


Abstract
Parallax error is a pitfall of pinhole scintigraphy that causes mislocalization of the findings. It is important to notice this error on pinhole thyroid and parathyroid scintigraphy and obtain additional images with a parallel-hole collimator to accurately determine the upper and lower margins of large goiters and nodules and the location of ectopic thyroid tissue and parathyroid adenomas. In this teaching case report, we revisit pinhole parallax error, present pinhole and SPECT/CT images of a patient with a large, hyperactive thyroid nodule, and review the literature and potential solutions to this important problem.
Use of a pinhole collimator is highly recommended for thyroid scintigraphy because it provides the only method of magnification, which is associated with better intrinsic resolution, contrast, and sensitivity than are obtainable with a parallel-hole collimator (1,2). However, pinhole collimators can cause geometric distortion of objects with depth (3–5). The upper and lower margins of a large goiter or nodule, and the location of ectopic thyroid tissue and parathyroid adenomas, can be incorrect on routine pinhole thyroid and parathyroid scintigraphy. Pinhole parallax error was previously reported in a case of substernal goiter and another of parathyroid adenoma (3,4). In this teaching case report, we present a case of pinhole parallax error in a patient with a large hyperactive thyroid nodule, and we briefly review the literature and discuss the potential solutions to this important problem.
CASE REPORT
A 24-y-old man with subclinical hyperthyroidism was referred to the Nuclear Medicine Department for a scintigraphic thyroid uptake study. Twenty minutes after intravenous administration of 185 MBq (5 mCi) of 99mTc-pertechnetate, routine pinhole images of the thyroid gland were obtained in right anterior and left anterior oblique views using an anterior marker. The duration of the pinhole acquisition was 150 kilo counts for each view, and the matrix size was 256 × 256. The distance from the pinhole collimator to the patient was adjusted so that the gland occupied two thirds of the field of view. Thyroid scintigraphy was performed using a SoloMobile γ-camera (DDD-Diagnostic A/S) equipped with a pinhole collimator (3-mm insert). An additional SPECT/CT image of the neck and upper mediastinum was also obtained using a GE Healthcare Discovery 670 16-slice SPECT/CT camera. First, low-dose CT was performed for attenuation correction and anatomic localization. Afterward, SPECT images were obtained at 25 s per view and 60 views. Iterative reconstruction was used for image processing. The SPECT, CT, and SPECT/CT images were reviewed in the transaxial, sagittal, and coronal planes, and a maximum-intensity projection was reviewed as well.
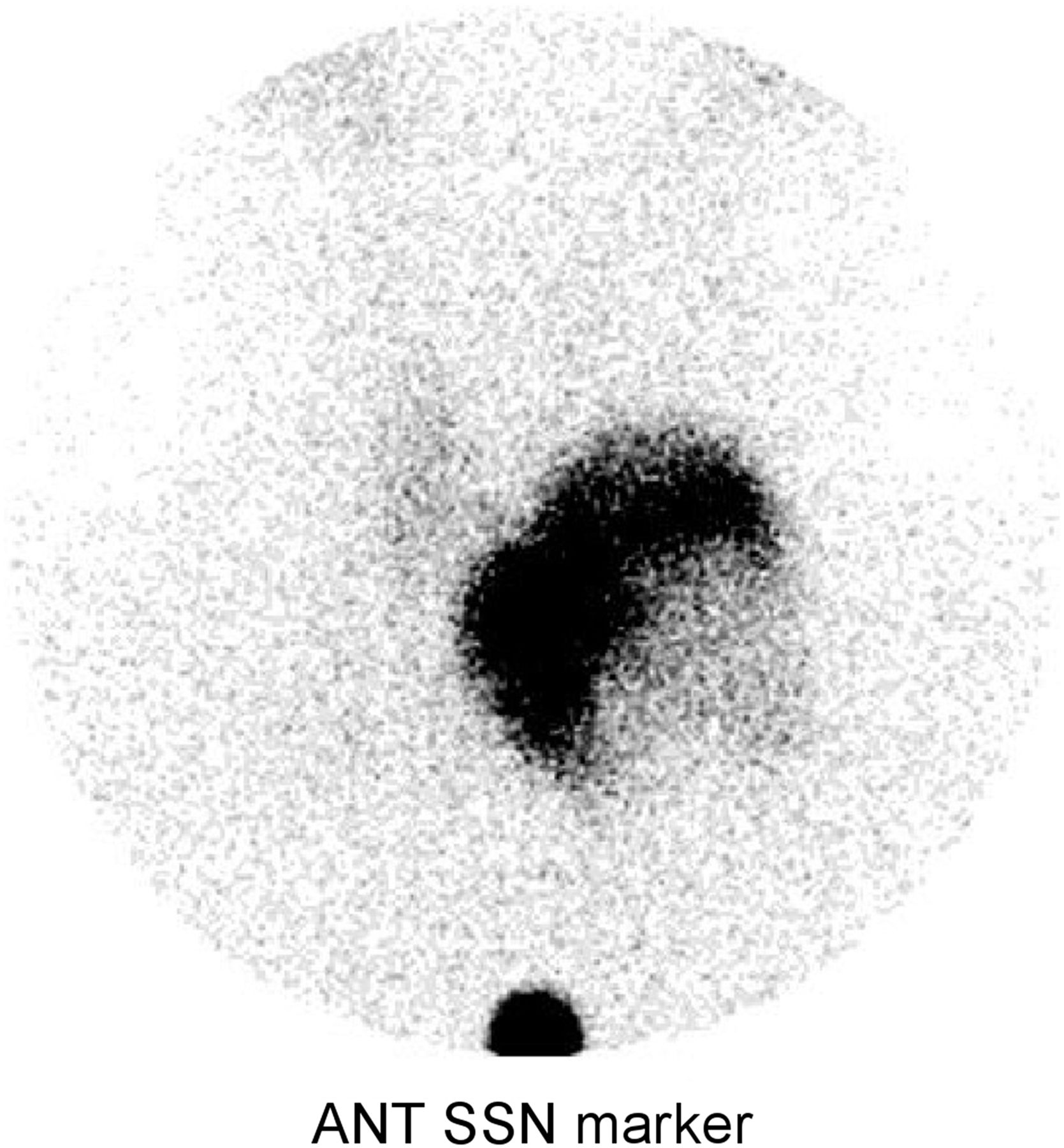
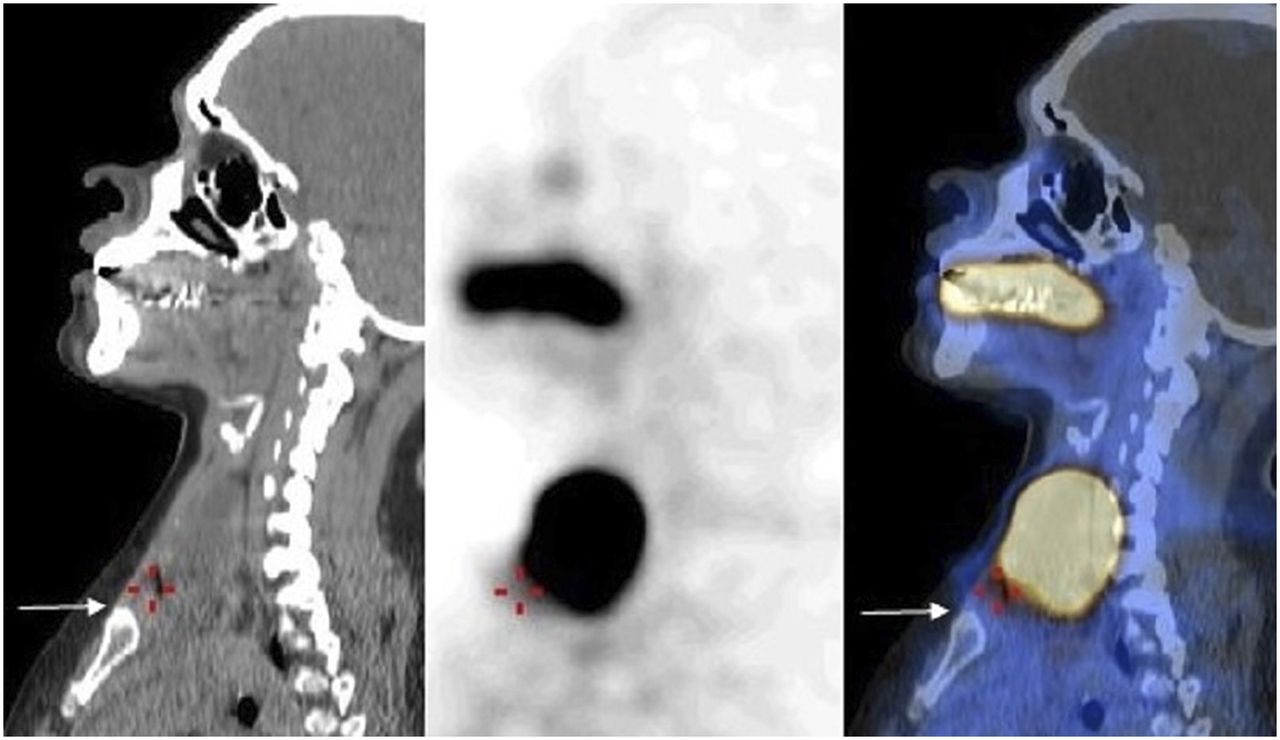
The pinhole images showed a large, heterogeneous, hyperactive nodule in the left lobe and suppression of uptake in the right lobe (Fig. 1). The lower margin of the nodule was far above the suprasternal notch. However, the SPECT/CT images showed that the lower portion of the nodule was at the level of the suprasternal notch (Fig. 2).
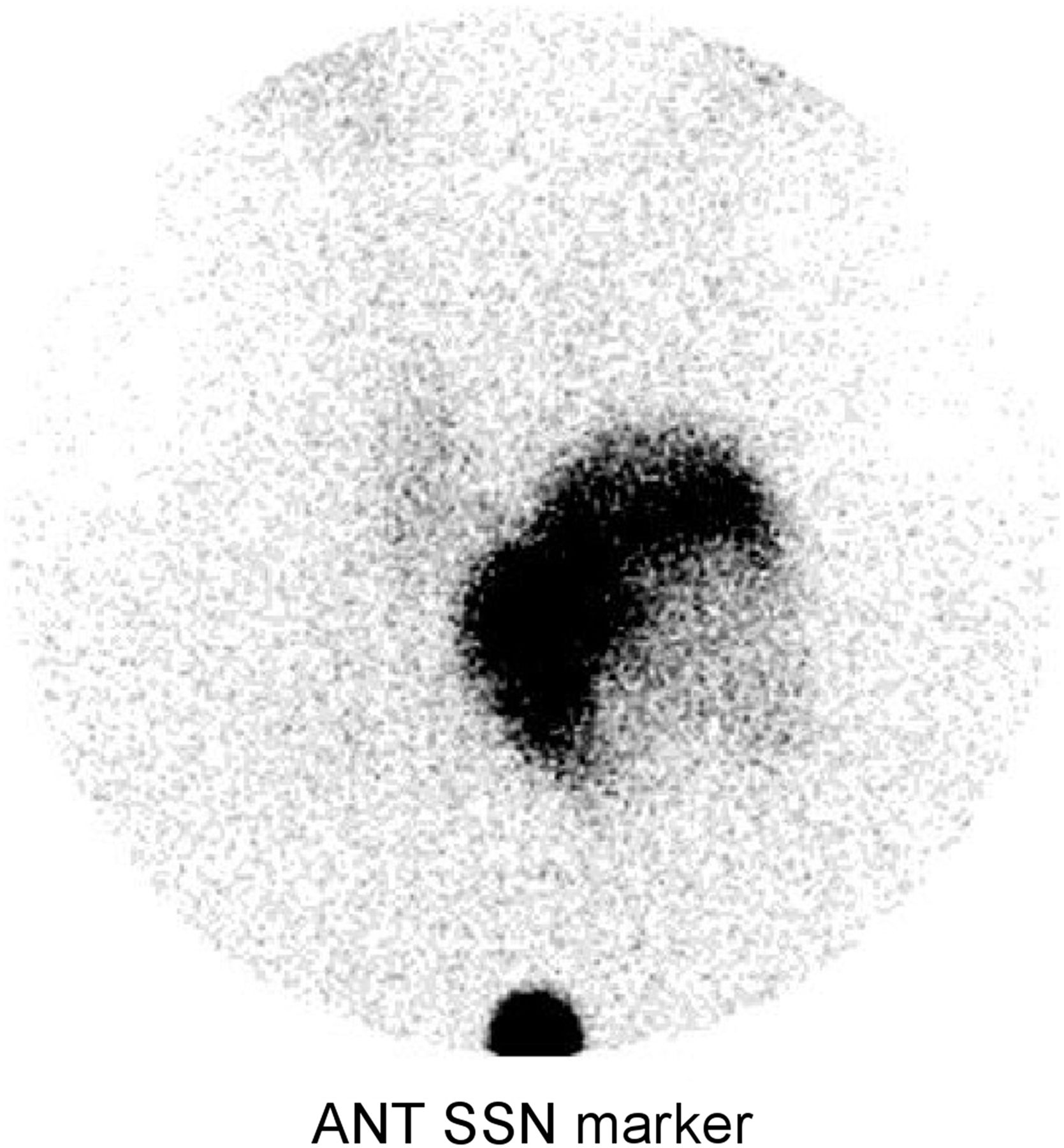
99mTc-pertechnetate anterior (ANT) pinhole image of thyroid gland with marker at suprasternal notch (SSN) reveals large, hyperactive nodule in left lobe. Nodule shows cold areas laterally, likely because of degeneration or necrosis. Remainder of thyroid gland is suppressed, with only mild activity seen in right lobe. Lower margin of this nodule is far above suprasternal notch.
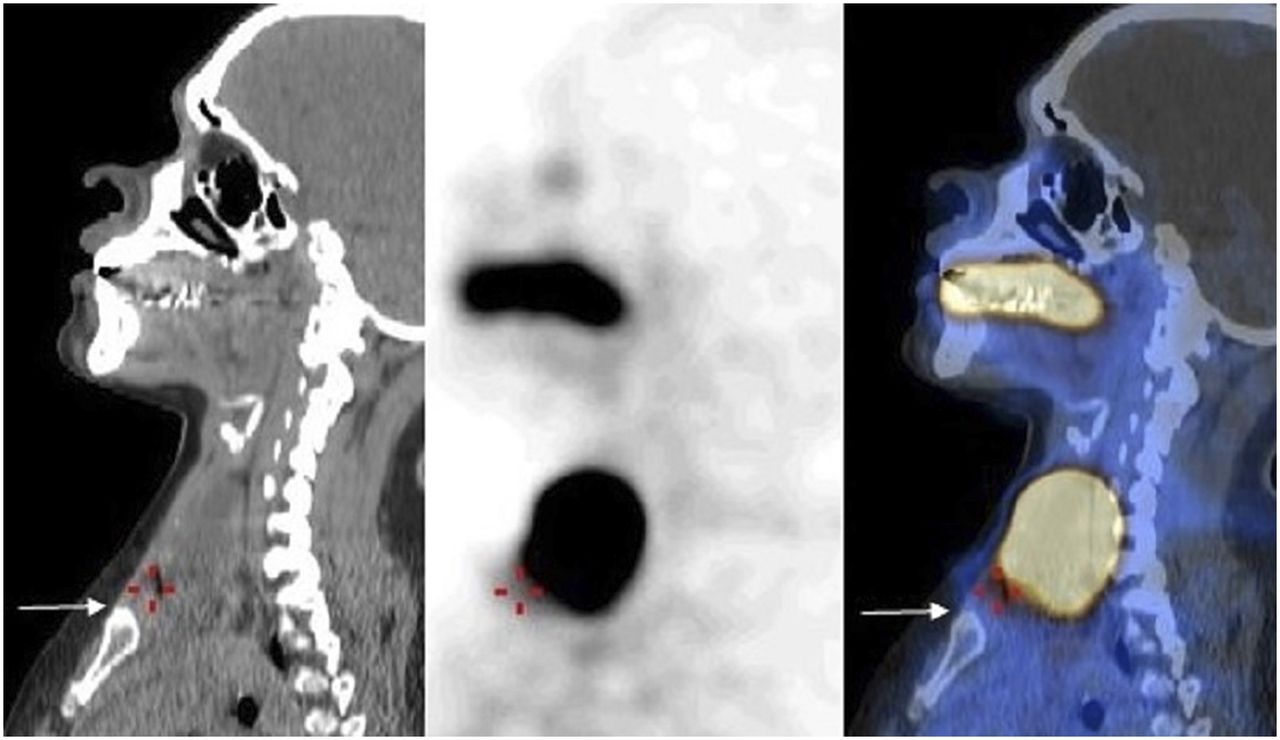
Selected 99mTc-pertechnetate sagittal CT, SPECT, and SPECT/CT images of thyroid gland show that lower margin of left thyroid nodule is at level of suprasternal notch. Arrow indicates upper margin of sternum.
DISCUSSION
The parallax error is caused by the combination of off-center positioning of the pinhole in relation to the object and the inherent minification effect of the pinhole collimator with increasing distance (3). McKitrick et al. reported the parallax error in a patient with substernal goiter who was imaged using a pinhole collimator positioned at the usual thyroid bed between the thyroid cartilage and the suprasternal notch (3). On the resulting image, the substernal portion of the thyroid appeared as if it were within the normal thyroid bed. An additional image obtained with a rectilinear scanner showed that the lower margin of the goiter was substernal. To demonstrate this parallax phenomenon, McKitrick et al. also performed a study using a thyroid phantom. Serial images were obtained at increasing depths of the phantom, which was intentionally placed off center from the pinhole. As the pinhole-to-phantom distance was increased, the thyroid image was “pulled up” to the normal location.
In another report, parathyroid adenoma was wrongly localized by pinhole 99mTc-sestamibi scintigraphy to the anterior mediastinum near a lower pole of the thyroid gland (4). After a failed surgical attempt to resect the adenoma, the patient was reimaged with a parallel-hole collimator and SPECT, which showed that the adenoma was near the heart, anterior to the carina.
In our patient, pinhole imaging erroneously showed the lower margin of the thyroid nodule to be far above the suprasternal notch. SPECT/CT helped to correctly locate the lower margin of the nodule.
This error can be avoided by centering the pinhole over the large goiter or nodule (3). In addition, using a parallel-hole collimator, a planar, SPECT, or SPECT/CT image of the thyroid and chest region (with markers at the thyroid cartilage and suprasternal notch) should also be obtained to better identify the upper and lower margins of the large goiter or nodule, determine whether it extends to the mediastinum, and locate ectopic thyroid tissue and parathyroid adenomas.
CONCLUSION
Pinhole scintigraphy is still commonly used to image the thyroid gland and is recommended for imaging parathyroid diseases. Hence, recognition of parallax error on pinhole thyroid and parathyroid scintigraphy is important, and if present, additional images should obtained with a parallel-hole collimator to accurately determine the upper and lower margins of a large goiter or nodule and the location of ectopic thyroid tissue and parathyroid adenomas.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online May 3, 2018.
REFERENCES
- Received for publication January 8, 2018.
- Accepted for publication March 5, 2018.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.