


Abstract
Coccidioidomycosis is an infection caused by inhalation of the Coccidioides fungus. Most infections remain subclinical or are confined to the pulmonary system. Disseminated disease is rare. Traditionally, a combination of imaging modalities has been used to determine disease extent. We suggest 18F-FDG PET/CT as a single first-line imaging examination to assess disease extent. We present a case of disseminated coccidioidomycosis to the lung, mediastinum, soft tissues, and skeletal system. To our knowledge, no prior case reports demonstrate such widespread disease using PET/CT.
Less than 1% of coccidioidomycosis infections result in extrapulmonary disseminated disease, and less than half of those involve the skeletal system (1). A single imaging examination with 18F-FDG PET/CT provides comprehensive assessment of disease extent.
CASE REPORT
An immunocompetent, 22-y-old African-American man was admitted for work-up and treatment of presumed pneumonia, which was refractory to empiric therapy. The patient reported 3 mo of fever, night sweats, weight loss, and difficulty breathing. He was born in Liberia, had moved to Texas 15 y earlier, and recently had traveled to Ohio. CT of the chest, abdomen, and pelvis demonstrated multiple osteolytic lesions. Left iliac lesion biopsy demonstrated coccidioidomycosis.
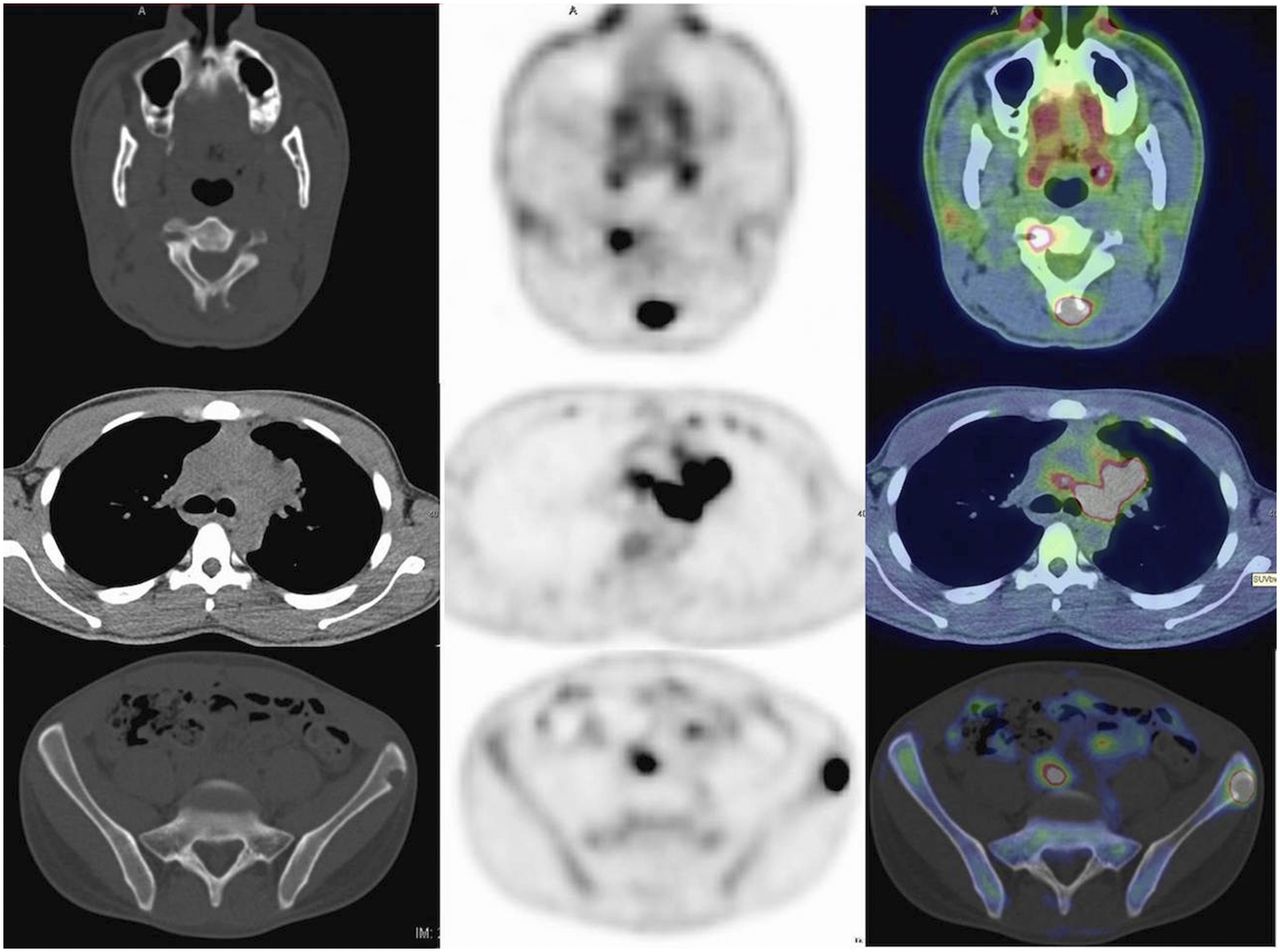
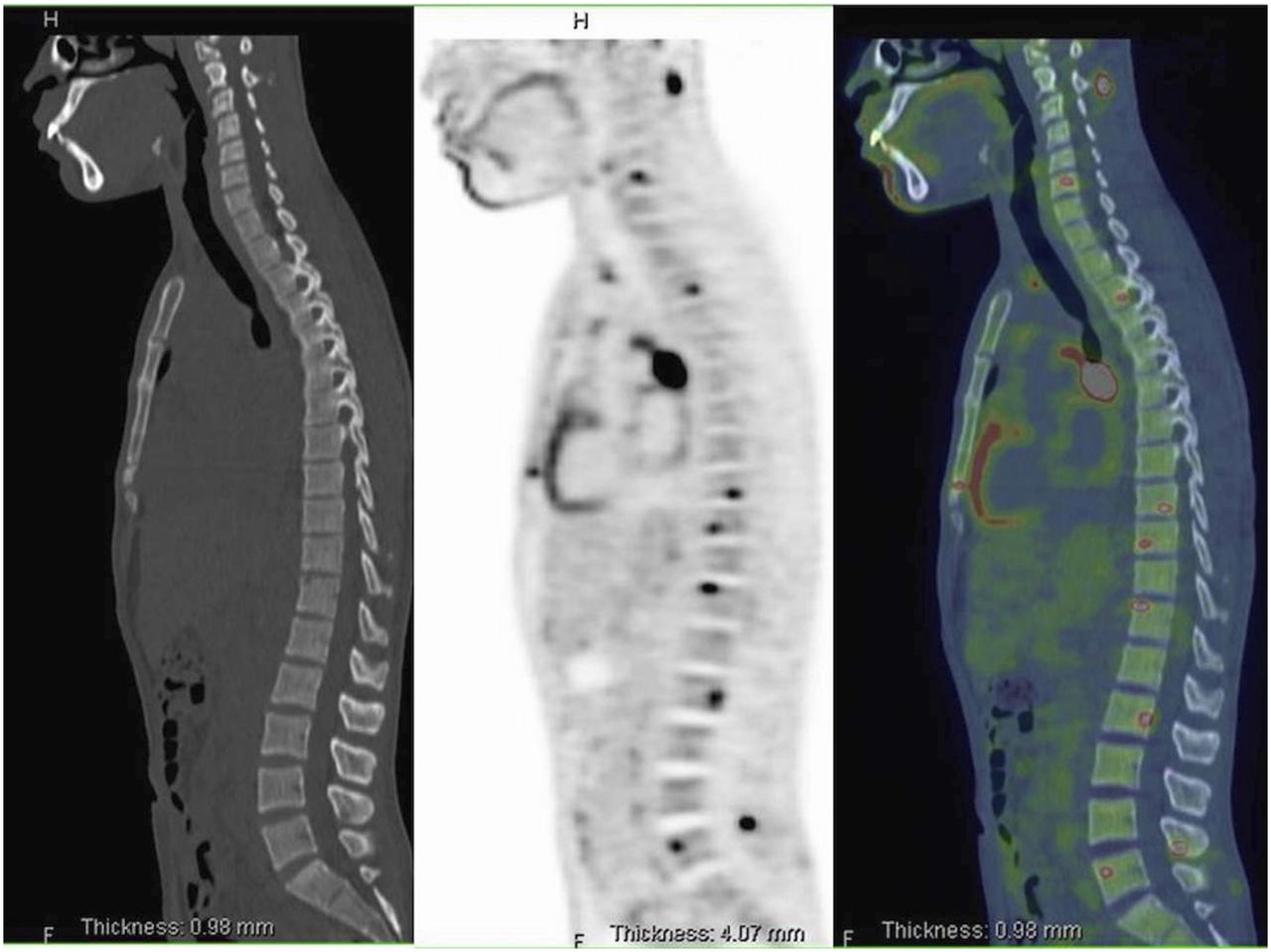
PET/CT was performed to determine disease extent (Figs. 1–3). Pertinent findings included hypermetabolic mediastinal, hilar, and mesenteric/retroperitoneal lymphadenopathy with an SUVmax of 30.8 g/mL; nonhypermetabolic pulmonary nodules; and widespread hypermetabolic osteolytic lesions with an SUVmax of 30.6 g/mL.

Maximum-intensity-projection images demonstrate too numerous to count foci of increased 18F-FDG activity representing disseminated disease.

Axial CT (left), corrected PET (center), and fused PET/CT (right) images through neck (top), mid thorax (center), and pelvis (bottom) demonstrate hypermetabolic mediastinal lymph nodes and lytic posterior C2 and left iliac lesions.
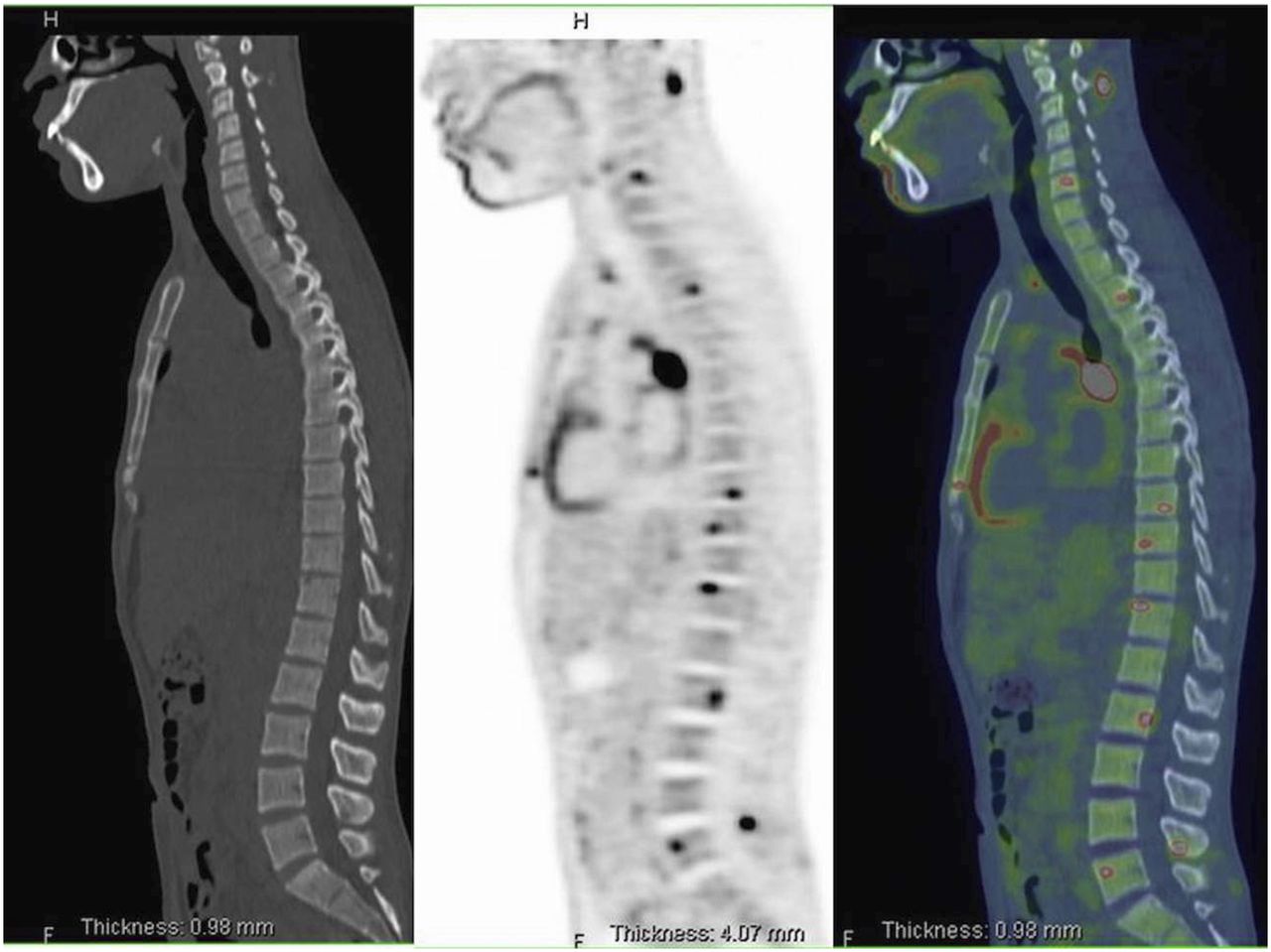
Sagittal CT (left), PET (center), and fused PET/CT (right) images demonstrate disseminated disease scattered throughout vertebral bodies and posterior spinal elements at multiple levels.
He was subsequently treated with a combination of high-dose fluconazole, itraconazole, and amphotericin. He responded well clinically and was discharged home.
DISCUSSION
18F-FDG is a glucose analog positron emitter, whose primary imaging use has traditionally been staging and monitoring of malignancy. Infectious and inflammatory cells, however, also preferentially metabolize glucose (2). PET/CT imaging of infection and inflammation is gaining greater acceptance, to include evaluation of joint prosthesis, fever of unknown origin, AIDS-related disorders, and vascular graft infections (3). Previously, multiple imaging modalities were used to assess infectious and inflammatory disease extent, to include bone scintigraphy, radiography, CT, and MRI (4). Now, whole-body PET/CT can provide a single comprehensive assessment of anatomic and metabolic extent of infection and inflammation involving both the soft tissues and the osseous structures.
Risk factors for disseminated coccidioidomycosis include African-American or Filipino ancestry, immunocompromised state, and male sex (4). The nonspecific symptomatology and indolent nature can lead to delayed diagnosis, with recurrence or spread possible 2 or more years after the initial infection. Fever of unknown origin work-up is then pursued and frequently uses multiple imaging examinations to determine disease extent.
Skeletal involvement of disseminated coccidioidomyocosis predominantly causes osteolytic lesions, which are 18F-FDG–avid on PET/CT. Additionally, soft-tissue assessment with PET/CT can demonstrate clinically occult soft-tissue infection/abscesses, which may need surgical debridement. Thus, 18F-FDG PET/CT can provide whole-body comprehensive assessment of disease extent and guide biopsy targets and therapy (3).
CONCLUSION
Though rare, disseminated coccidioidomycosis is associated with significant morbidity and mortality to include clinically occult abscesses. Previously, a combination of multiple imaging examinations was used to determine disease extent. PET/CT, however, provides whole-body metabolic and anatomic assessment of disease and should be considered a first-line imaging examination in these patients.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Apr. 21, 2016.
- Received for publication November 25, 2015.
- Accepted for publication February 29, 2016.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.