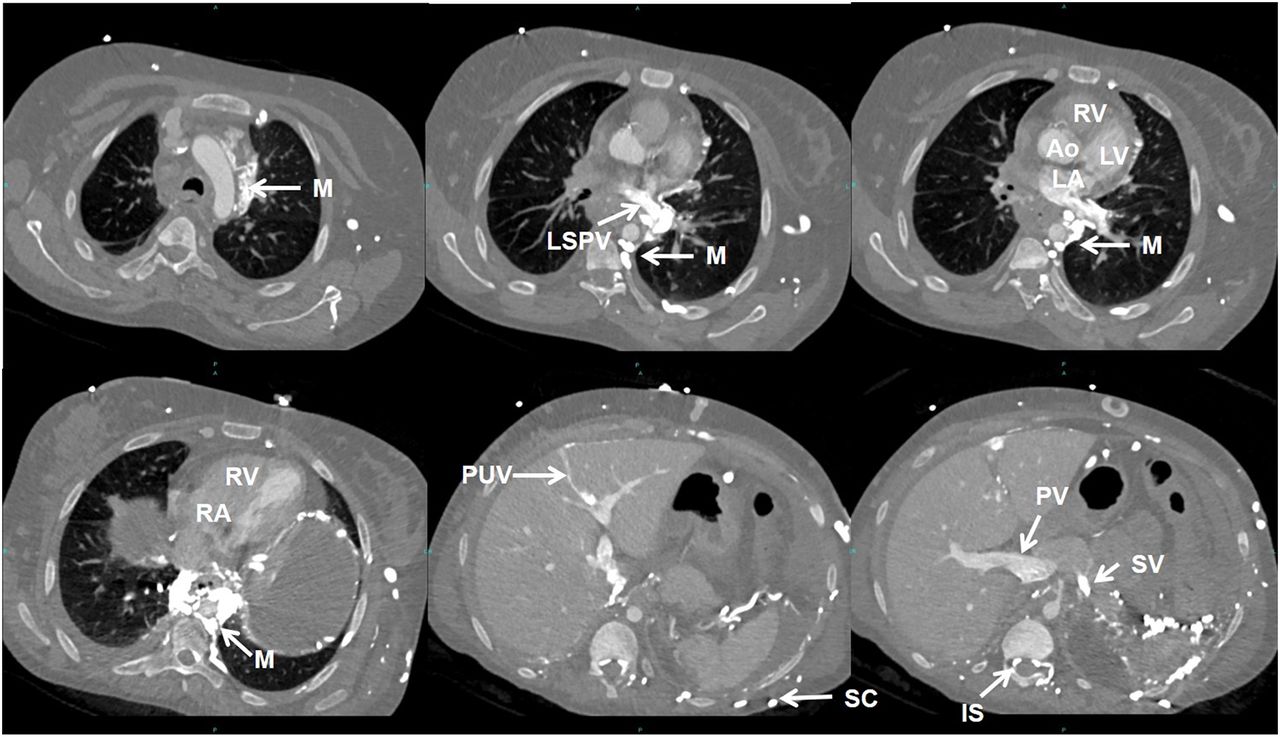
Axial images of first-pass contrast-enhanced CT scan of thorax show passage of contrast agent (injected in left arm vein) through dilated and tortuous collateral mediastinal (M), subcutaneous (SC), and intraspinal (IS) veins into left atrium (LA), left ventricle (LV), and aorta (Ao) via left superior pulmonary vein (LSPV), before reaching right atrium (RA) and right ventricle (RV). Systemic–portal collateral pathways carry contrast agent into portal vein (PV) through splenic vein (SV) and recanalized paraumbilical vein (PUV).
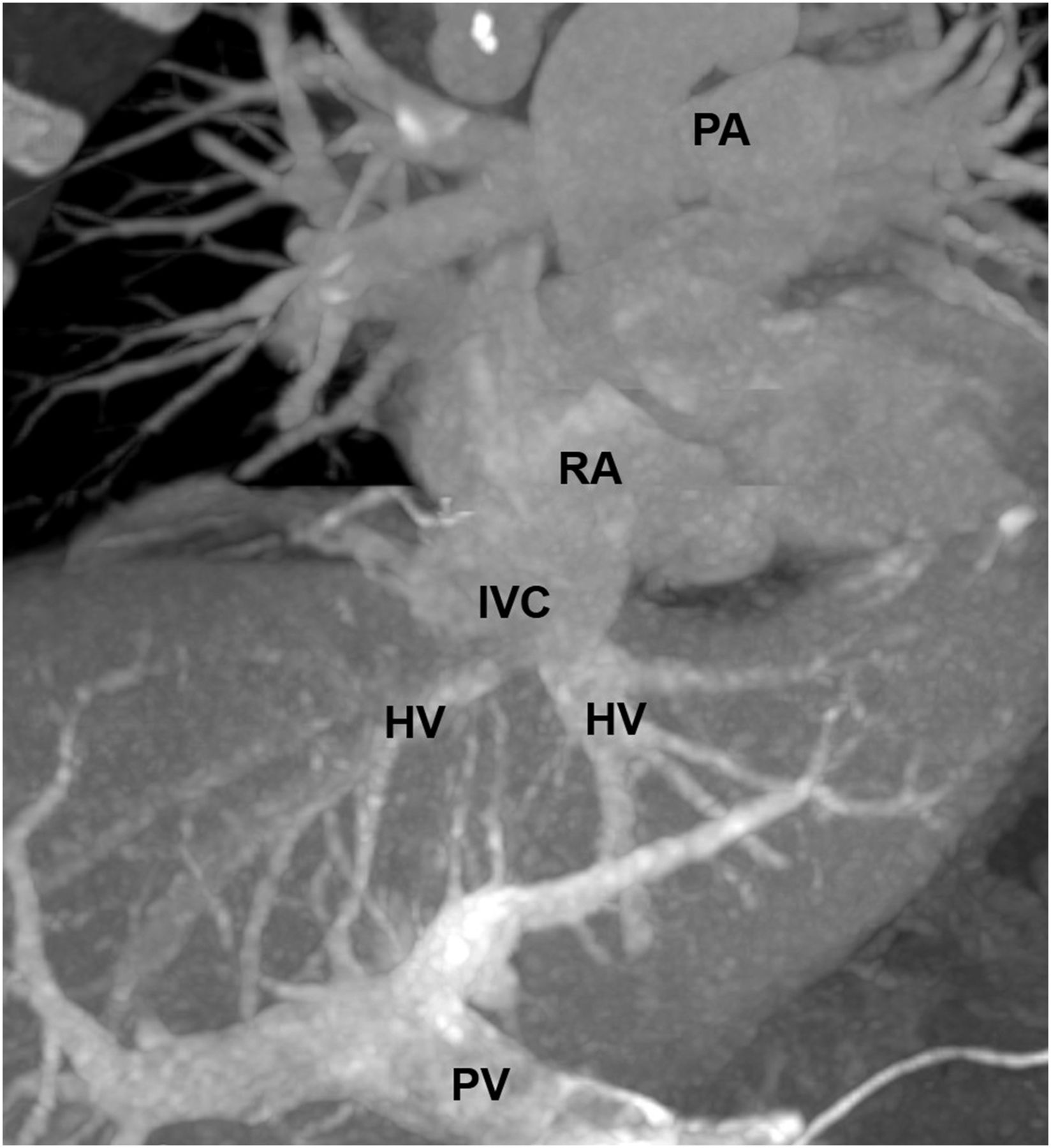
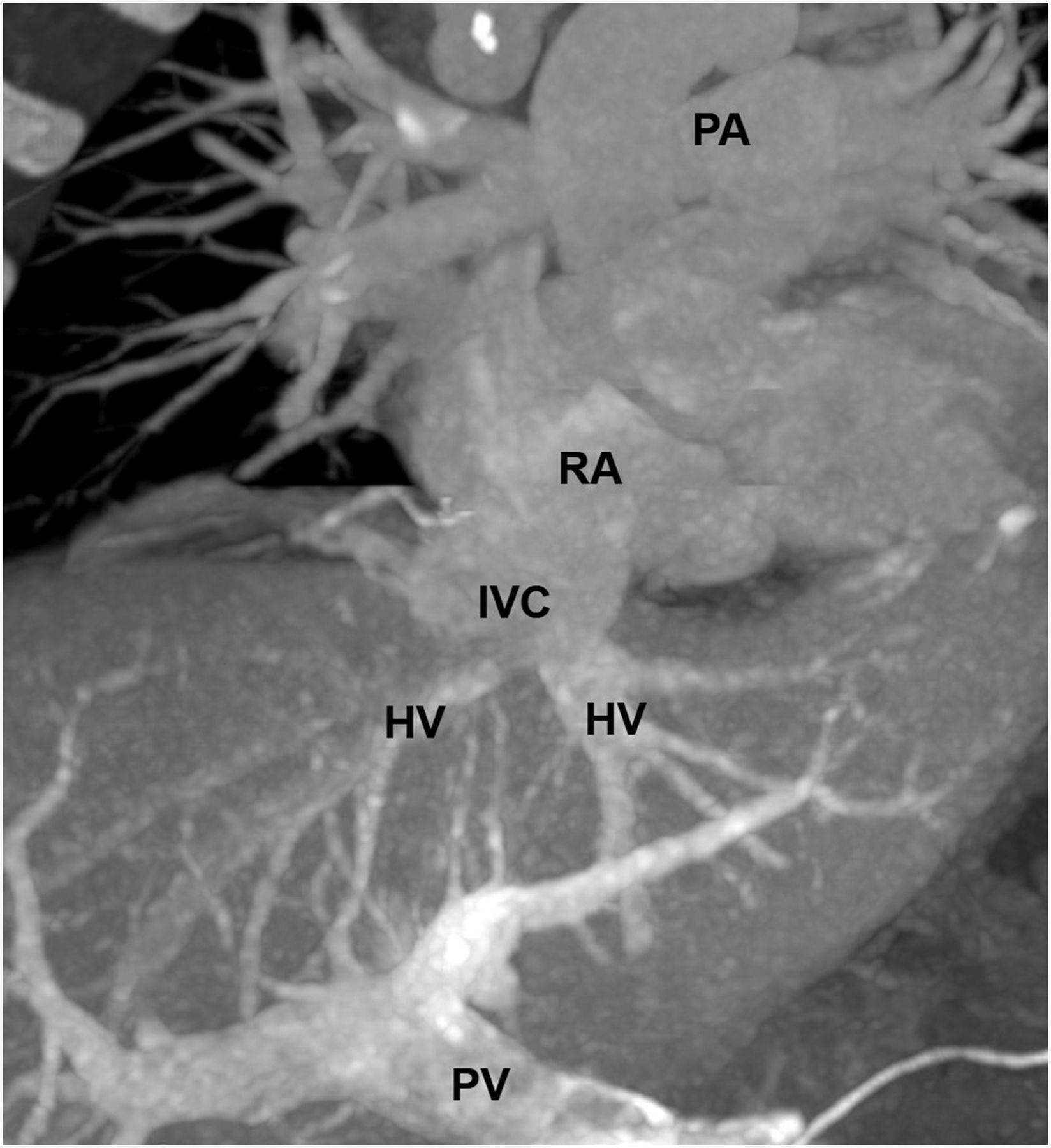
Coronal maximum-intensity projection from second-pass phase of contrast-enhanced CT scan shows passage of contrast agent via portal vein (PV), liver sinusoids, and hepatic veins (HV) into patent suprahepatic part of inferior vena cava (IVC) and right atrium (RA) to reach main pulmonary artery (PA) and pulmonary vasculature.
DISCUSSION
Once the quality check of the radiopharmaceutical is sorted out, extrapulmonary radioactivity on 99mTc-macroaggregated albumin lung scans suggests a right-to-left or portosystemic shunt, depending on the organs visualized (1). Shunting of systemic venous blood to the portal system causes hepatic radiotracer accumulation (2). In cases of chronic obstruction of the superior or inferior vena cava, venous drainage is maintained by collateral pathways (3), and on the basis of this anatomy, abnormal liver uptake is demonstrated. Causes for superior vena cava obstruction include malignancy, thrombus, mediastinal fibrosis, and venous catheterization (4). Superior extension of lower limb or pelvic deep vein thrombosis is a major reason for inferior vena cava obstruction (5).
CONCLUSION
Diffuse liver uptake on 99mTc-macroaggregated albumin lung scintigraphy should not be overlooked. In our case, the finding led to initial suspicion of critical synchronous obstruction of the superior and inferior venae cavae, leading to further investigations and a definitive diagnosis.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Jun. 10, 2019.
REFERENCES
- Received for publication May 3, 2019.
- Accepted for publication May 23, 2019.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.