


Abstract
131I-metaiodobenzylguanidine (131I-MIBG) is a theranostic agent useful for treatment of neuroendocrine malignancies. In this case, a child with a Curie score of 21 was administered 17.871 GBq (483 mCi) of 131I-MIBG. The elimination half-life progressively increased from 23 h to 77 h during the 11 d that the patient was hospitalized for radiation isolation. Six weeks after the posttherapy scan, a survey with an ion-chamber device yielded readings of 0.3 μSv/h (0.03 mR/h) on contact with spinal regions that had shown increased uptake on the scan. A planar image obtained using the 131I setting and a high-energy collimator did not demonstrate any focal uptake. 123I-MIBG was administered, and the 24-h scan was of diagnostic quality, without degradation from the remaining 131I-MIBG. Additional study is needed on whether the Curie score affects elimination of 131I-MIBG and on whether the period of hospitalized radiation isolation needs to be extended.
We report a case of progressively delayed excretion of 131I-MIBG, while in hospitalized radiation isolation. Elimination of the agent became progressively decreased over time. Upon discharge from hospitalized radiation isolation, the posttherapy scan showed retention of 131I-MIBG throughout much of the skeleton. We questioned whether any remaining 131I-MIBG after therapy interfered with the 123I-MIBG diagnostic scan.
CASE REPORT
Neuroblastoma patients who may not qualify for other 131I-metaiodobenzylguanidine (MIBG) protocols may qualify for the Jubilant DraxImage, Inc., expanded-access protocol (IND 76,227), as was the case for this patient. Treatment of the patient in this case report was approved by the Cook Children’s Medical Center Institutional Review Board, and the child’s legal guardian gave written informed consent.
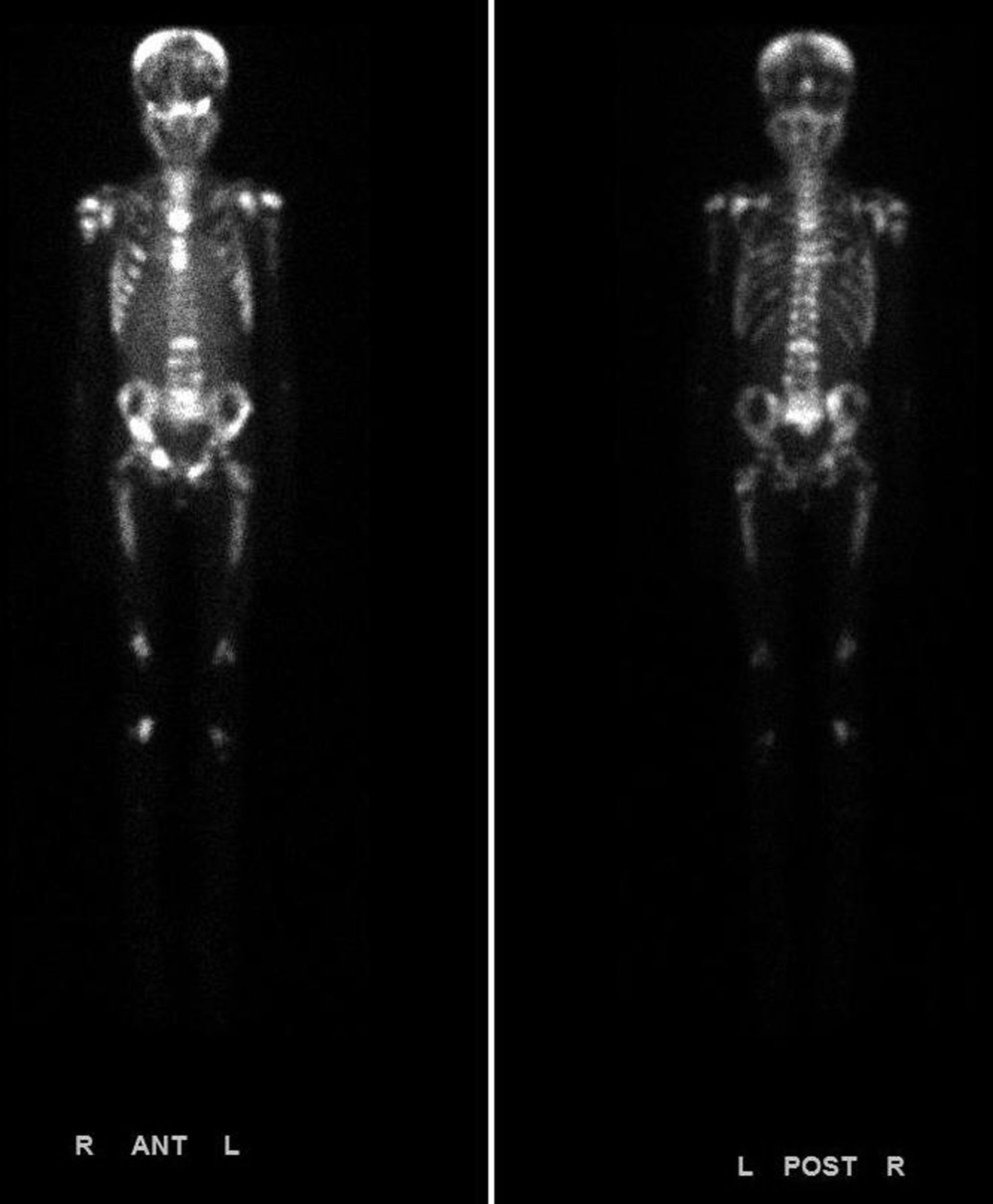
A 12-y-old girl with metastatic neuroblastoma and a Curie score of 21 underwent systemic therapy with 131I-MIBG at a dose of 666 MBq/kg (18 mCi/kg). In our experience, when 17.871 GBq (483 mCi) of 131I-MIBG is administered intravenously, approximately 90% is eliminated through urinary excretion during the first 96 h (Fig. 1), and the elimination half-life of the agent progressively increases while the patient is hospitalized for radiation isolation. The first half-life excretion time was approximately 23 h, the second 86 h, the third 148 h, and the fourth 225 h (Fig. 2). The posttherapy scan (Fig. 3) confirmed retention of 131I-MIBG throughout the axial skeleton, pelvis, and lower extremities.
Normal elimination curve with 14,948 MBq (404 mCi) of 131I-MIBG.

Delayed elimination curve with 17,908 MBq (484 mCi) of 131I-MIBG.

Posttherapy 131I-MIBG scan at 11 d.
Approximately 6 wk after receiving the therapy, the patient was scheduled for a diagnostic 123I-MIBG scan, as is usual practice. We could not find any reports in the literature on either dose rate readings or imaging performed on a patient after such a prolonged retention of 131I-MIBG. There was uncertainty as to whether, to achieve a diagnostic-quality scan, we would need to administer additional 123I-MIBG activity to overcome any scatter from the remaining 131I-MIBG. On arrival at the nuclear medicine department for the diagnostic scan, the patient was surveyed with a Ludlum 9DP-1 low-pressure ion chamber survey meter pressurized to 1.36 atm (20 psi), with a 0- to 5-Sv (0–500 R/h) dose range. Radiation exposure readings at that time were 0.3 μSv (0.03 mR/h) at 1 m over the umbilicus and 1.0 μSv/h (0.1 mR/h) on contact with the umbilicus. A similar survey performed over the areas of the spine that had shown increased uptake on the 131I-MIBG posttherapy scan yielded measurements of no more than 0.4 μSv (0.04 mR/h) on contact. A planar scan with a GE Healthcare Optima 640 SPECT/CT γ-camera using the 131I setting and a high-energy collimator at the equivalent scan speed of 30 cm/min was performed before administration of the 123I-MIBG imaging dose. This scan showed increased background activity but no focal uptake (Fig. 4). The decision was made to proceed with administration of the planned activity of 259 MBq (7 mCi) of 123I-MIBG. A scan on the next day using the same γ-camera with a medium-energy collimator and an equivalent scan speed of 6.6 cm/min yielded a diagnostic-quality image (Fig. 5).

Posttherapy 131I-MIBG scan at 6 wk.

Posttherapy 24-h 123I-MIBG scan at 6 wk.
DISCUSSION
Neuroblastoma accounts for about 6% of all cancers in children, with about 700 new cases diagnosed each year in the United States (1). The theranostic agent 131I, when bound to MIBG, has proven useful against neuroblastoma and other neuroendocrine tumors (2), with response rates of as high as 50% for relapsed disease (3). The pharmacokinetics fits a 3-compartment model, with approximately 50% of the 131I-MIBG being excreted in the urine during the first 24 h, 90% being excreted within 96 h, and the maximum biologic half-life being about 5 d (4). In our experience, we have not had patients with a biologic half-life excretion of more than about 2 d.
Treatment-study parameters specify that kidney function must meet one of the following two criteria: a serum creatinine level of no more than 2 times the upper limit of normal, or a 24-h creatinine clearance or glomerular filtration rate of at least 60 mL/min/1.73 m2. This patient’s kidney function at the time of therapy was reflected by a blood urea nitrogen level of 7 mg/dL (range of normal, 6–20 mg/dL) and a creatinine level of 114 mg/dL (range of normal, 60–115 mg/dL). Furthermore, the patient was not taking any medications known to interfere with MIBG excretion. To maintain optimal hydration and urinary excretion, we gave the patient supplemental intravenous normal saline at a rate of 125 mL/h while she was hospitalized for radiation isolation. Therefore, retention of the radiopharmaceutical due to poor kidney function was unlikely.
Elimination half-life measurements were derived from continuous readings with an over-the-bed Ludlum 9DP-1 survey meter. The survey meter was affixed to the bed so as to be kept at a constant distance of about 1 m from the patient regardless of bed height. Maintaining a constant distance between the patient and the survey meter reduces changes in instrument response due to the proximity of the radioactive patient and inverse-square-law effects (5). Measurements were logged onto a USB memory chip once every minute for the duration of the isolation period. These measurements are useful for calculating the radiopharmaceutical excretion rate and deriving the whole-body radiation dose to the patient (6). Periodic dose-rate measurements also help with decision making on when to release the patient from radiation isolation in the hospital and on how long the patient should be additionally confined at home.
Diagnostic imaging with 123I-MIBG for neuroblastoma is widely accepted as the optimal study to determine disease stage and suitability for therapy with 131I-MIBG (7). The semiquantitative Curie score from 123I-MIBG diagnostic scans standardizes the measurement of [disease stage and] response to therapy and has proven useful in predicting long-term outcome (8). A correlation between whole-body radiation dose and administered activity is expected, but a correlation does not appear to exist between a [low or high] Curie score and reduced burden of osteomedullary metastases (9). By extension, one would expect that patients with higher Curie scores would have slower excretion of 131I-MIBG, but a literature search found no evidence for such a correlation.
CONCLUSION
There was much retention of 131I-MIBG in this case. The activity appeared to be released more quickly from skeletal tumors than from the liver. Nevertheless, the normal activity remaining in the liver did not seem to degrade the quality of the 123I-MIBG diagnostic scan. This case shows that more data are needed from patients with various Curie scores to determine whether there is a correlation between Curie score and the retention time of 131I-MIBG.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Oct. 11, 2019.
REFERENCES
- Received for publication May 10, 2019.
- Accepted for publication July 26, 2019.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.