


Abstract
Primary hyperparathyroidism is predominantly caused by a single parathyroid adenoma. Knowledge of normal and ectopic locations of parathyroid glands is crucial to help guide surgeons who plan targeted unilateral parathyroidectomy to reduce surgical time and risk. We describe a female patient with clinical primary hyperparathyroidism who underwent a failed initial parathyroidectomy, with subsequent imaging localizing an ectopic parathyroid adenoma in the carotid sheath.
Given that ectopic parathyroid glands are not uncommon in the setting of primary hyperparathyroidism, preoperative localization is critical to the current minimally invasive approaches toward surgical excision. Knowledge of ectopic locations and appropriate imaging guidelines is imperative.
CASE REPORT
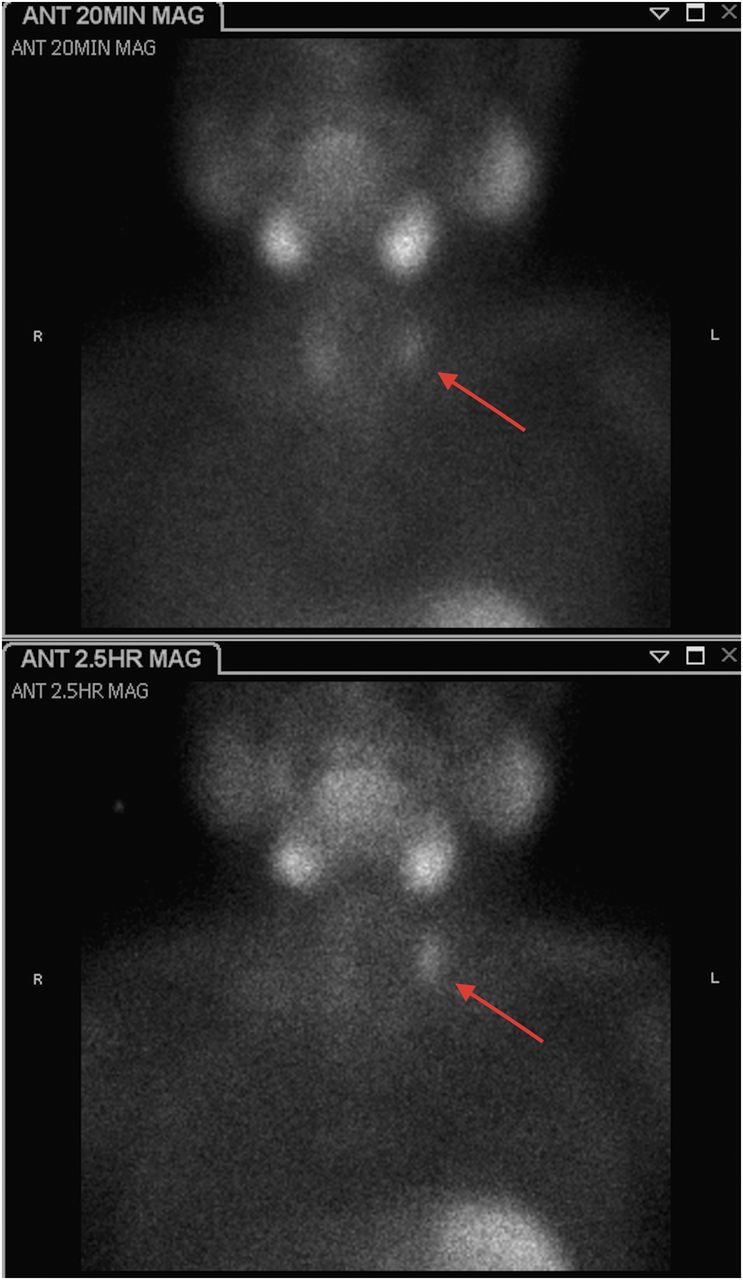
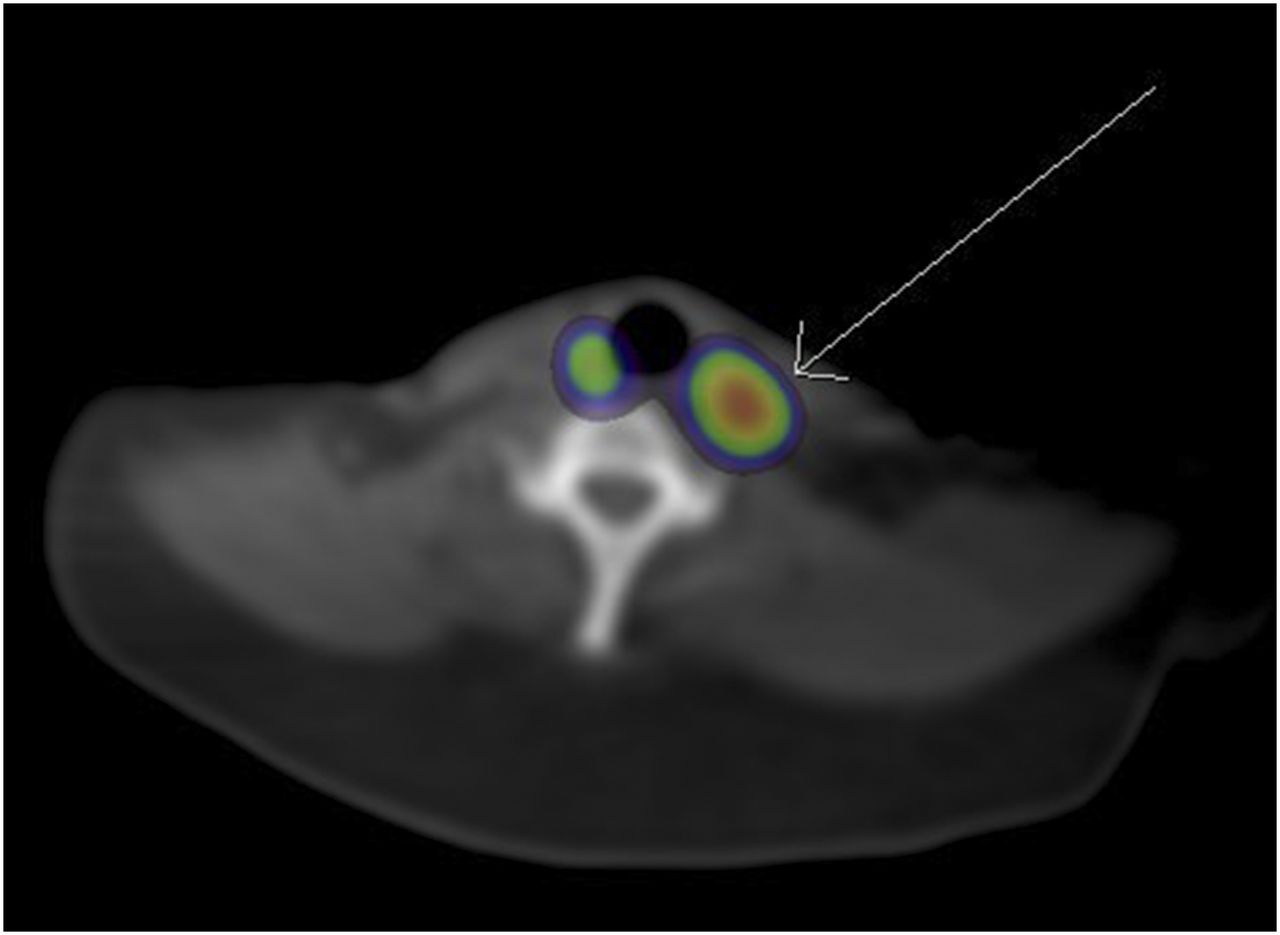
Our patient was clinically diagnosed with primary hyperparathyroidism after a workup for incidental hypercalcemia. Dual-phase 99mTc-sestamibi scintigraphy with early SPECT/CT demonstrated uptake posterior and lateral to the superior left thyroid (Figs. 1 and 2). The findings of neck ultrasound were unremarkable.
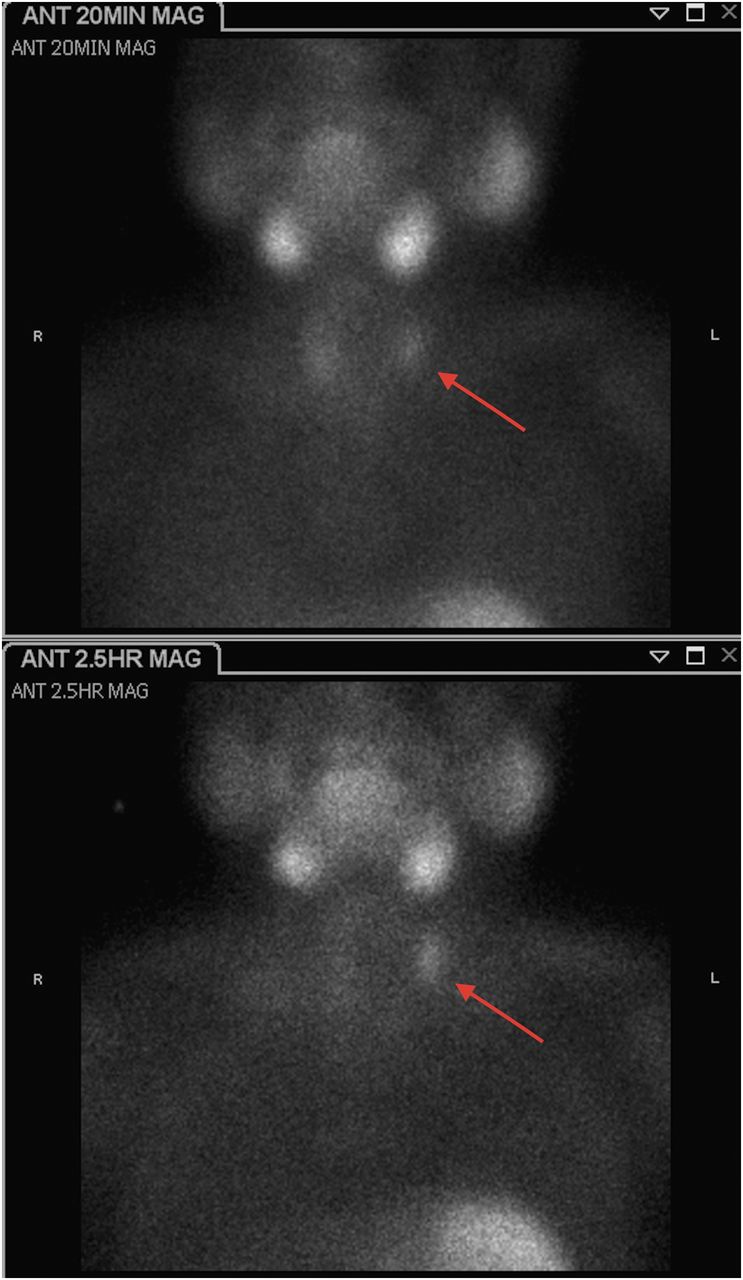
Anterior 20-min (top) and 2.5-h (bottom) 99mTc-sestamibi images demonstrate persistent focal uptake in left neck. MAG = magnified.
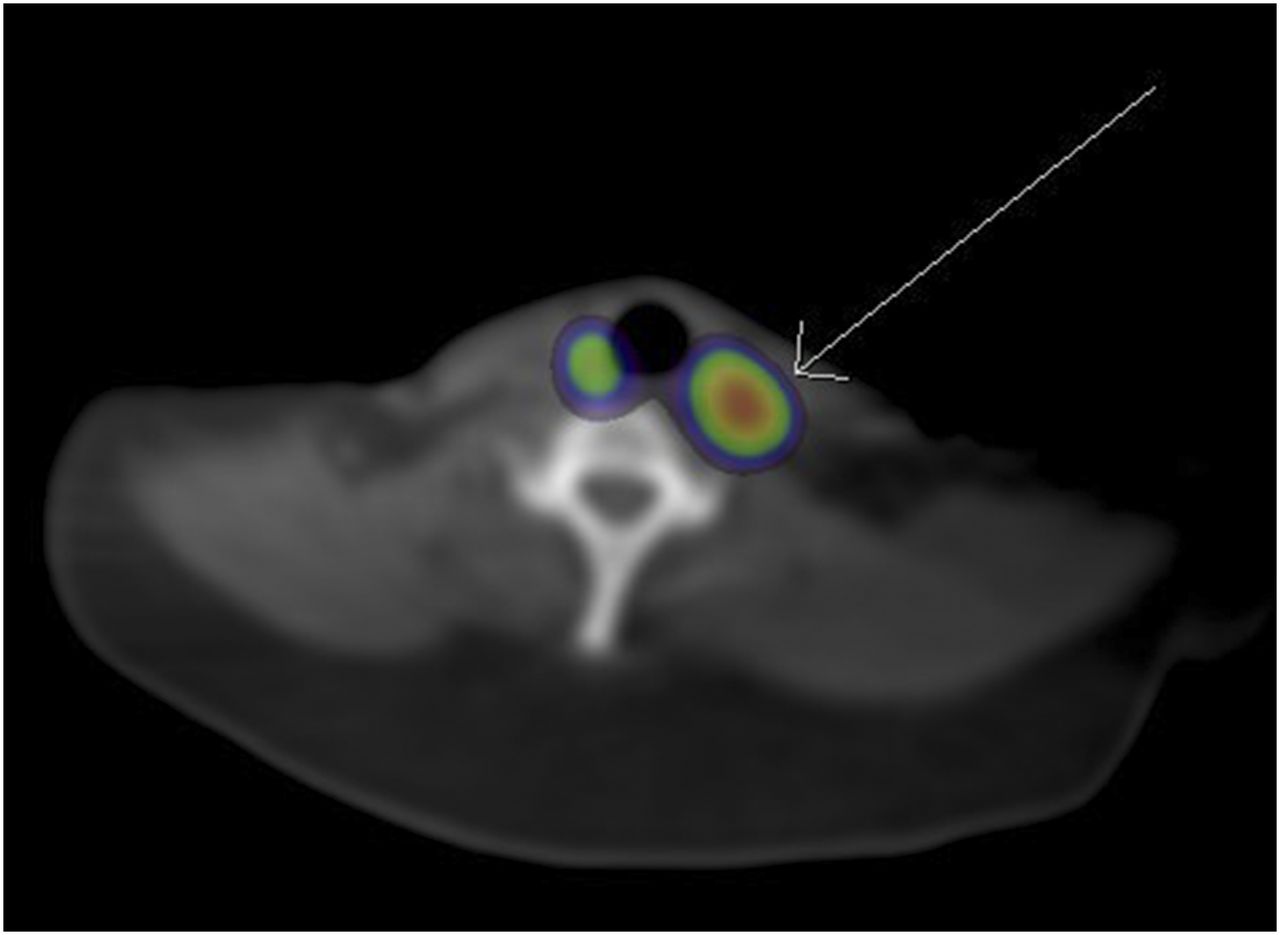
SPECT/CT data localize uptake posterior and lateral to superior left thyroid gland.
Excision of the left superior parathyroid gland led to no change in intraoperative parathyroid levels. The surgeon proceeded with left hemithyroidectomy and bilateral explorative dissection, with no abnormal tissue found on pathologic examination.
Postoperative MRI did not prospectively identify a parathyroid adenoma. Repeated dual-phase parathyroid scintigraphy confirmed persistence of the adenoma. Repeated SPECT coregistered with dedicated neck CT localized the adenoma to the left carotid sheath (Figs. 3 and 4).
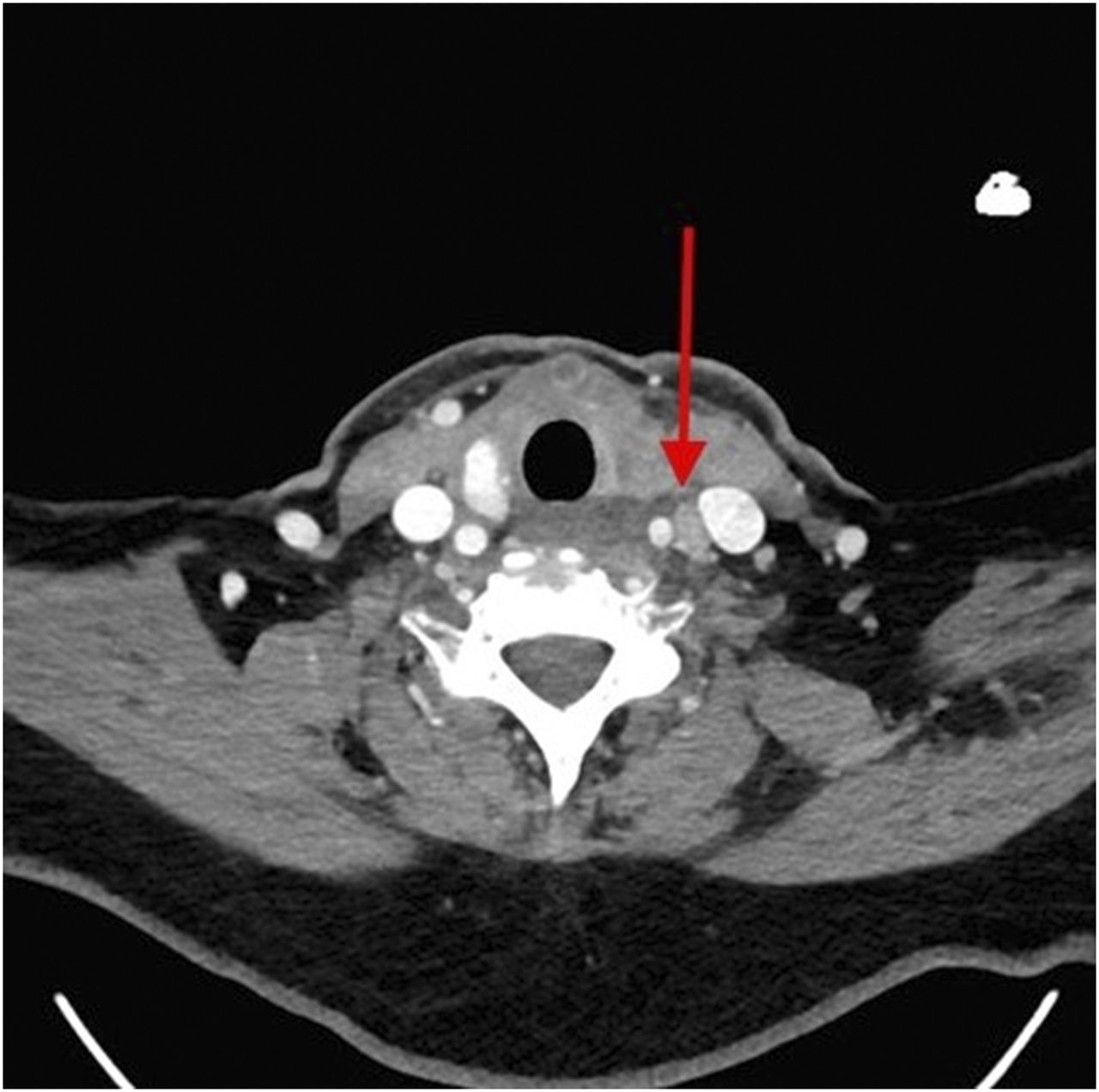
Contrast-enhanced CT demonstrates soft-tissue lesion in left carotid sheath.
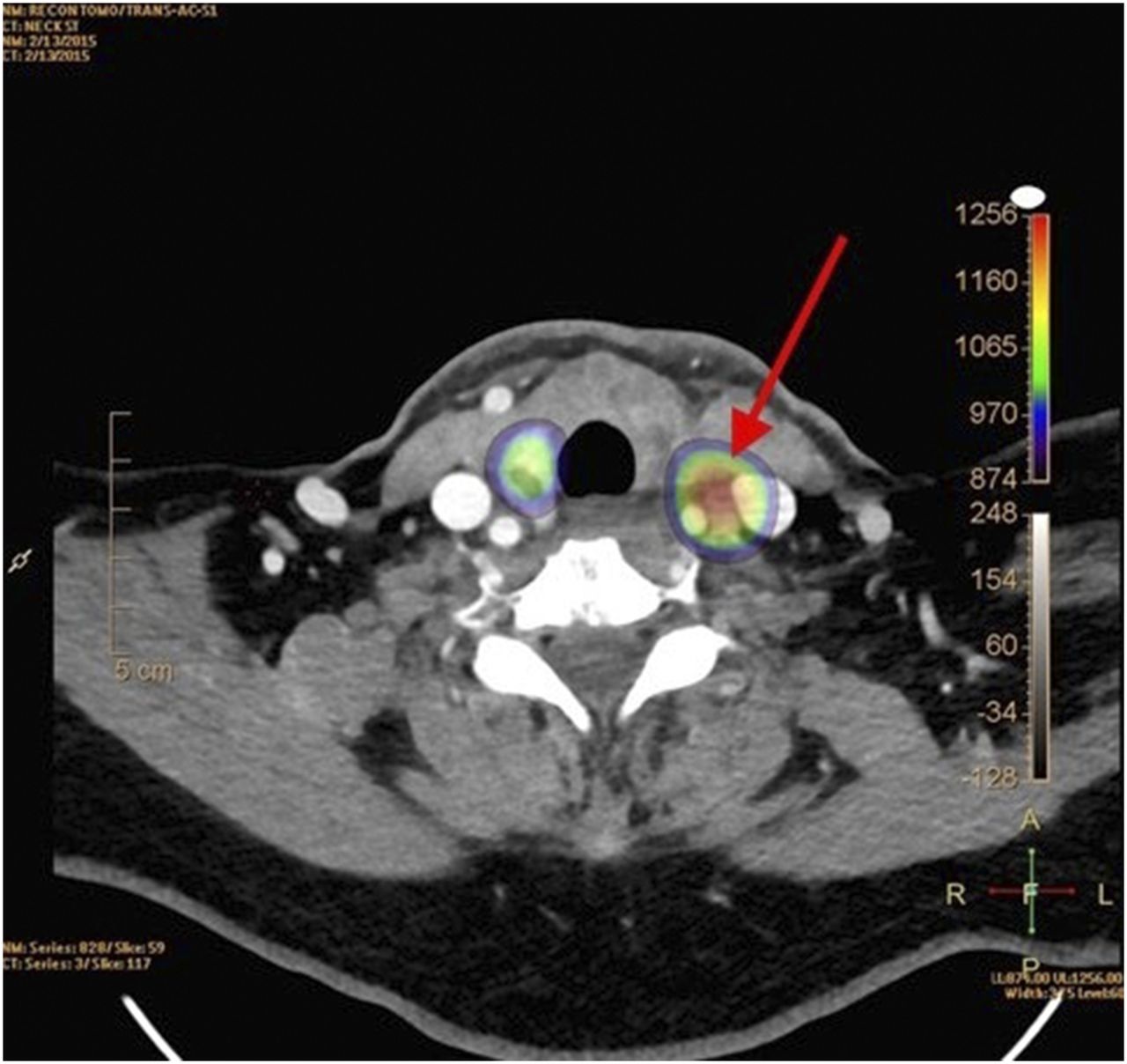
Fused SPECT/high-resolution CT localizes uptake to soft-tissue lesion in left carotid sheath.
Repeated surgery removed a pathology-proven parathyroid adenoma from the left carotid sheath.
DISCUSSION
Primary hyperparathyroidism is a clinical diagnosis based primarily on laboratory results, usually in the fifth to seventh decades of life (1). Hypercalcemia, the primary clinical abnormality, can present with numerous symptoms, including bone or abdominal pain, nephrolithiasis, and psychiatric imbalances (1). Etiologies include a single parathyroid adenoma, multiglandular hyperplasia, multiple adenomas, and, rarely, parathyroid carcinomas (1). Surgical excision of abnormal parathyroid tissue is usually curative. Historically, bilateral cervical dissection has been performed with 95% success (1). Preoperative imaging localization, however, allows for focused surgeries, reducing procedure length and risk (2).
Usually, 2 superior and 2 inferior parathyroid glands are immediately posterior to the thyroid. Ectopic parathyroid glands exist in numerous locations between mouth and diaphragm, with a frequency of 6%–16% (3). Ectopia in the carotid sheath, as occurred in our patient, is reported in less than 1% of cases (2).
Our institution performs a dual-phase 99mTc-sestamibi protocol, with planar images obtained at 20 and 150 min, plus SPECT/CT at 20 min for improved localization (4). The initial examination was limited by the reduced spatial resolution of the coregistered low-dose cone-beam CT scan; subsequent coregistration with high-resolution CT proved invaluable. Four-dimensional CT, along with ultrasound and MRI, can also improve preoperative localization (5).
CONCLUSION
Because focused unilateral parathyroidectomy is curative in most cases of primary hyperparathyroidism, with less surgical time and risk than nontargeted surgery, preoperative localization is crucial. Frequently, the clinical question focuses on whether there is an adenoma—a question readily answered with planar scintigraphy alone. However, the better anatomic localization and spatial resolution provided by advanced imaging is extremely helpful. The initial surgical failure in this case may have been prevented if the initial CT scan had been of higher resolution or if ectopia had been suspected because of the location of the parathyroid adenoma—posterior and lateral to the thyroid.
DISCLOSURE
No potential conflict of interest relevant to this article was reported. The views expressed in this paper are those of the authors and do not reflect the official position of the U.S. Government, the Department of Defense, or the Department of the Air Force.
Footnotes
Published online Feb. 4, 2016.
REFERENCES
- Received for publication December 8, 2015.
- Accepted for publication January 27, 2016.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.