


Abstract
Neuroendocrine tumors (NETs) of the skin or soft tissue are rare (mostly described as sites of metastasis), whereas primary soft-tissue NETs are extremely rare; they are usually diagnosed at advanced stages with distant metastases because of their indolent nature. We herein describe our experience with 2 such cases. In the first case, the NET originated in the retroperitoneal soft tissue, and in the second case, the patient was a middle-aged lady with NET arising from soft tissue in the pelvis. Both patients were treated with 177Lu-DOTATATE in view of their somatostatin receptor–expressing metastatic lesions, demonstrating an excellent outcome as reflected by a complete metabolic response and near-complete anatomic response to the administered peptide receptor radionuclide therapy. The noteworthy factors of the reported cases were, first, unusual sites of primary tumor and, second, near-complete to complete symptomatic, anatomic, and metabolic resolution of the recurrent primary tumor and metastatic lesions with peptide receptor radionuclide therapy alone. NETs arising from rare anatomic locations are usually nonfunctioning, with good clinical outcomes, and 177Lu-DOTATATE peptide receptor radionuclide therapy can be considered promising in patients with metastatic or advanced disease.
- 177Lu-DOTATATE
- neuroendocrine tumor
- peptide receptor radionuclide therapy
- primary soft tissue neuroendocrine tumor
Neuroendocrine tumors are rare heterogeneous tumors with an incidence ranging from 1 to 5 per 100,000 patients (1) and arise from the neural crest cells (Kulchitsky cells), enterochromaffin cells, and enterochromaffinlike cells, having both neural and endocrine components. They were first known as carcinoid tumors, but the term has been replaced by neuroendocrine tumor (NET) in the World Health Organization and European Neuroendocrine Tumor Society classification (2). Malignancy is not infrequent, and most cases of malignancy are diagnosed at advanced stages with distant metastases because of its indolent nature. The most common sites are gastroenteropancreatic (73.7%) and tracheobronchopulmonary (25.1%). Other sites, which are seldom affected, include the parathyroid, adrenal, and pituitary glands and the calcitonin-producing C-cells of the thyroid, and sites that are still less common are the skin and soft tissues (3,4). NETs in the skin and soft tissues are almost always metastatic from primary NETs in the more commonly involved organs (5,6). Primary cutaneous and soft-tissue NETs arising de novo are extremely rare and have not been described in the published literature, except for the well-documented Merkel cell carcinoma of the skin (7–9). Published accounts of primary soft-tissue NETs are sparse and comprise only a few case studies (10–13). This report presents our experience with 2 such cases of primary soft-tissue NETs and their favorable outcome with peptide receptor radionuclide therapy (PRRT). Both patients had metastatic NETs, demonstrated a Krenning score of 3 for uptake on 68Ga-DOTATATE PET/CT, were being considered for PRRT after discussion by a multidisciplinary team, and were to receive the therapy after providing written informed consent.
CASE I
A 42-y-old woman with no comorbidities presented in June 2017 with abdominal pain, vomiting, and an increased frequency of loose stools. Her baseline hematologic examination, renal function, liver function, serum electrolytes, and electrocardiograph were all within normal limits. On further evaluation, CT of the abdomen and pelvis revealed multiple retroperitoneal nodes, irregular peritoneal thickening, cholelithiasis without active cholecystitis, a sclerotic lesion at the junction of the body of the T12 vertebra, and a pedicle on the right side of the T12 vertebra. She underwent open cholecystectomy, along with diagnostic laparotomy and biopsy of the suspected abdominal nodes, in June 2017. Histopathologic examination of the nodes revealed a well-differentiated NET (World Health Organization grade II, 2010), with the immunohistochemistry panel showing chromogranin and synaptophysin positivity, along with the epithelial markers AE1 and AE3 and an MIB-1 index (proliferative index) of 8%. These results were further correlated with an increased level of serum chromogranin A, a tumor marker (2,910 ng/mL; reference value, <98.1 ng/mL).
On the basis of the clinical profile, the results of laboratory evaluations, and the imaging and histopathologic evidence, a diagnosis of a grade II (intermediate-grade) NET of retroperitoneal soft-tissue mass was made, with lymph nodal and solitary skeletal metastases. The patient was evaluated accordingly with molecular imaging and referred for PRRT at our center in August 2017.
Whole-body 68Ga-DOTATATE PET/CT revealed high-grade somatostatin receptor (SSTR) expression in the omental thickening, with multiple serosal and peritoneal deposits on the surface of the liver, pelvic organs, and bowel loops. Multiple enlarged, SSTR-expressing pelvic, retroperitoneal, epiphrenic, internal mammary, mediastinal, supraclavicular, and a few tiny mesenteric nodes were seen bilaterally. There were also SSTR-expressing right pleural deposits and areas of pleural thickening, together with an SSTR-expressing T12 lesion at the junction of the vertebral body and pedicle on the right side. A small hypodense lesion was seen in the segment II of liver with no tracer uptake. 18F-FDG PET/CT of the whole body revealed moderate- to high-grade metabolism in all above-mentioned lesions except the subcarinal and right supraclavicular nodes. The segment II liver lesion did not reveal any hypermetabolism.
Renal functional scans as a part of the pretherapy work-up were done with 99mTc-labeled diethylenetriaminepentaacetic acid and ethylene dicysteine and were within normal limits. The patient underwent a first cycle of PRRT with 177Lu-DOTATATE in August 2017 using a standard renoprotective protocol. She tolerated the therapy well and was discharged the next morning, with posttherapy scans showing uptake similar to the 68Ga-DOTATATE PET/CT scan findings.
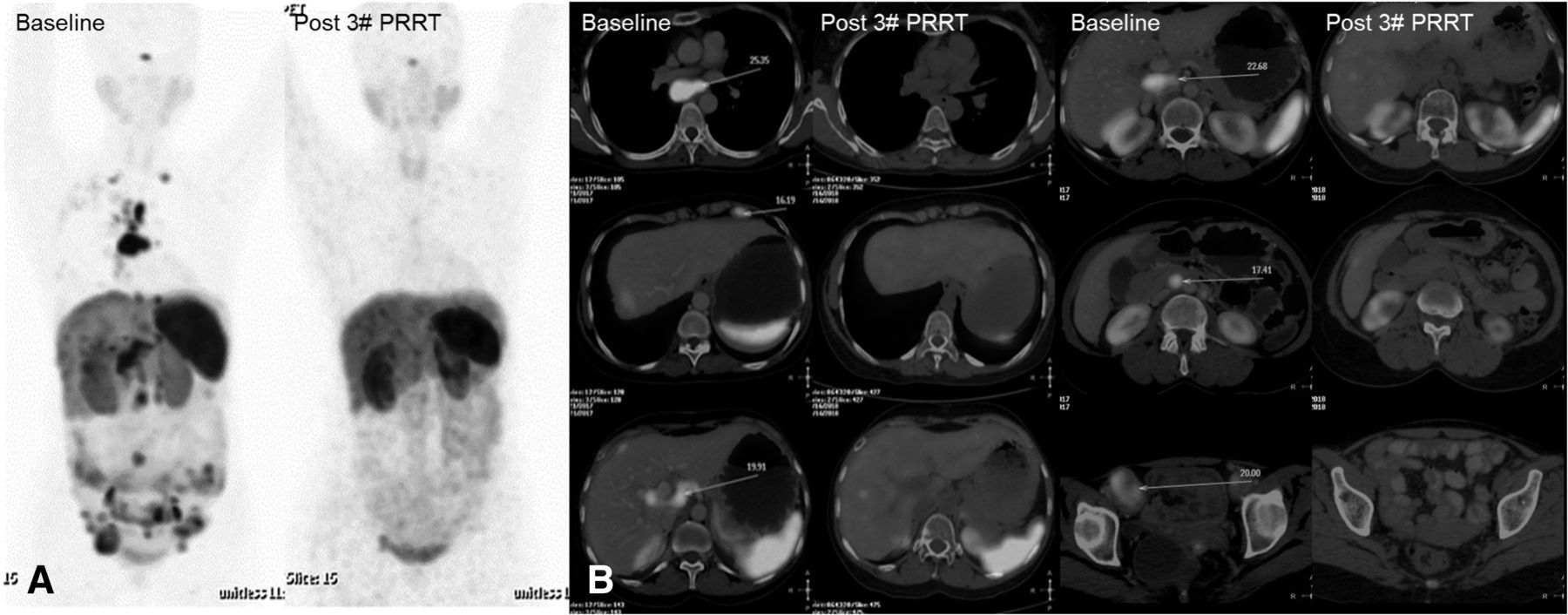
Similarly, she underwent 2 more cycles of PRRT at an interval of 3–4 mo, with a cumulative activity of approximately 22,200 MBq (600 mCi) after the third PRRT in June 2018. She reported in October 2018 for her fourth-cycle work-up and showed complete symptomatic resolution. The 68Ga-DOTATATE PET/CT at this time showed physiologic tracer distribution with no abnormal tracer uptake (Fig. 1). Contrast-enhanced CT revealed complete anatomic resolution of the omental and serosal deposits and of the mediastinal, retroperitoneal, and pelvic lymph nodes; a small, unchanged mildly enhancing solitary lesion in segment II of liver; and a small sclerotic focus at the junction of the T12 body and pedicle on the right side of the vertebra. The mesentery, omentum, and bowel loops were normal.

(A) Maximum-intensity-projection 68Ga-DOTATATE PET/CT scans at baseline and after 3 cycles of PRRT showing complete metabolic resolution of uptake. (B) Transaxial 68Ga-DOTATATE PET/CT scans at baseline and after 3 cycles of PRRT showing complete metabolic and anatomic resolution of lesions.
The findings suggested complete anatomic and metabolic resolution. Hence, no further PRRT was administered, and it was decided to follow up the patient biannually.
CASE II
A 50-y-old woman with a history of total abdominal hysterectomy and bilateral salpingo-oophorectomy for a large uterine fibroid presented with pain in the perianal region and right lower leg for a 2-y duration. The findings on systemic examination were essentially normal, with no organomegaly or free fluid on abdominal palpation. Rectal examination revealed a hard, nodular, and fixed mass felt through the right lateral rectal wall, with intact mucosa, 4 cm from the anal verge. Physical inspection of other body parts revealed no significant abnormalities. Contrast-enhanced MRI of the pelvis revealed an enhancing mass measuring approximately 6 × 5.5 × 4 cm in the right pararectal space, with pelvic side-wall infiltration and a small locoregional node, inseparable from the lateral aspect of the lower rectum on the right side. CT of the thorax and abdomen was also done in an effort to diagnose the primary site, but the thoracic and abdominal cavities and the contained viscera were unremarkable. An ultrasonography-guided Tru-Cut (Merit Medical) biopsy of the lesion revealed NET, grade II. An exploratory laparotomy revealed within the right pelvis a 5 × 5 cm fixed mass involving the lateral pelvic wall and infiltrating the sacrum and, hence, deemed inoperable. Follow-up contrast-enhanced MRI revealed a 6 × 3 cm enhancing mass with irregular borders in the right side of pelvis. Fat planes within the rectum, ipsilateral pyriformis, ipsilateral sacrum, right internal iliac vessels, sciatic nerve, and sacrococcygeal nerves were either inconspicuous or lost. There was obvious infiltration of the ipsilateral levator ani and the obturator internus. The patient underwent surgery again, by a combined multispecialty team, who performed exploratory laparotomy. Perioperative findings revealed an approximately 5 × 4 cm hard, irregular growth lying in the presacral plane in front of S2, S3, and S4 to the right of the midline, closely abutting the lower rectum, vaginal stump, and urinary bladder. The S2 nerve was found traversing the tumor and was removed en bloc. Wide excision was undertaken, with removal of the pyriformis muscle, sacrospinous ligament, and periosteum. Rectal wall injury was found and repaired, and a diversion ileostomy was made. In December 2015, the ileostomy was closed with a side-to-side approach using staples.
In early 2017, the patient presented with pain in the right pelvic region, and the mass was found to have recurred at the surgical site. Contrast-enhanced CT revealed a 9 × 7 × 6 cm soft-tissue mass in the right pelvis adjacent to the urinary bladder. The mass was infiltrating the pelvic wall muscles and sacrum posteriorly, with resultant widening of the S2 neural foramina and extension of soft tissue through it. There was evidence of metastatic lesions in the liver (segments VI and VII of the right lobe), the lesser sac above the pancreas, and multiple bilateral lung nodules. An SSTR-imaging PET/CT scan revealed SSTR expression in the pelvic presacral soft-tissue mass and lung nodules. No abnormal SSTR expression was seen in the hepatic lesions or the lesser sac deposits. The baseline serum chromogranin A level was 86.8 ng/mL, and 24-h urinary 5-hydroxyindoleacetic acid was 2.56 mg.
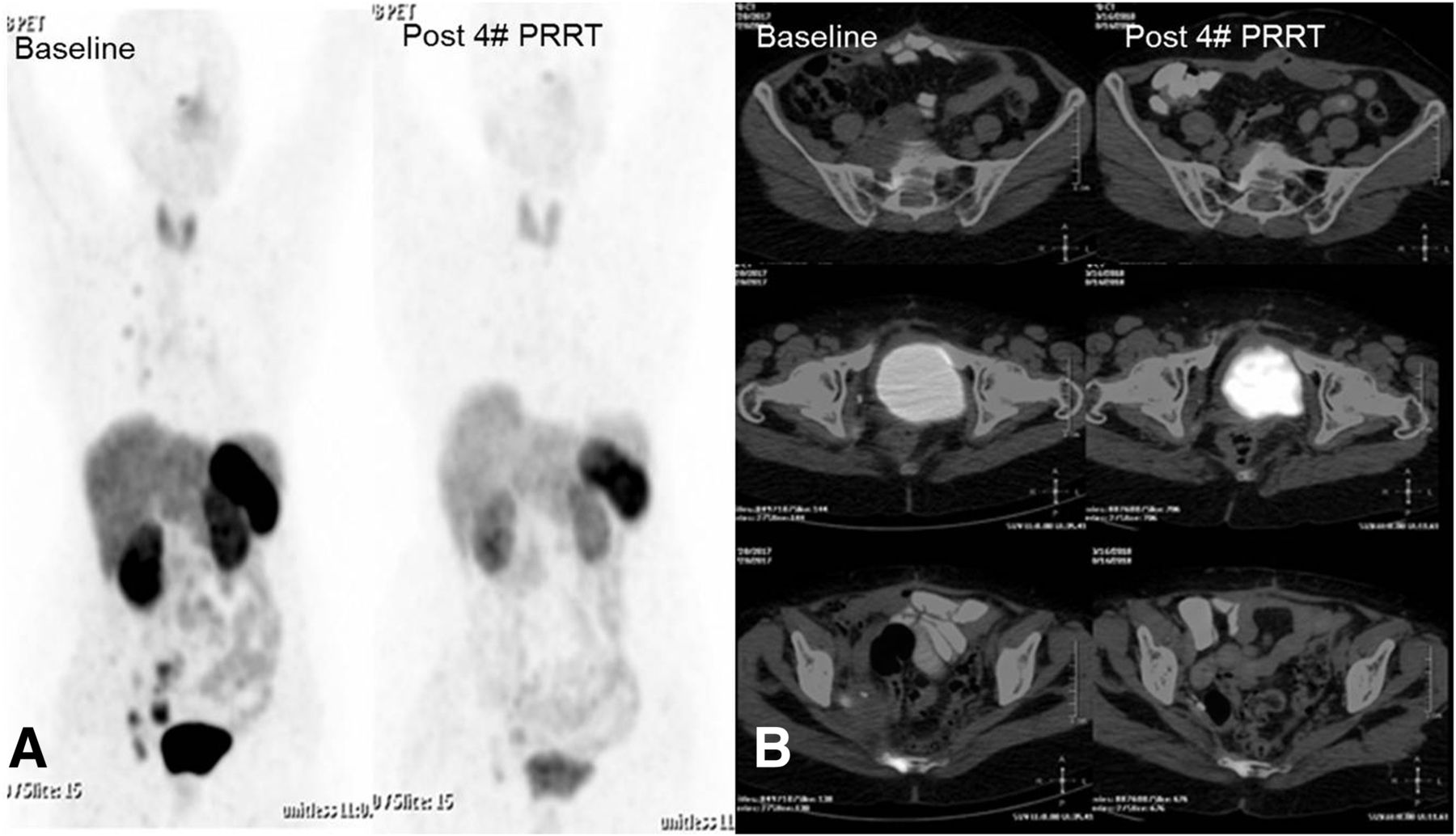
In view of the findings, the patient was referred to our department for PRRT. She underwent 4 cycles of PRRT with 177Lu-DOTATATE between May 2017 and December 2018, with a cumulative activity of approximately 25,900 MBq (700 mCi) according to the standard renoprotective protocol, as in the first case. Follow-up 68Ga-DOTATATE and whole-body 18F-FDG PET/CT revealed a progressive decrease in the size and metabolic activity of the tumor, with normal tumor marker levels: serum chromogranin A was 54.9 ng/mL and 24-h urinary 5-hydroxyindoleacetic acid was 2.52 mg. Follow-up scans after 4 cycles of PRRT, in October 2018, showed complete anatomic and metabolic resolution of the right pelvic soft-tissue mass and the lung nodules. Although a subcentimeter-sized right internal iliac node with minimal SSTR expression was persisting, it showed a significant decrease in size; also, mild uptake was seen in the sacrococcygeal region, but no abnormal soft-tissue mass was noted (Fig. 2). None of the lesions showed abnormally increased 18F-FDG uptake, suggesting no abnormal metabolic activity and hence a favorable prognosis.
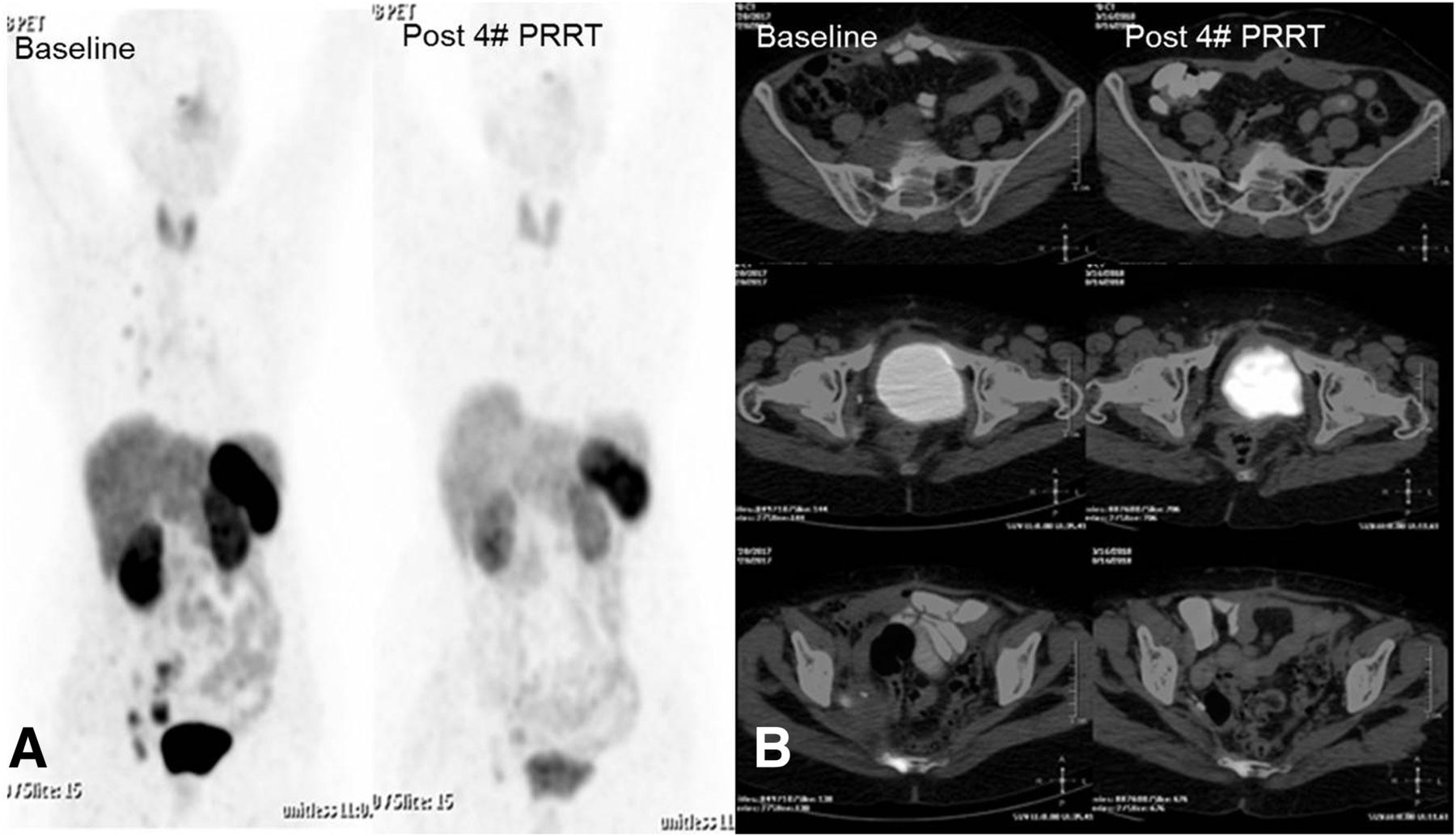
(A) Maximum-intensity-projection 68Ga-DOTATATE PET/CT scans at baseline and after 4 cycles of PRRT showing near-complete metabolic resolution of uptake. (B) Transaxial 68Ga-DOTATATE PET/CT scans at baseline and after 4 cycles of PRRT showing near-complete metabolic and anatomic resolution of lesions.
In view of the favorable outcome reflected by the complete metabolic response and the near-complete anatomic response, further PRRT was withheld and the patients was scheduled for biannual follow-up.
DISCUSSION
NETs are rare tumors and are classified according to their various attributes, namely embryologic origin into foregut, midgut, and hindgut derivatives; functional and nonfunctional tumors, depending on the synthesis and release of biologically active amines and peptides; grades I, II, and III, depending on the proliferation index and mitotic figures; and NETs or neuroendocrine carcinoma.
The differential diagnosis of the soft-tissue tumors in our patients included metastatic deposits from a primary in the gastrointestinal tract, malignant transformation of nerve-sheath tumors, and a spindle cell neoplasm. A metastatic origin was nearly ruled out in view of the negative results on imaging and other clinicopathologic examinations, which failed to find any substantial evidence of a second primary tumor. Hence, a diagnosis of primary soft-tissue NET was made. The incidence of primary soft-tissue NETs is extremely low, and most of the soft-tissue involvement in NETs comprises metastases from a more common primary site in the gastrointestinal tract or lungs. To date, only 8 publications have reported a soft-tissue primary NET. In most of these, the primary tumor was in the breast, thigh, or axilla (11–18). In this regard, the peculiarity of our cases lay in their unusual locations; that is, retroperitoneal soft tissue in the first case and pelvic soft tissue in the second case.
Diagnosing NETs can be challenging at times because of their widespread location, small size, and indolent nature. Functional tumors are diagnosed earlier than nonfunctional ones. Transabdominal ultrasonography, endoscopic examination of the gastrointestinal tract and tracheobronchial tree, and MRI, along with SSTR- and glucose transporter receptor–based PET imaging fused with CT or MRI, have been widely used to diagnose the small and inconspicuous lesions with increasing confidence. The primary tumor highlighted by these modalities is then amenable to tissue diagnosis and immunohistochemistry, thus increasing the sensitivity, specificity, and yield (19–23). Treatment and follow-up strategies are then devised on the basis of metastatic involvement and the proliferation index or grade of the tumor. Both of our cases were grade II tumors and hence carried a better prognosis than grade III tumors or neuroendocrine carcinoma (8).
The treatment of choice in a case of NET is surgical excision (24), but surgery often is not possible because of widespread metastases, vascular encasement, or a high risk of morbidity and mortality because of preexisting diseases or conditions. In patients for whom surgery cannot be undertaken, there are a battery of therapeutic options, including chemotherapy (with mammalian target of rapamycin inhibitors, platinum-based compounds, and capecitabine, among others), interferon-α, somatostatin analogs, localized radiotherapy, ablation therapy, and PRRT (25,26). Recently, PRRT targeting the SSTRs has gained popularity because of a good symptomatic response, a favorable toxicity profile, and convenient administration as 3 monthly cycles.
The noteworthy factors of our cases are the unusual site of the primary tumor, involving the retroperitoneal and pelvic soft tissue (to our knowledge, this has not previously been reported in the literature), and the near-complete to complete symptomatic, anatomic, and metabolic resolution of the primary tumor and metastatic lesions with PRRT alone.
CONCLUSION
Primary soft-tissue NETs are an extremely rare entity, and surgical resection is potentially curative. However, adjuvant therapy with PRRT targeting the SSTRs is effective and a safe adjunct to surgery or, in cases of metastatic disease, for use on an unresectable primary tumor or a patient not deemed fit for surgery. In patients with a favorable tumor histopathology (with low to intermediate proliferation and mitotic profile), PRRT can produce gratifying tumor regression even in the presence of extensive metastasis.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Aug. 10, 2019.
REFERENCES
- Received for publication January 31, 2019.
- Accepted for publication June 3, 2019.





{kind=link}
{kind=link}