


Abstract
Cost containment through indigenous production of radioimmunotherapy agents for non-Hodgkin lymphoma (NHL) would be a pivotal step toward wider clinical availability, especially in developing countries. We examined the biodistribution and dosimetry of indigenously developed and radiolabeled 131I-rituximab, using the monoclonal antibody of chimeric origin, in patients with B-cell lymphoma for potential use in radioimmunotherapy. Methods: This prospective study included 13 patients with B-cell NHL who underwent low-dose diagnostic scanning for dosimetric and biodistribution studies. Soon after rituximab infusion, a diagnostic dose of radioiodinated rituximab was administered. Serial planar whole-body γ-camera images were taken soon afterward and on days 1, 2, 4, and 6. A source of 131I with known activity was used as a reference standard for dosimetry calculations. Results: The patient-specific administered dose that would give a whole-body absorbed radiation dose of 75 cGy, calculated by the MIRD schema, ranged from 3,095.42 to 6,330.33 MBq (83.66–171.09 mCi), with a mean of 3,986.01 ± 863.95 MBq (107.73 ± 23.35 mCi) and a median of 3,697.41 MBq (99.93 mCi). The mean residence time was 69.54 h. Within the first 48 h at least 50% of the injected activity was cleared, and by 144 h at least 80% was cleared. The patient-specific administered dose that would give a whole-body absorbed radiation dose of 75 cGy, calculated by mean residence time and activity-hours, ranged from 2,654.75 to 6,210.45 MBq (71.75–167.85 mCi), with a mean of 3,576.42 ± 927.59 MBq (96.66 ± 25.07 mCi) and a median of 3,421.02 MBq (92.46 mCi). With respect to organ-specific dosimetry, the mean absorbed doses to organs (apart from blood pool [3.77 Gy] and spleen [4.02 Gy]) were 0.97 Gy to the lungs, 0.69 Gy to the liver, and 0.7 Gy to the kidneys. Conclusion: The indigenous product had kinetics similar to commercial radiopharmaceuticals, with the advantage of a lower human antimouse antibody response because of the pharmaceutical’s being a chimeric antibody rather than a murine antibody. Hence, clinical administration was safe. In none of the organs did dose-limiting radiation exposure occur at the proposed therapeutic dose.
Malignancy of lymphoid cells ranges from indolent to highly aggressive forms (1). Thomas Hodgkin, for whom Hodgkin lymphoma is named, published the first description of lymphoma in 1832 (2). Lymphoma is one of the most common hematologic malignancies worldwide, with an estimated 74,680 new cases diagnosed in the United States in 2017 and 2018 (3–5). It comprises 3%–4% of all malignancies and is ranked as the seventh most common cancer overall (6,7) and the third most common in children (8), and its incidence is higher in developed countries than in developing countries (6). These cancers arise from the immune system at different stages of differentiation, causing a wide range of morphologic, immunologic, and clinical findings (1). Once the diagnosis is established, there are several treatment options: chemotherapy with cyclophosphamide, doxorubicin, vincristine, and prednisone (most commonly); combination chemotherapy–immunotherapy with rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone; radiation; and hematopoietic stem cell transplantation. Despite the multitude of chemotherapeutic options available for recurrence, none has had a significant impact on survival, with low cost effectiveness and poor safety profiles (9,10).
More recently, radioimmunotherapy, which uses a monoclonal antibody in addition to a radionuclide to deliver radiation to the sites of disease, has been extensively studied with encouraging results (9,11). Radioimmunotherapy combines the benefits of immunotherapy and radioisotopes and has been shown to be effective for non-Hodgkin lymphoma (NHL), both in relapsed or refractory cases and in newly diagnosed cases. Although initial success was found for low-grade NHL, recent studies have shown promising results in other types of lymphoma, even Mantle cell and aggressive diffuse large cell disease.
Lymphomas are sensitive to radiation, and radioimmunotherapy delivers total-body radiation in a more directed and continuous fashion (12), with more selectivity for tumor tissues than for normal background viscera. The irradiated cells are arrested at the G2 phase of the growth cycle, induces DNA damage with an impaired repair mechanism, and finally culminates in apoptosis. Moreover, the radioisotope exerts a cytotoxic effect over a spheric volume in its immediate vicinity and thereby targets inaccessible and antigen-deficient tumor cells by the crossfire effect (13,14), thus alleviating refractoriness.
Many of the available radioimmunotherapy options use murine monoclonal antibodies and hence are more prone to causing a human antimouse antibody reaction. This problem limits their use in NHL patients, and retreatment is associated with a progressively increasing risk of hypersensitivity reactions. Hence, radioconjugation of the chimeric monoclonal anti-CD20 antibody is an effective strategy to circumvent the development of human antimouse antibody and allow safe retreatment. Radioiodination of rituximab is an easy and safe method and has been done in the nuclear medicine laboratory by the chloramine T method (15,16).
MATERIALS AND METHODS
Thirteen patients (6 male and 7 female; age range, 30–70 y; median, 61 y) with biopsy-proven B-cell NHL with CD20 positivity on immunohistochemistry were recruited for this prospective dosimetric study (Table 1). To be included, the patients had to be planned to receive rituximab-based chemotherapy in a medical oncology facility, have an absolute neutrophil count of at least 1,500 × 106/L, a platelet count of at least 100,000 × 106/L, and a bone marrow biopsy showing at least 15% normal cellularity and less than 25% lymphoma cells.
Demographic Data
The types of lymphoma included diffuse large cell B-cell lymphoma (39% of patients, one of whom had the gastric form), follicular lymphoma (30%), mantle cell lymphoma (15%), splenic marginal zone lymphoma (8%), or primary central nervous system lymphoma (8%). The patient with primary central nervous system lymphoma had undergone surgery for the same. All patients had undergone at least 2 cycles of chemotherapy with rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone. None of the enrolled patients had thrombocytopenia (hence, dose capping at 65 cGy was not required).
The patients received rituximab-based chemotherapy under medical oncology supervision. Soon afterward (4–6 h), they were administered a small diagnostic dose (∼259–444 MBq [∼7−12 mCi]) of the indigenously produced radioiodinated rituximab by intravenous infusion in 0.9% normal saline over 15–20 min.
Anterior and posterior serial planar whole-body γ-camera images were taken soon after the infusion (before and after voiding) and at days 1, 2, 4, and 6. All imaging were performed on a Siemens Symbia dual-head camera equipped with 1.0-cm NaI(Tl) crystals and high-energy collimators. A 15% energy window around 364 keV, the dominant γ-ray energy of 131I, was applied. During each whole-body image, a source of 131I with known activity was used as a reference standard for dosimetry calculations.
Image Analysis
The images were further analyzed using Syngo MI software, version VA60A/VA46A, on a Siemens workstation. All 5 scans were compared, and regions of interest were drawn over the whole body (anterior and posterior) and a 131I source with known activity placed alongside the patient during each scan. From each region of interest, counts were obtained and the geometric mean calculated for the whole body and the 131I source. From these counts, we calculated an attenuation factor and, hence, the activity retained in the patient’s body.
The administered activity (radiopharmaceutical dose) that would give a whole-body absorbed radiation dose of 75 cGy (17–20) (normal platelet count ≥ 150,000/μL) and 65 cGy (17–20) (platelet count of 100,000–150,000/μL) was calculated by 2 methods.
In the first method, the cumulative-activity method, the time–activity curve for each patient is constructed from activity retained in the patient’s body using Origin Pro 8 SRO software (Origin Lab Corp.). Whole-body cumulative activity is estimated by calculating the area under the curve (from time zero to time when extrapolated graph touches baseline [when percentage injected activity is almost negligible, that is, the body is cleared of activity]), which, when multiplied by the patient-specific S factor for 131I (calculated from a given value of 9.9E−06 cGy/μCi-h for a 73.0-kg reference person), gives the mean absorbed radiation dose (cGy). Using the unitary method, the dose that would give a whole-body absorbed radiation dose of 75 cGy (or 65 cGy, depending on the platelet count) is calculated: this is the desired dose to administer. The absorbed radiation dose for the whole body is estimated according to the MIRD scheme as follows: mean absorbed radiation dose (cGy) = cumulative activity × S factor.
The second method of calculating the administered activity is the residence-time method. Percentage retained activity is plotted versus time on semilogarithmic graph paper and used to determine the residence time, which is defined as the time for the semilogarithmic plot to reach 0.37 times the injected activity. Activity-hours (mCi-h) was the product of the amount of radioactivity and the residence time. For calculation of patient-specific therapeutic dose, the first step was to divide the activity-hours by the patient-specific residence time. The activity-hours to deliver a 75-cGy total-body dose with 131I for a given body mass was determined and used in this method. The therapeutic dose was calculated as previously described (20): therapeutic dose (mCi) = [activity-hours (mCi-h)/residence time (h)] × [desired total-body absorbed radiation dose (65 or 75 cGy)/75 cGy].
Serial γ-camera whole-body images were analyzed with respect to time by visual, semiquantitative, and quantitative approaches to determine the pharmacokinetics and clearance pattern. Pixel-matched background-corrected regions of interest were drawn around the major critical organs (heart, lung, liver, spleen, and kidney) on the serial planar images in both anterior and posterior projections. The geometric mean of the anterior and posterior counts was obtained. The organ-specific dosimetry was performed with CT-based organ volume calculations, and the residence time in each organ was calculated. Organ-specific absorbed radiation doses for both the diagnostic and the therapeutic radiopharmaceutical dose (calculated by projecting the diagnostic dose to the therapeutic activity) to these organs were calculated according to the standard MIRD formulation. As per convention, the maximum dose-limiting organ-specific dose to the organs was considered to be 20 Gy (2,000 rad).
RESULTS
Whole-Body Clearance Pattern
The residence time of the indigenous radiopharmaceutical (time required for whole-body activity to drop to 37% of injected activity, as calculated from a semilogarithmic graph of percentage injected activity vs. time) ranged from 40 to 100 h (mean, 69.54 h; median, 73 h).
Whole-body clearance of the radiopharmaceutical was assessed by the percentage of injected activity remaining in the body as obtained by the counts from the serial γ-camera images. Two components of clearance were noted: rapid and slow. The rapid component represented exponential clearance and was between 48 and 72 h in all patients. The slow component, which when extrapolated touched the baseline (representing near-complete to complete clearance of activity from the body), was between 190 and 330 h (mean total clearance time, 230 h). Within the first 48 h (the second day) at least 50% of the injected activity was cleared from the body in all the patients, and by 144 h (the sixth day) at least 80% was cleared.
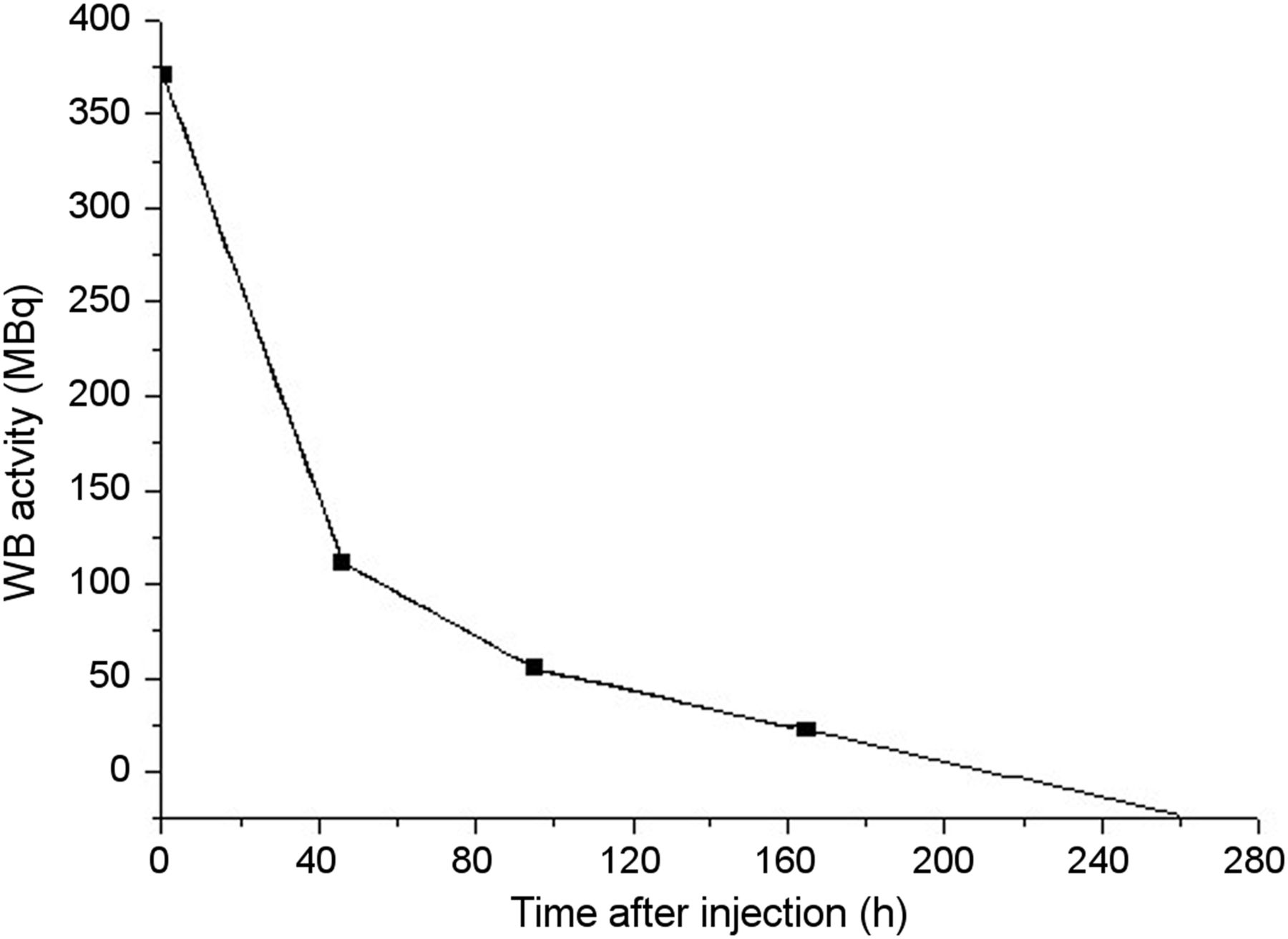
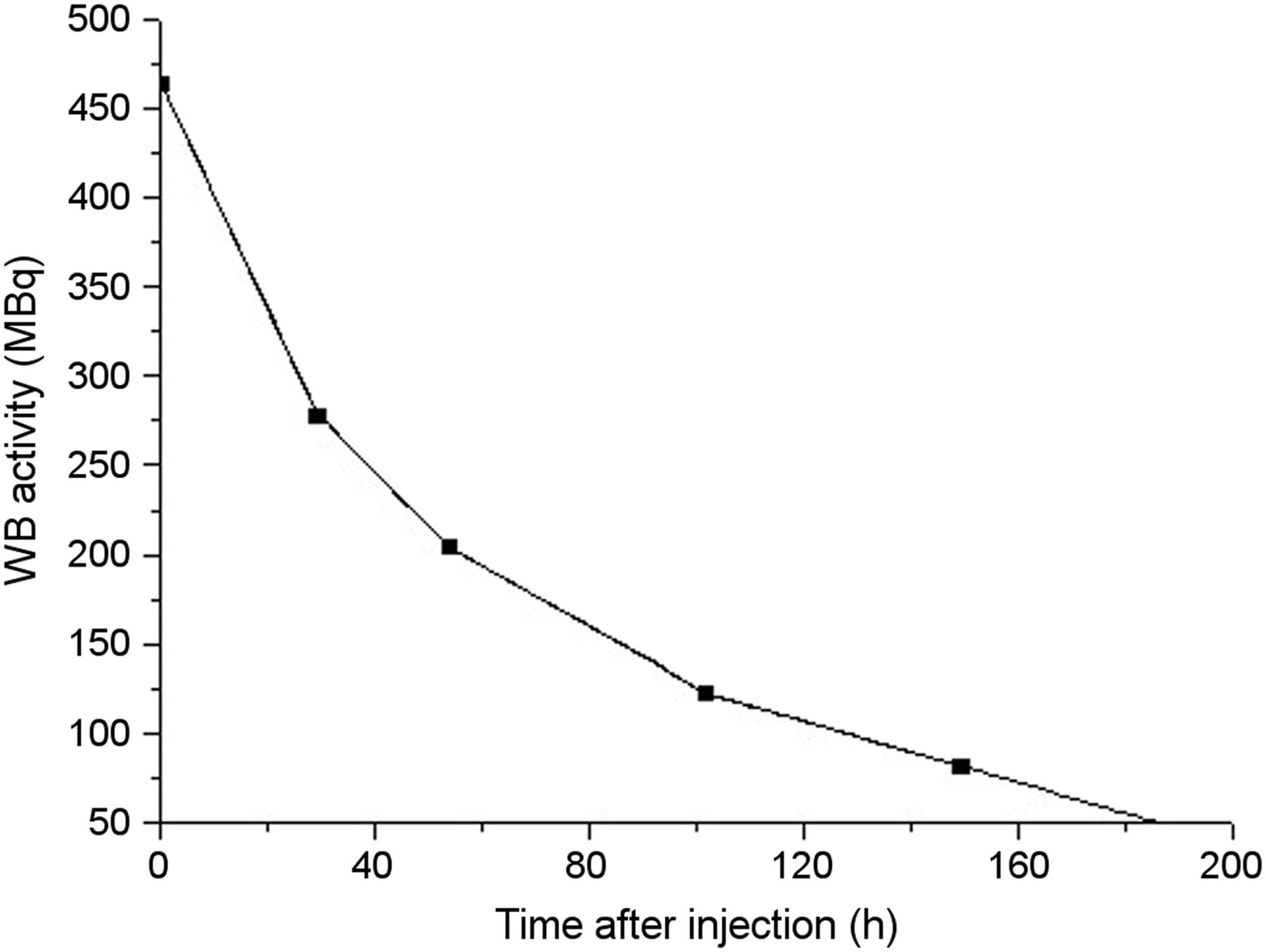
The time–activity curves of the patients with the fastest clearance and slowest clearance, hence requiring administration of the minimum and maximum calculated doses (to give a whole-body absorbed radiation dose of 75 cGy), are shown in Figures 1 and 2. Analyzing both curves, we can see that in the patient requiring the lowest administered dose (3,095.42 MBq [83.66 mCi]), the rapid component is almost negligible, and about 240 h (10 d) is needed for complete clearance of the radiopharmaceutical from the body. On the other hand, the patient requiring the maximum dose (6,330.33 MBq [171.09 mCi]) has a steep, rapid component, with more than 70% of the injected activity being cleared within the first 48 h. The slow component of the time–activity curve represents clearance of the remaining less than 30% of the injected activity, and about 210 h (8.75 d) is needed for complete clearance of the radiopharmaceutical from the body.
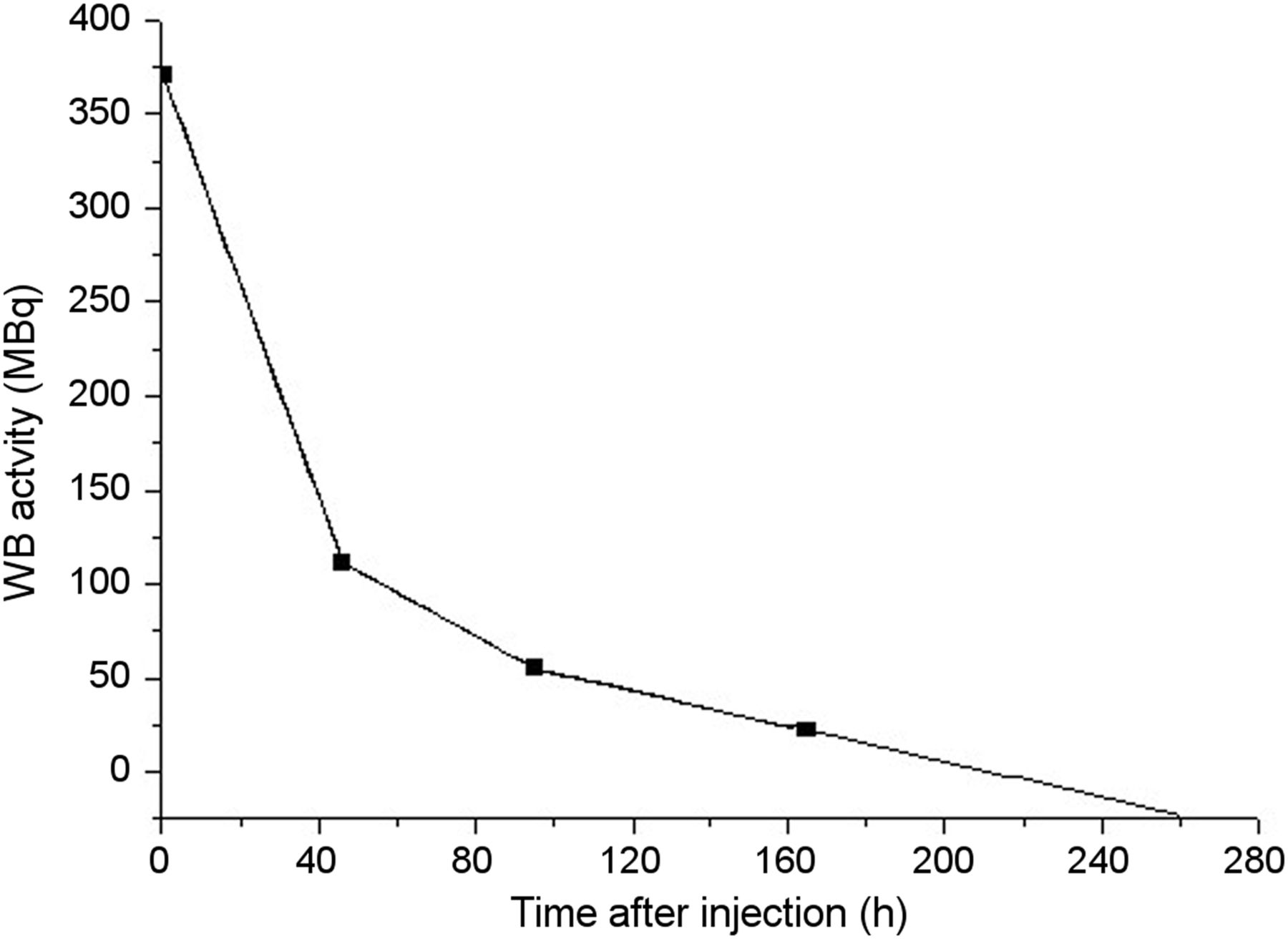
Time–activity curve of patient requiring minimum dose. WB = whole body.

Time–activity curve of patient requiring maximum dose. WB = whole body.
Individual-Organ Clearance Pattern
Clearance of radiopharmaceutical from the major organs nearly followed the whole-body clearance pattern, that is, initial rapid or exponential clearance followed by prolonged slow clearance.
The radiopharmaceutical showed a prolonged residence in the blood pool (including heart) and in major normal organs (liver, spleen, and kidneys) (Figs. 3–5). The maximum mean absorbed radiation dose per unit of diagnostic 131I activity injected was in the spleen (1.14 mGy/MBq), followed by the heart (0.97 mGy/MBq). In calculating the organ that received the maximum absorbed dose, we did not consider blood pool and spleen to be critical dose-limiting organs because the blood pool shows physiologic prolonged clearance and the spleen tolerates a higher absorbed dose, which may be desirable because the spleen is frequently an involved or primary site. In almost all patients, after the blood pool and spleen, the lungs (0.25 mGy/MBq) received the maximum dose per unit of injected activity, followed by the liver and kidneys (0.18 mGy/MBq). The maximum absorbed radiation dose in an individual patient was received by the spleen (3.51 mGy/MBq) of a patient who had splenic marginal zone lymphoma with splenomegaly. The mean absorbed radiation doses to the major organs, with diagnostic and proposed therapeutic doses and mean organ residence times, are shown in Table 2. The comparative clearance fractions and therapeutic doses calculated by the cumulative-activity method and the residence-time method are shown in Table 3 and Figure 6.
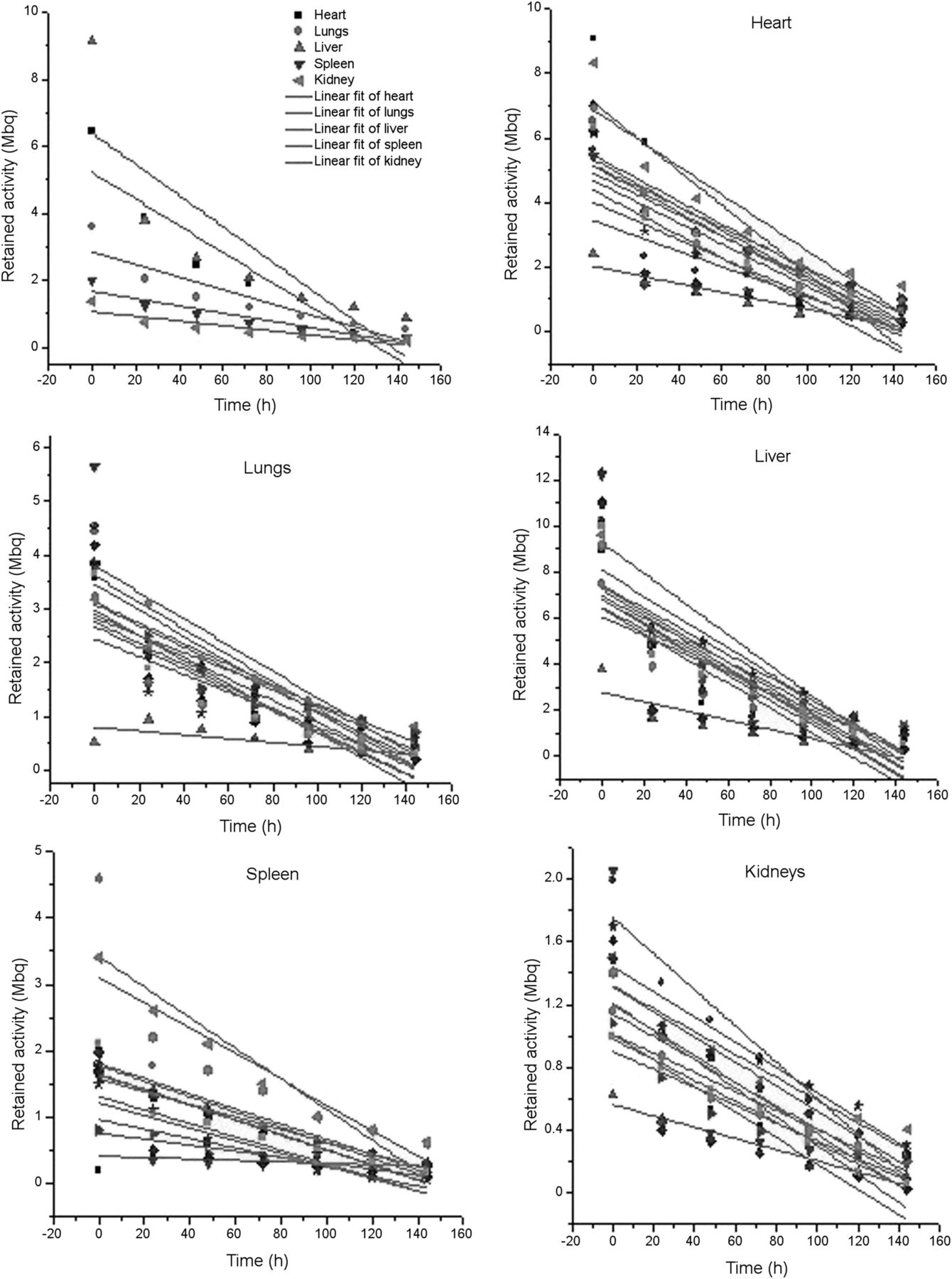
Mean and patientwise organ-specific clearance pattern from various major organs over time.
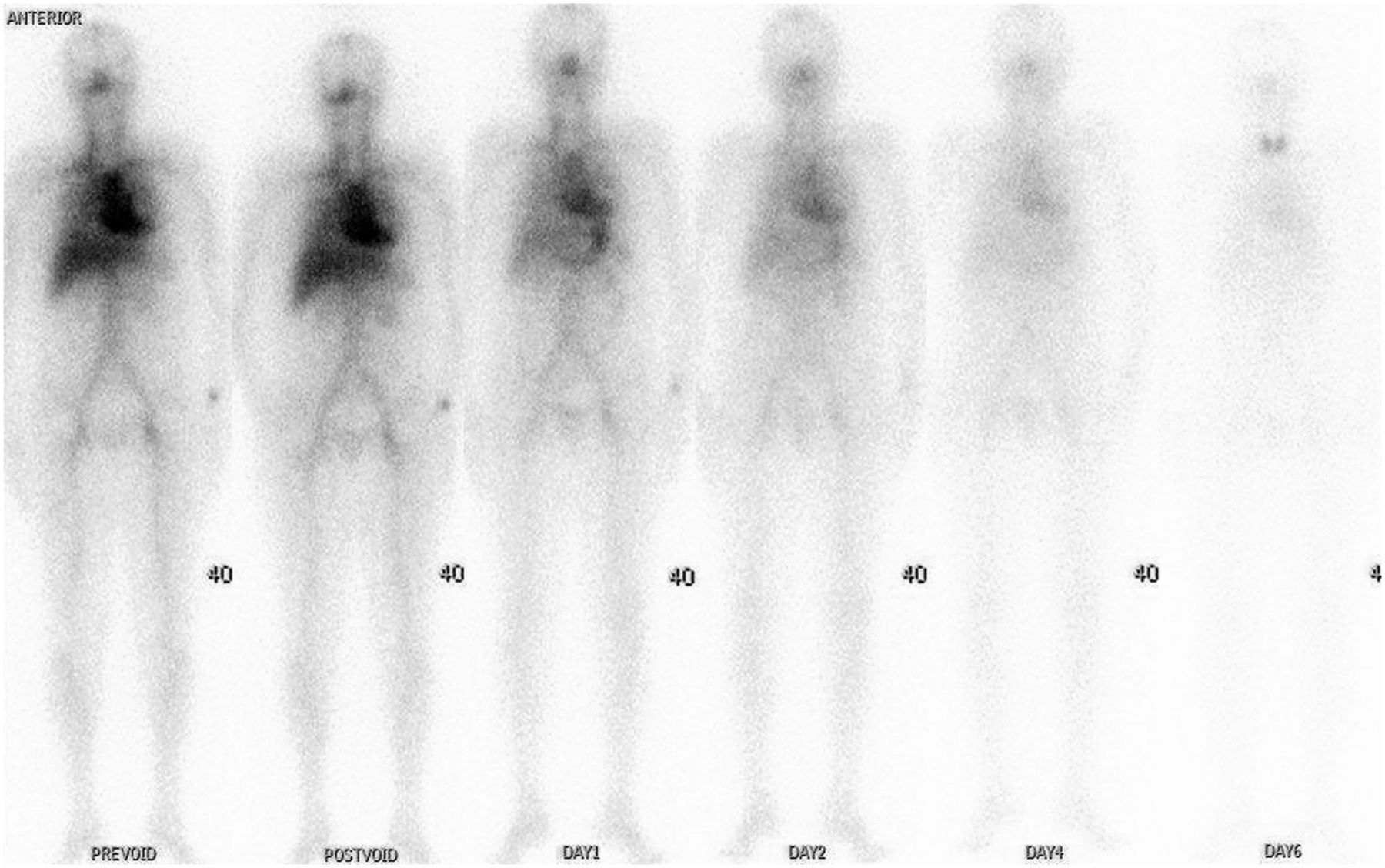
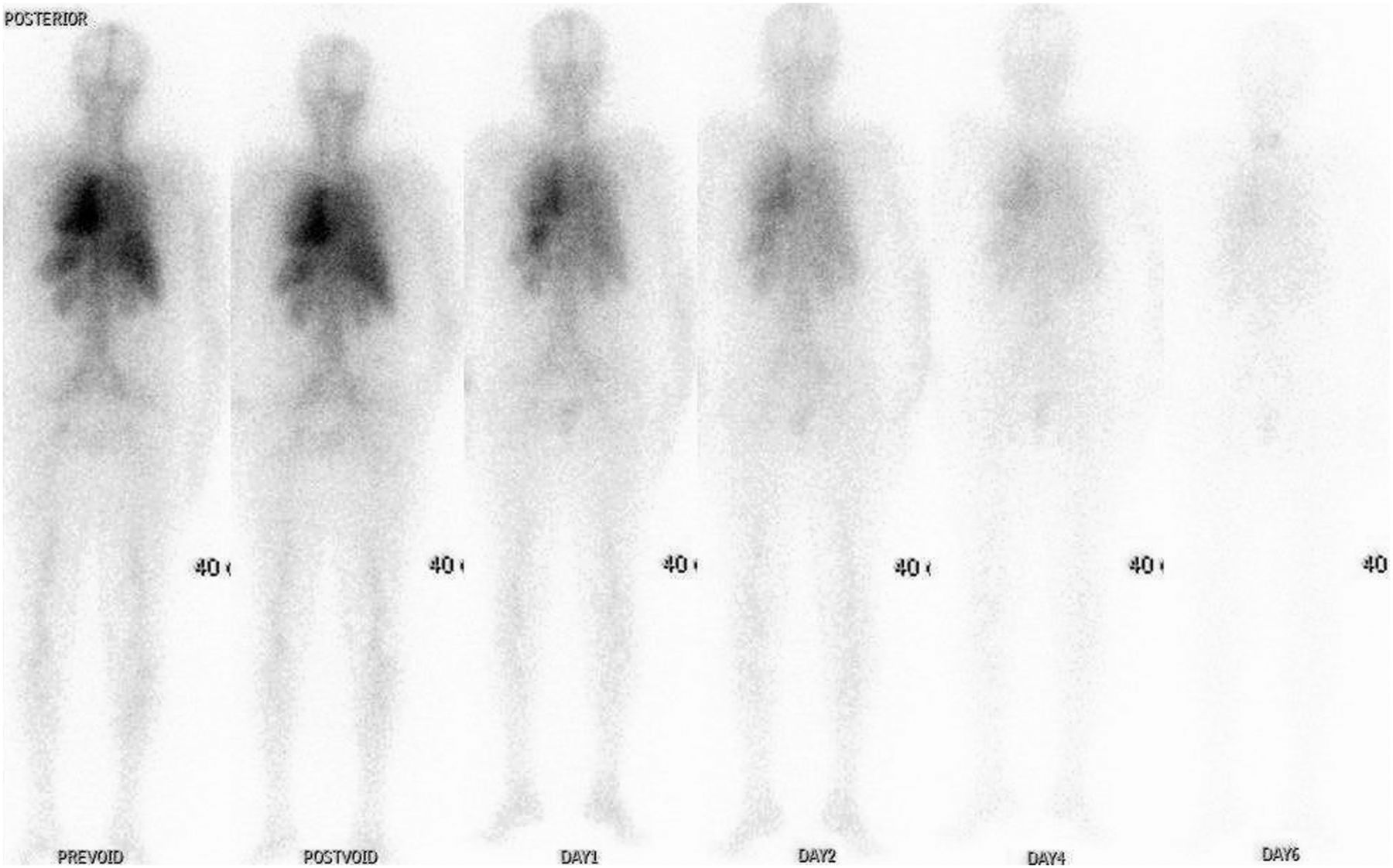
Anterior projection of serial biodistribution and clearance pattern of indigenous 131I-rituximab.
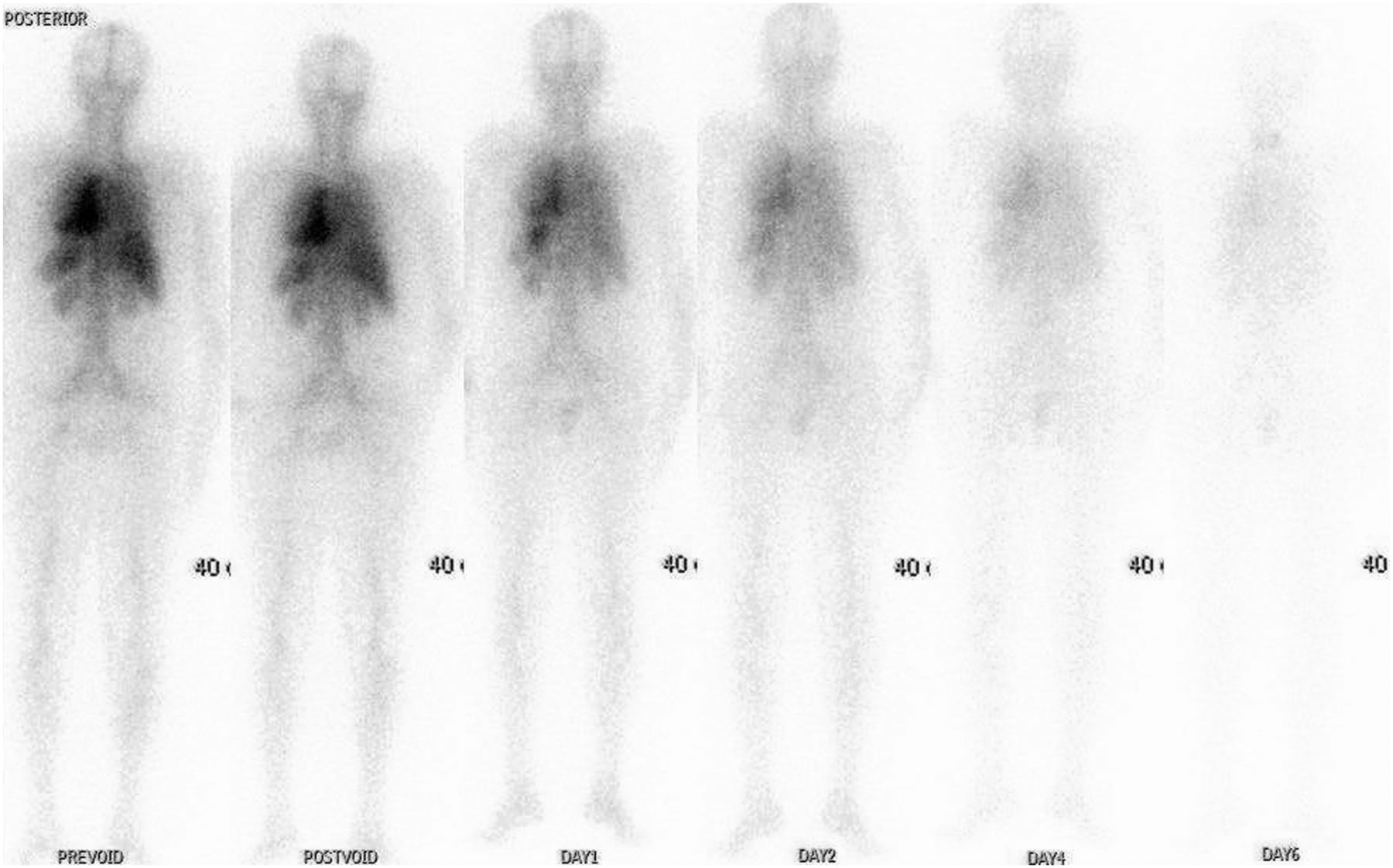
Posterior projection of serial biodistribution and clearance pattern of indigenous 131I-rituximab.
Mean Absorbed Radiation Dose per Unit of Diagnostic and Therapeutic 131I Injected and Mean Organ Residence Time
Clearance Fractions and Therapeutic Doses Calculated by Cumulative-Activity Method and Residence-Time Method
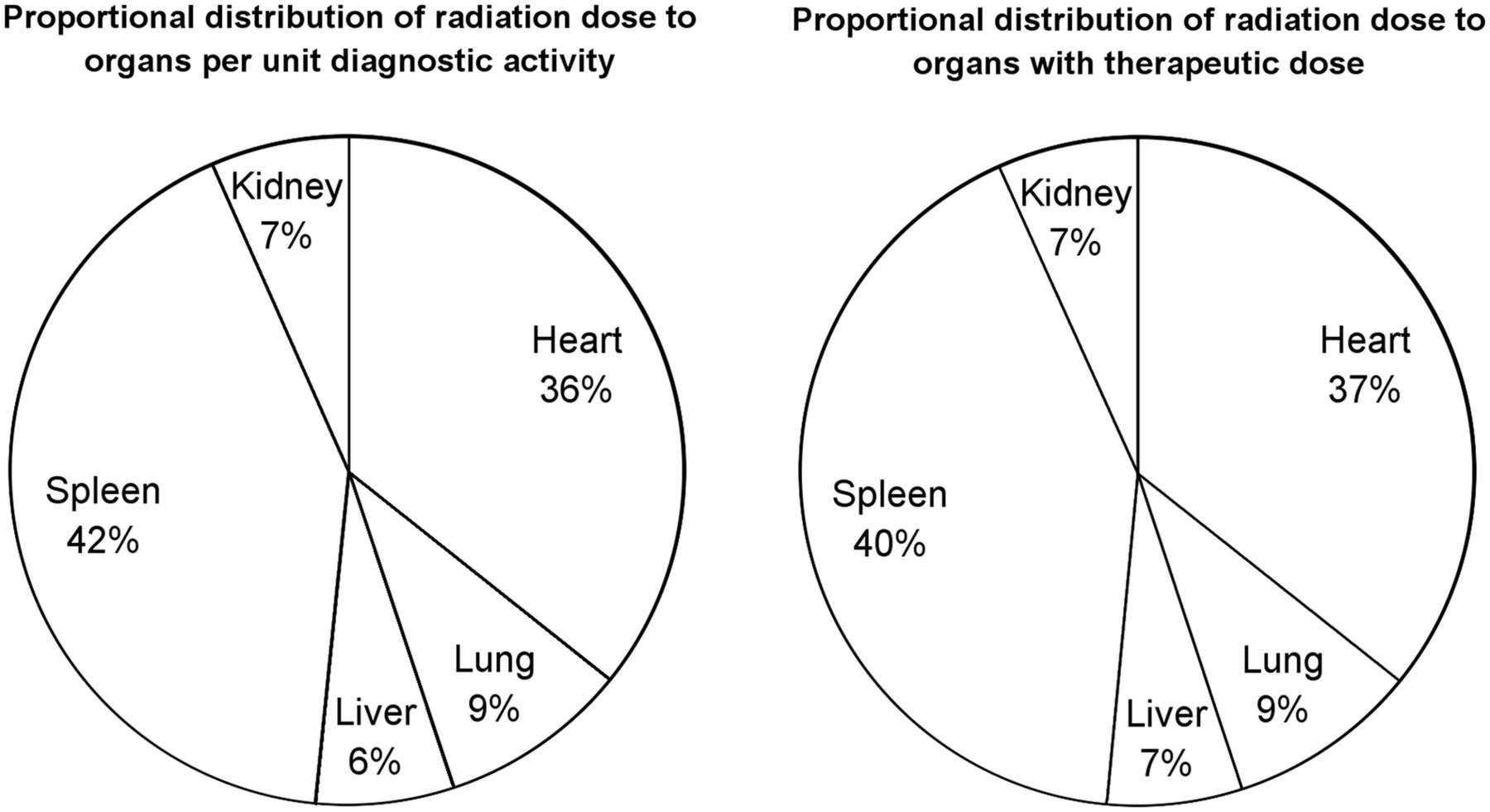
Organwise distribution of mean absorbed radiation dose per unit of diagnostic activity and with proposed therapeutic dose of radiopharmaceutical injected.
In most patients, we noticed the 2 components of clearance, fast and slow, and most such patients showed an obvious difference between the therapeutic doses calculated by the 2 methods. However, in a few such patients, for whom clearance did not show 2 distinct components, the calculated therapeutic doses were more or less comparable (≤10%–12% variation). A single-component clearance pattern was seen in 4 patients with minimal lesions or complete remission, whereas patients with residual tumor generally showed the 2 distinct components. The mean residence time was 69.54 h.
Patient-Specific Administered Doses
The patient-specific administered dose calculated using the cumulative-activity method ranged from 3,095.42 to 6,330.33 MBq (83.66–171.09 mCi), with a mean of 3,986.01 ± 863.95 MBq (107.73 ± 23.35 mCi) and a median of 3,697.41 MBq (99.93 mCi).
The patient-specific administered dose calculated using the residence-time method ranged from 2,654.75 to 6,210.45 MBq (71.75–167.85 mCi), with a mean of 3,576.42 ± 927.59 MBq (96.66 ± 25.07 mCi) and a median of 3,421.02 MBq (92.46 mCi).
With the residence-time method, the therapeutic dose required to deliver 75 cGy was slightly less than with the cumulative-activity method. The error ranged from 0% to 22%, with a mean of 10.56%.
DISCUSSION
Although a combination of rituximab with established chemotherapy regimens has brought about an improvement in overall response rate, progression-free survival, and overall survival in patients with newly diagnosed B-cell NHL (21–23), the prognosis for relapsed or refractory B-cell NHL is often poor. Radioimmunotherapy has demonstrated promise not only for recurrent or refractory indolent or transformed B-cell NHL (24) but also as first-line treatment (25) and as consolidation treatment for a first remission (26). 131I-tositumumab and 90Y-ibritumomab tiuxetan are approved for treatment of relapsed or refractory indolent or transformed B-cell NHL. 90Y-ibritumomab tiuxetan furthermore is approved as consolidation therapy after remission induction in previously untreated follicular lymphoma. Despite these encouraging results, the use of radioimmunotherapy remains infrequent (27).
Two advantages of indigenously labeled rituximab over commercially available rituximab can be envisaged. First, a single regimen of the commercial product can cost up to $30,000 (∼21 lakh Indian rupees), precluding its routine use in developing countries, whereas the indigenously labeled product is expected to cost less. Second, the antibodies used in the commercially approved radiopharmaceuticals are murine antibodies and hence may cause human antimouse antibody reactions in as many as 50%–60% of patients. Because rituximab, being a chimeric antibody, has a lower reported rate of human antimouse antibody reactions, retreatment can be undertaken safely.
The primary aim of this study was to determine the therapeutic dose of the indigenous 131I-rituximab and to study its biodistribution. Our study with 13 patients demonstrated that the calculated therapeutic doses were comparable to those of the commercial products. A specific feature of this study was the comparison between therapeutic doses calculated by the cumulative-activity method and therapeutic doses calculated by the residence-time method. The latter were comparable to those of the cumulative-activity method (Table 3).
Among the major critical organs, apart from the blood pool (3.77 Gy) and spleen (4.02 Gy), those with the maximum mean absorbed radiation dose at the proposed therapeutic dose were the lungs (0.97 Gy), followed by the liver (0.69 Gy) and kidneys (0.7 Gy). The absorbed doses per unit of injected diagnostic radioactivity (in mGy/MBq) were comparable to those for the therapeutic dose and were greatest for the lungs (0.25), followed by the liver and kidneys (0.18), apart from blood pool or heart (0.97) and spleen (1.14). In none of these organs was there any dose-limiting radiation exposure at the standard prescribed therapeutic doses. The maximum absorbed radiation dose received by individual organs with the administration of a therapeutic dose was well within the conventional limit of 20 Gy. Similar to the diagnostic data, the maximum organ-specific absorbed radiation dose was received by the spleen (11 Gy) of a patient who had splenic marginal zone lymphoma with splenomegaly.
The fast and the slow components of clearance were studied and showed wide interpersonal variations. Patients with minimal lesions or complete remission showed a single-component clearance pattern.
This study had limitations due mainly to the small number of patients, the variation in their stages of treatment, and the fact that the MIRD schema is based on various assumptions. Rajendran et al. demonstrated a CT volume–adjusted absorbed dose per unit of radioactivity (in mGy/MBq) of 1.30 for the lungs, 0.92 for the liver, 0.76 for the kidneys, 1.40 for the spleen, and 0.22 for the whole body (28). The trend in the results obtained by this study resonated well with the available literature, and administration of the indigenous product for therapeutic indications was found to be safe.
At present, radioimmunotherapy is underutilized in routine practice despite approval by the responsible regulatory authorities in the United States and in Europe. Treating physicians seem hesitant to recommend radioimmunotherapy to a larger number of potentially eligible patients. This hesitation might be due to the availability of alternative nonradioactive therapies and to various logistic, educational, and economic concerns (29). Cost is certainly a limiting factor in developing countries. Data from Leahy and Turner demonstrated that radioimmunotherapy with 131I-rituximab in routine clinical outpatient practice is a safe option for relapsed or refractory indolent NHL, with half the patients achieving a durable complete response that has potential for repeat treatment (30). Recently, a possible role for radioimmunotherapy was evaluated as part of the conditioning regime before allogeneic stem cell transplantation in patients with persistent high-risk B-cell NHL. In two phase 2 trials, radioimmunotherapy proved feasible and safe in combination with a reduced-intensity conditioning regime consisting of fludarabine and total-body irradiation (2 Gy), with acceptable toxicity even in elderly and heavily pretreated patients (31,32). These results provide an important basis for studying the cost effectiveness of the indigenous product in approved and future indications. The present study results add an important perspective to this particular topic.
CONCLUSION
The indigenous 131I-rituximab product has demonstrated kinetics similar to commercially available, approved radiopharmaceuticals, with the advantage of a lower human antimouse antibody response due to the pharmaceutical’s being a chimeric antibody rather than murine. Considering the promising data obtained for this indigenously developed product, its use in lymphoma care for a larger patient benefit can hardly be overemphasized.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Nov. 9, 2018.
REFERENCES
- Received for publication June 28, 2018.
- Accepted for publication October 2, 2018.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}