


Abstract
We report the gratifying response of functioning metastatic neuroendocrine tumor with carcinoid heart disease (uncontrolled by long-acting octreotide) to treatment with 177Lu-DOTATATE. This response favorably altered the clinical course of the patient, enabling corrective valvular surgery, enhancing health-related quality of life, improving symptoms (from New York Heart Association grade III at baseline to grade I after 6 cycles), stabilizing the disease, and substantially reducing the level of 5-hydroxyindole acetic acid. Avoiding concerns about volume overload by administering amino acids over a relatively prolonged period of 7.5–8 h during peptide receptor radionuclide therapy could be particularly helpful and could be conveniently adopted in this clinical setting. Considering the significantly shortened overall survival of patients with carcinoid heart disease, the relative paucity of available treatment options, and the risk of complications during corrective surgery on poorly controlled functioning disease, 177Lu-DOTATATE can emerge as a potent option in this group of patients.
- 177Lu-DOTATATE PRRT
- carcinoid heart disease
- neuroendocrine tumor
- long-acting octreotide
- 5-hydroxyindole acetic acid (5-HIAA)
Located mostly in the gastrointestinal system, neuroendocrine tumors can originate and are derived from neuroendocrine stem cells in the gut wall, lungs, mediastinum, thymus, liver, pancreas, bronchus, ovaries, prostate, and kidneys. Carcinoid syndrome develops in about 50% of the population with neuroendocrine tumors (1). Carcinoid heart disease manifests in many patients with carcinoid syndrome (2), but the prevalence dropped to approximately 20% after the introduction of newer therapies such as somatostatin analogs and 177Lu-DOTATATE, along with everolimus, sunitinib, and the combination of capecitabine and temozolomide (3). A definitive cure requires appropriate presurgical management and control of the functioning disease to improve the feasibility and outcome of surgery. Adjunctive peptide receptor radionuclide therapy (PRRT) in this clinical setting has not been widely explored. We report a case of carcinoid heart disease that was managed successfully by such therapy (177Lu-DOTATATE), with a documented objective and symptomatic response that enabled the patient to be considered for corrective surgery.
CASE REPORT
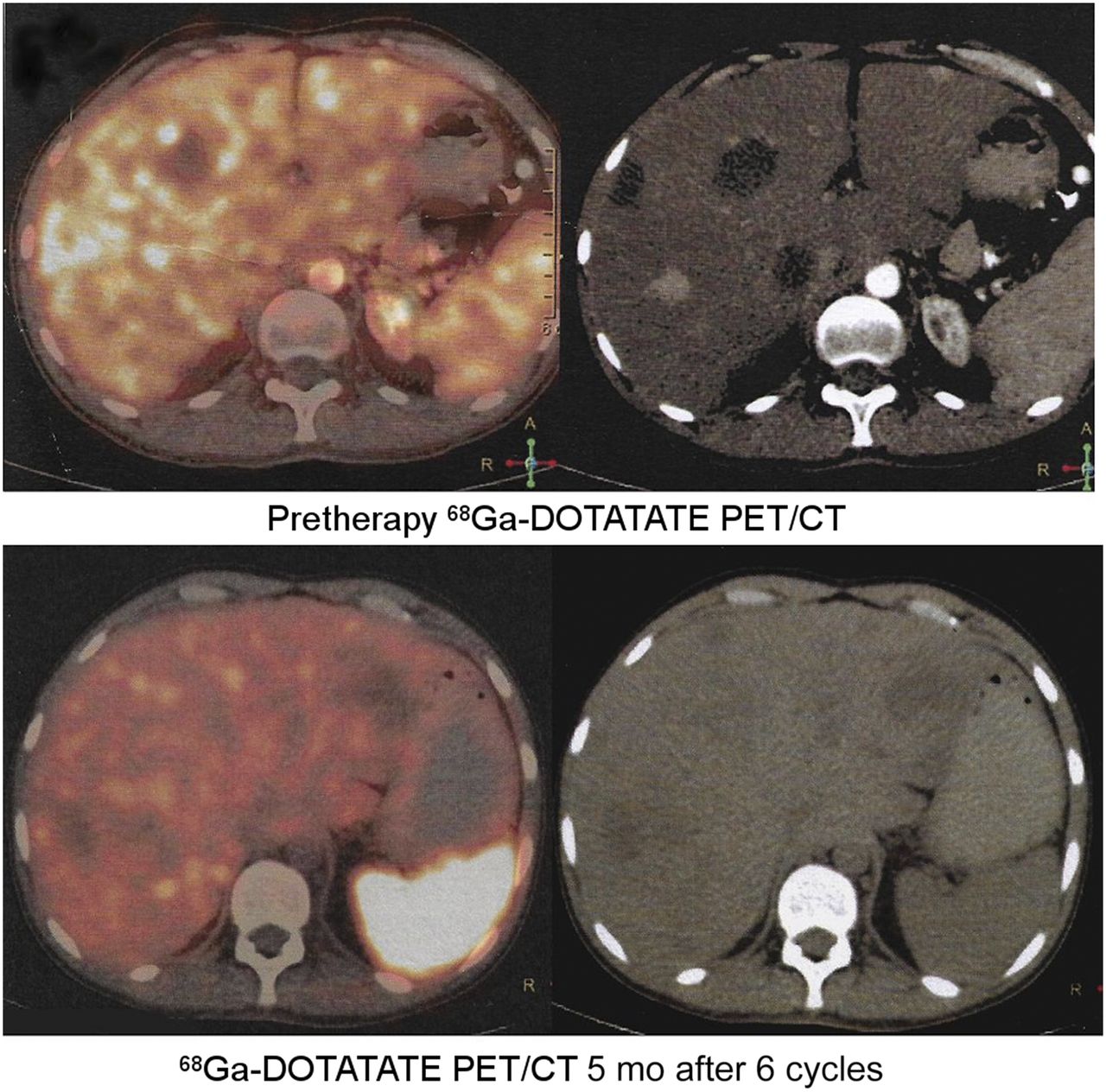
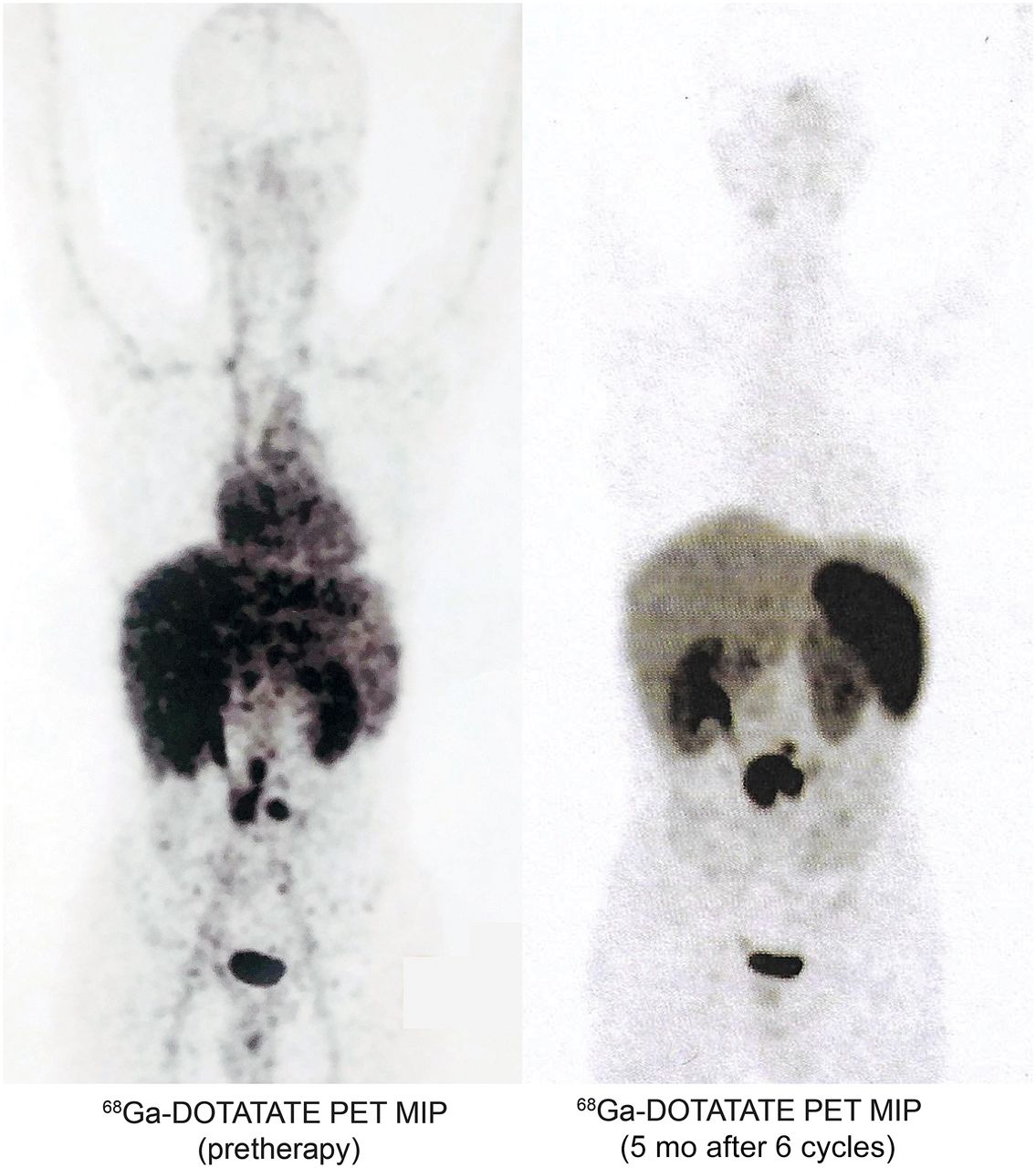
A 30-y-old man who had been diagnosed with a grade II jejunal neuroendocrine tumor metastatic to the liver and abdomen was found clinically and on 2-dimensional (2D) echocardiography to have the complication of carcinoid heart disease. At the time of his referral for consideration of PRRT, he presented with severe flushing, diarrhea, and dyspnea of grade III on the New York Heart Association scale, uncontrolled by monthly long-acting octreotide injection. Pre-PRRT 2D echocardiography revealed a severely dilated right atrium, severe tricuspid stenosis, moderate pulmonary stenosis, and severe tricuspid regurgitation. The opinion of a cardiothoracic surgeon was sought, who deemed the disease inoperable because of suboptimal cardiac function. The patient was thus considered for PRRT as a potential way to control the functioning carcinoid syndrome. The initial 2 cycles of 177Lu-DOTATATE brought about impressive symptomatic improvement, and the patient went on to receive a total of 6 cycles with a cumulative dose of 37.40 GBq. Subjective symptomatic, radiologic, biochemical, and 2D echocardiographic parameters were used to determine the treatment response. The patient showed improvement in all these parameters after completion of the 6 cycles. Particularly noteworthy was a remarkable improvement in the symptomatic scale, with the patient being asymptomatic for dyspnea at that point (from New York Heart Association grade III at baseline to grade I after 6 cycles) and with a substantial reduction of urinary 5-hydroxyindole acetic acid (5-HIAA) to nearly one sixth the baseline level. Table 1 details the chronologic summary of 24-h urinary 5-HIAA values after 3 and 6 PRRT cycles, showing a measurable decrease. On scans, the liver lesions showed a partial response whereas the primary lesion was stable (Figs. 1 and 2).
24-Hour Urinary 5-HIAA After PRRT

68Ga-DOTATATE PET/CT axial slices showing partial response of hepatic lesions.
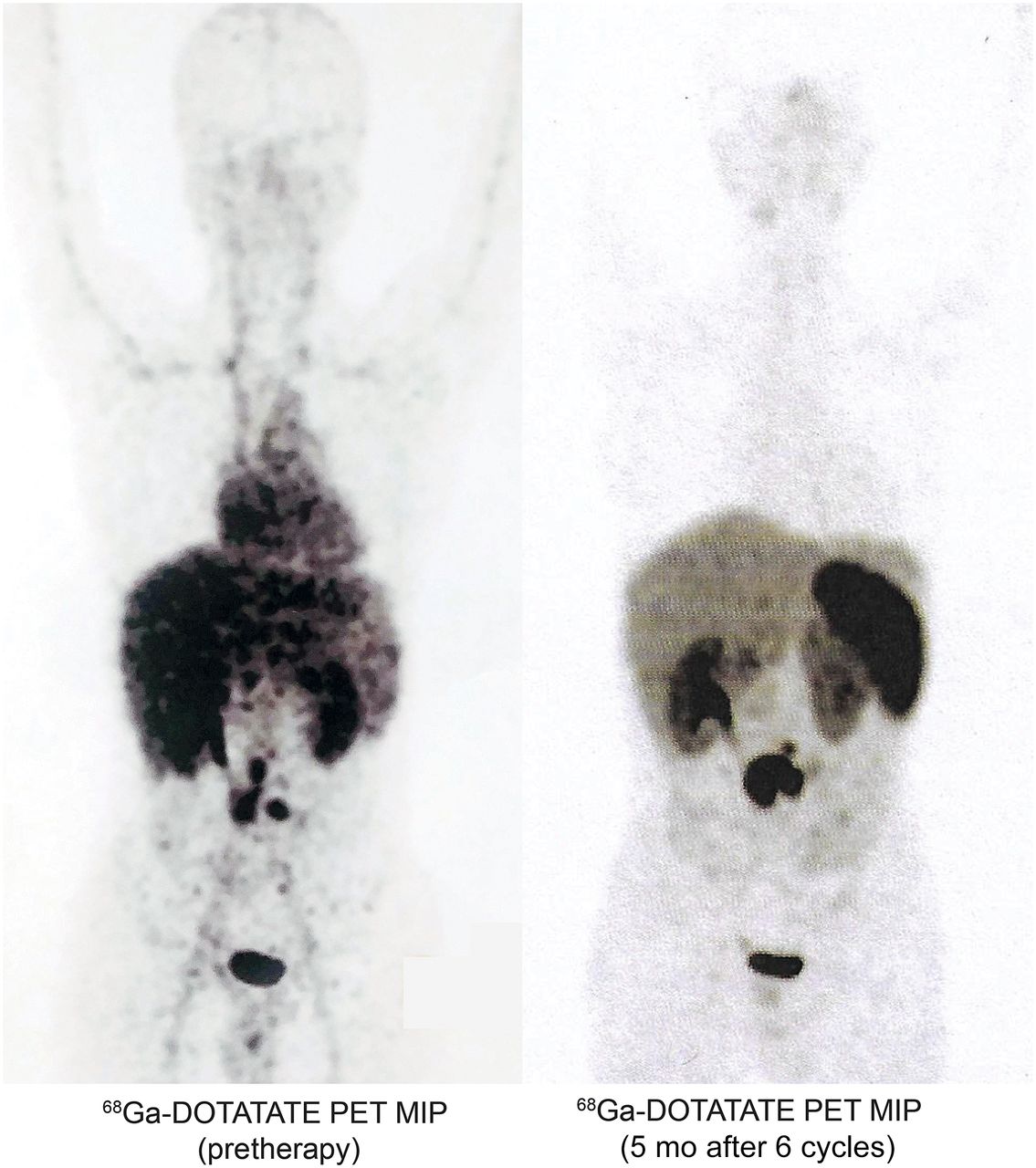
68Ga-DOTATATE PET/CT maximum-intensity projection (MIP) showing partial response of hepatic lesions.
After 6 cycles of PRRT, 2D echocardiography revealed moderate tricuspid stenosis and mild pulmonary stenosis (Table 2). In view of the better control of carcinoid symptoms and metastatic disease (including improved objective and subjective cardiac function), a cardiothoracic surgical reassessment was undertaken. The patient is currently asymptomatic and is being finalized for planned corrective surgery.
2D Echocardiography Findings
DISCUSSION
In neuroendocrine tumor, bulky hepatic involvement is an important risk factor because it leads to secretion of vasoactive substances (5-hydroxytryptamine, tachykinins, and prostaglandins) that reach the right side of the heart through the hepatic veins. The consequent deposition of fibrous tissue on the endocardial surfaces of the heart results in pathogenesis of carcinoid heart disease. The cardiac manifestations are due to these vasoactive substances released by the metastatic cells and not to direct metastatic involvement of the heart. An additional risk factor is suboptimal efficiency in dealing with these vasoactive substances (which normally are deactivated by uninvolved liver), because they produce pathognomonic pathologic changes as they reach the right side of the heart in large quantities. The resulting anatomic distortion of the valves leads to stenosis or regurgitation (4). Peak 5-HIAA level is a significant predictor of the progression of carcinoid heart disease (5); thus, urinary 5-HIAA and 2D echocardiography are important investigative options in the physicians’ armamentarium for identifying carcinoid heart disease.
Among patients with inoperable or metastatic neuroendocrine tumors, the presence of carcinoid heart disease without active management or intervention leads to a significantly shortened overall survival than in such patients without carcinoid heart disease. PRRT with or without somatostatin analogs has proven beneficial in relieving symptoms and in improving health-related quality of life and progression-free survival (6). One concern about amino acid infusion in carcinoid heart disease is volume overload in patients with cardiac insufficiency (6). Our institutional protocol of administering mixed amino acids over a relatively prolonged period of 7.5–8 h during PRRT has been particularly helpful in addressing this concern about volume overload and might be recommended to allow safe use of this treatment in patients with carcinoid heart disease. Furthermore, extending the infusion period of the amino acid solution to 10 h has been reported to further reduce the absorbed dose to the kidney by up to 39% (6,7).
The only definitive cure for severe right heart failure appears to be valve surgery. Mortality in patients with carcinoid heart disease is due to severe regurgitation because of morphologic defects in the right-side valves or, uncommonly, in the left-side valves (because of deactivation of the vasoactive substances in the lung parenchyma). Surgery on functioning metastatic disease increases perioperative morbidity and mortality unless there is appropriate preoperative management (8). The mortality rate in carcinoid heart disease patients undergoing surgical correction is now lower than previously. As evidenced in our case and the more recent literature (9), 177Lu-DOTATATE not only can enhance quality of life and stabilize metastatic disease but also can improve cardiac status and make more patients eligible for surgery early in the course of carcinoid heart disease.
CONCLUSION
This teaching case study illustrates the potential role of PRRT as adjunctive therapy for patients who have inoperable metastatic carcinoid syndrome with symptomatic carcinoid heart disease. By substantially improving quality of life and disease control, PRRT would better the feasibility and outcome of risky surgical procedures in this challenging group of patients. The value of prolonged amino acid infusion during PRRT in carcinoid heart disease patients is also a noteworthy consideration.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Jun. 8, 2018.
REFERENCES
- Received for publication February 21, 2018.
- Accepted for publication April 17, 2018.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.