


Article Figures & Data
Figures
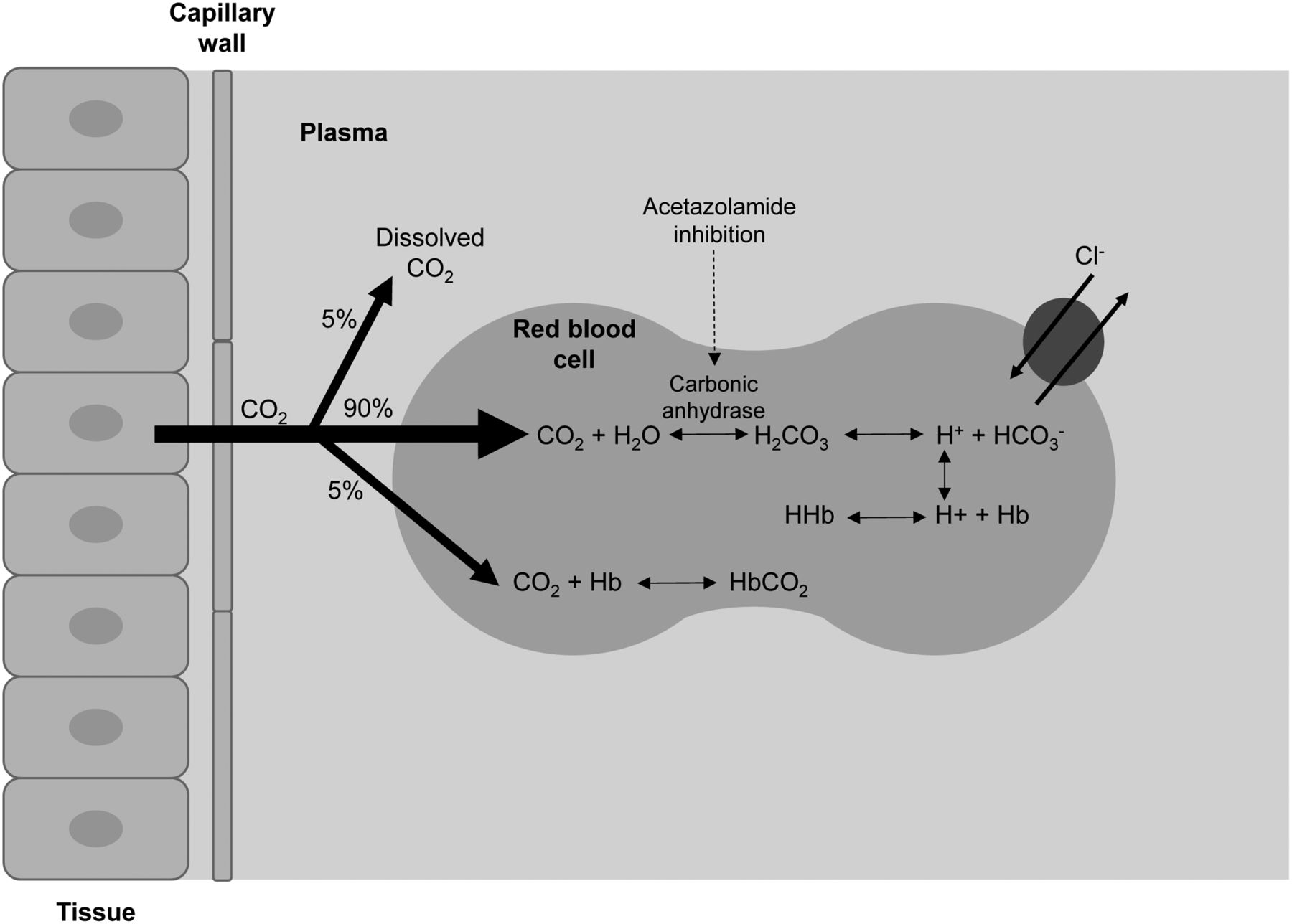
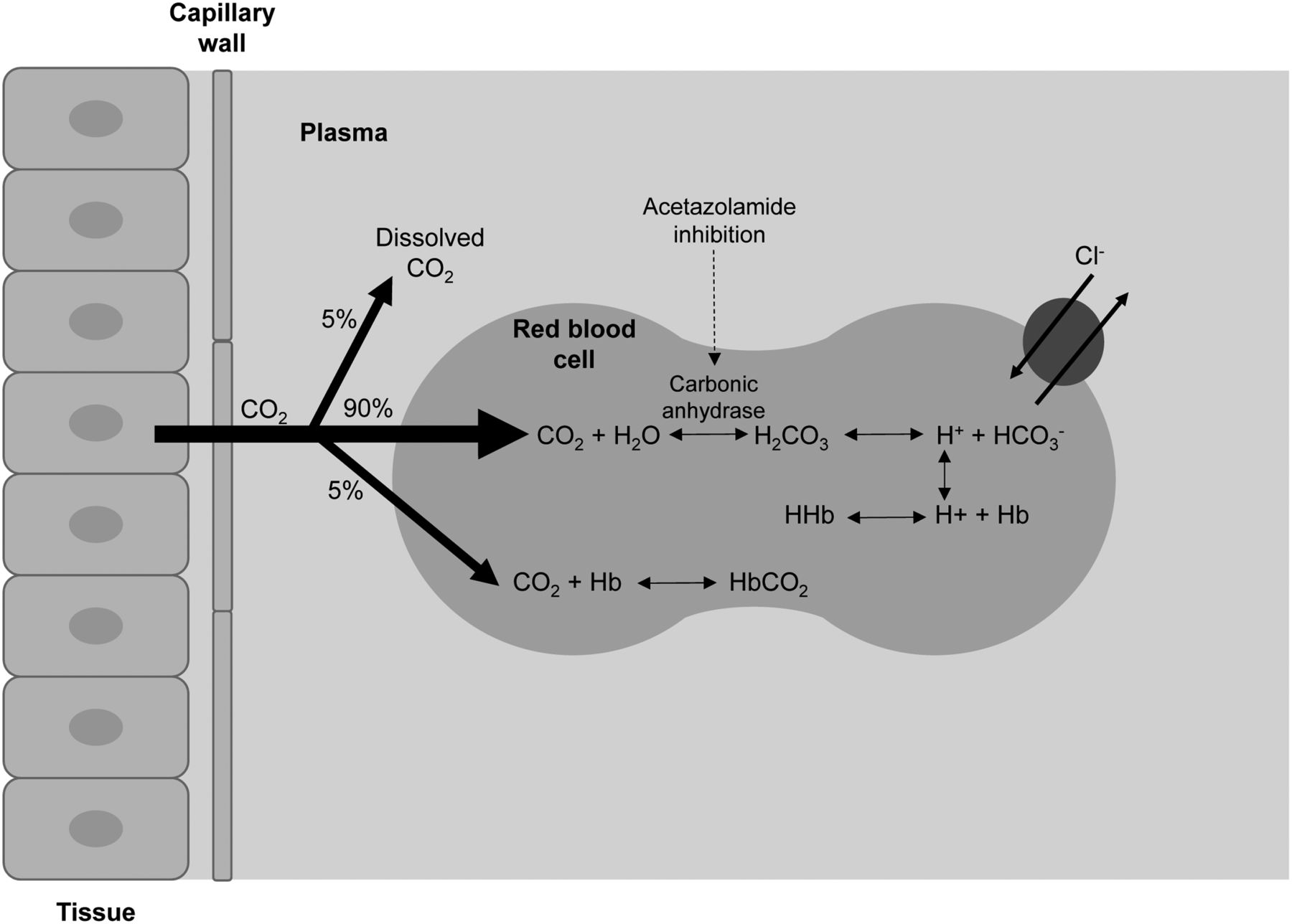
- FIGURE 1.
Schematic representation of impact of acetazolamide in inhibiting carbonic anhydrase and increasing serum carbon dioxide, which leads to increased cerebral perfusion.
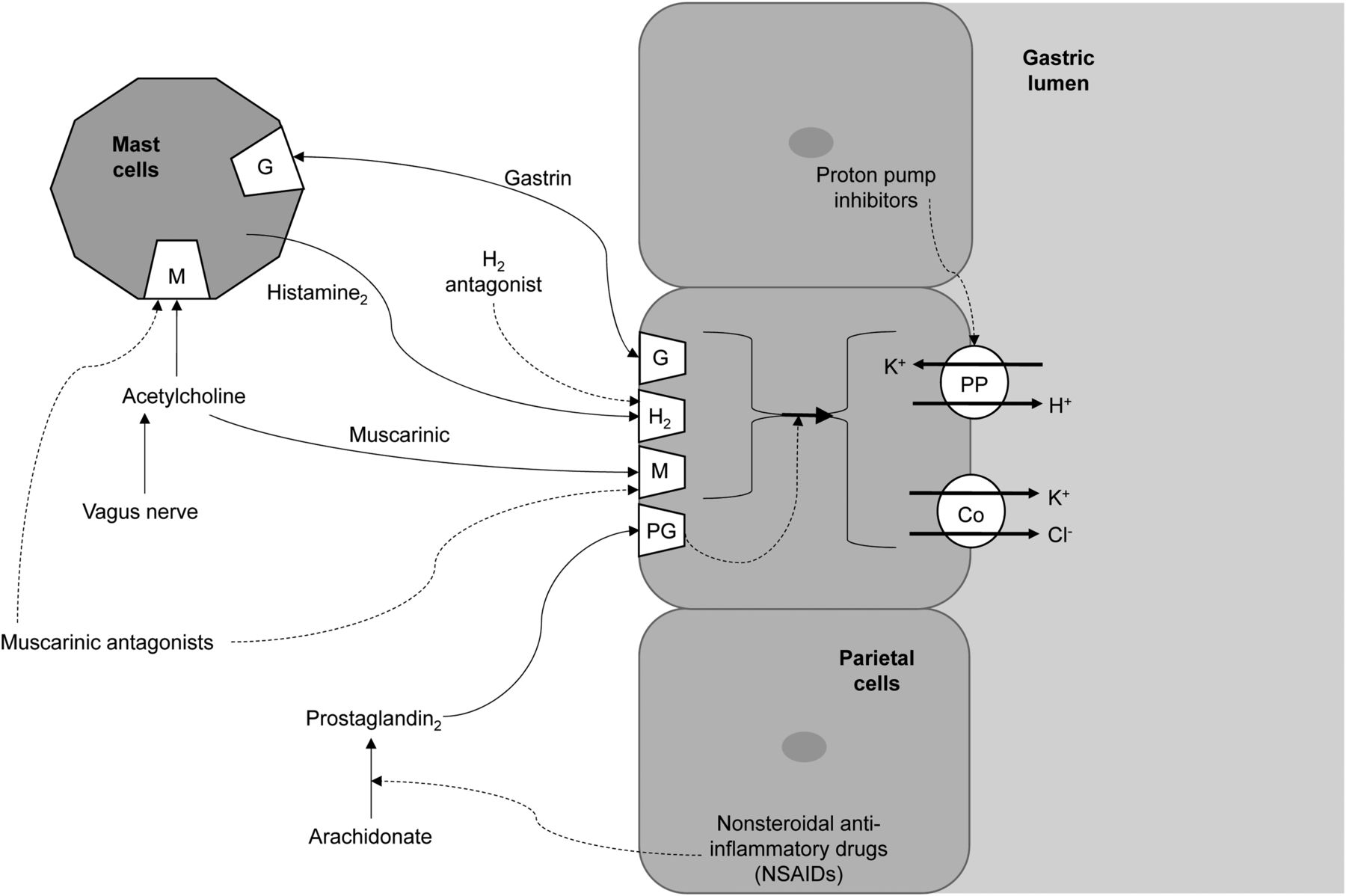
- FIGURE 2.
Schematic representation of action of receptors responsible for gastric acid secretion (solid lines) and inhibitors of gastric acid secretion (dashed lines). Co = cotransporter.
Tables
Drug Indication Dose Pharmacokinetics Mechanism of action Contraindications/cautions Adverse effects/interactions Acetazolamide Cerebral flow reserve in brain perfusion studies 1 g diluted in sterile water intravenously over 2 min Onset, 30 min, slow; peak, 2 h; duration, 12 h; half-life, 3–6 h; 70%–90% plasma protein–bound Carbonic anhydrase inhibitor; causes sodium bicarbonate dieresis and vasodilation in brain in response to cerebral carbonic acidosis (carbon dioxide clearance inhibition) Contraindicated in sodium or potassium depletion, hyperchloremic acidosis, Addison disease, closed-angle glaucoma, and severe renal or liver dysfunction; caution in acute stroke, kidney or liver disease, diabetes, gout, lupus, hypotension, and pregnancy Tingling sensation, flushing, dizziness, blurred vision, confusion, nausea, headache, tinnitus, and allergic reaction; potential interactions with aspirin, lithium, cyclosporin, amphetamines, other diuretics, antihypertensives, salicylates, hypoglycemics, phenytoin, sodium bicarbonate, anticoagulants, and cardiac glycosides Cimetidine Enhanced detection of Meckel diverticulum 300 mg orally, 4 times over 24 h in adults and 20 mg/kg in 20 mL of saline intravenously over 20 min in children Onset, 0.5–1 h; peak, 1 h; half-life, 2 h; duration, 4–6 h; 20% plasma protein–bound H2 histamine receptor blocker; reduces gastric acid secretion and volume and impedes 99mTc-pertechnetate secretion Contraindicated in known hypersensitivity; caution in renal or cardiovascular dysfunction Headache, dizziness, diarrhea, muscle pain, confusion, and bradycardia; potential interactions with medications metabolized in liver; can also alter bioavailability of drugs reliant on stomach pH for absorption Ranitidine As above 300 mg orally for adults and 1 mg/kg intravenously over 20 min for children Onset, 60 min; peak, 2–3 h; half-life, 2–3 h; duration, 4–13 h; 15% plasma protein–bound As above As above As above Omeprazole 40 mg orally morning before and morning of scan Onset, 60 min; peak, 2 h; half-life, 0.5 h; duration, 3–5 d; 95% plasma protein–bound Proton pump inhibitor (irreversible); suppresses stomach acid secretion and impedes 99mTc-pertechnetate secretion Contraindicated in known hypersensitivity; caution in liver dysfunction; ranitidine is preferred in pediatrics Infrequent but include headache, dizziness, abdominal pain, diarrhea, nausea, vomiting, and rash; potential interactions with diazepam, phenytoin, warfarin, and medications reliant on gastric acidity for absorption Duration is period of significant or measurable effect. Some adverse effects are more likely when used therapeutically than in single interventional doses.
Drug Indication Dose Pharmacokinetics Mechanism of action Contraindications/cautions Adverse effects/interactions Chloral hydrate Sedation in children 30–50 mg/kg to maximum of 1 g Good gut absorption, rapid metabolism, and onset of action in 30–60 min; elimination half-life of 7–11 h and significant effects for 4–8 h Prodrug; is converted to trichloroethanol, which modulates GABA to cause CNS depression Contraindicated in significant liver, kidney, or cardiac dysfunction; caution in respiratory insufficiency and known hypersensitivity Nausea, vomiting, diarrhea, dizziness, ataxia, drowsiness, headache, confusion, and paradoxic excitement; potential interactions with ethanol, warfarin, and CNS depressants Diazepam (benzodiazepam) Anxiolytic (claustrophobia) 1–10 mg orally individualized by age and liver/kidney function Onset, 15–45 min; peak 30–90 min; half-life 46 h; duration can be prolonged; 100% bioavailability orally; 98%–99% PPB; biphasic elimination with rapid component followed by slower half-life of 1–2 d Causes inhibition through modulation of GABA and neuronal inhibition Contraindicated in chronic obstructive pulmonary disease, severe liver or lung disease, sleep apnea, and hypersensitivity; caution in depression, dependence, glaucoma, liver or kidney dysfunction, depression, pregnancy, and lactation Drowsiness, sedation, muscle weakness, ataxia, vertigo, headache, confusion, and paradoxic excitement, all with increased risk in the elderly; potential interactions with CNS depressants, including antihistamines and drugs metabolized by liver Bisacodyl Laxative for differentiating stool from disease Single oral dose, 5–15 mg Minimal absorption after oral administration; onset, 6–8 h Stimulant laxative; increases stool water retention and peristalsis Contraindicated in bowel obstruction; caution in liver impairment Gastric irritation, cramping and fluid or electrolyte imbalance; potential interactions with medications that change gastric acidity Heparin Blood labeling to prevent clotting 10–15 units/mL of blood being labeled in vitro Highly plasma protein–bound with variable elimination based on dose (slow for low doses); rapid onset with effects lasting 3–6 h Combines with antithrombin III to inactivate numerous clotting factors Contraindicated in known sensitivity, acute bacterial endocarditis, and high bleeding risk; caution in anticoagulant use, asthma, liver dysfunction, and animal protein allergy Bleeding, hemorrhage, and hypersensitivity; potential interaction with anticoagulants (including NSAIDs and aspirin) PPB = plasma protein bond; NSAIDs = nonsteroidal antiinflammatory drugs.
Duration is period of significant or measurable effect. Some adverse effects are more likely when used therapeutically than in single interventional doses.





{kind=link}
{kind=link}