


Abstract
On brain perfusion SPECT, a primary brain lesion presents as a localized defect that corresponds to the mass lesion. 99mTc-HMPAO images generally show a focal defect in the region of abnormality, whether containing necrotic tissue, recurrent tumor, or both. Further characterization with MR imaging is needed to confirm the diagnosis, as demonstrated in this case report.
We report a case of meningioma suspected on 99mTc-hexamethylpropyleneamine oxime (HMPAO) brain SPECT. Few cases of meningioma appear on SPECT scans. Brain SPECT may provide complementary information for the diagnosis of brain tumors.
CASE REPORT
A 34-y-old woman diagnosed with Lyme disease 15 y previously presented with a 2-month history of chronic headaches, tremor, numbness, and adenopathy. Blood biochemistry was within normal limits. A 99mTc-HMPAO SPECT brain scan was performed because of suspected Lyme neuroborreliosis. The patient was injected with 1,073 MBq (29 mCi) of 99mTc-HMPAO, and SPECT images of the brain were subsequently obtained.
DISCUSSION
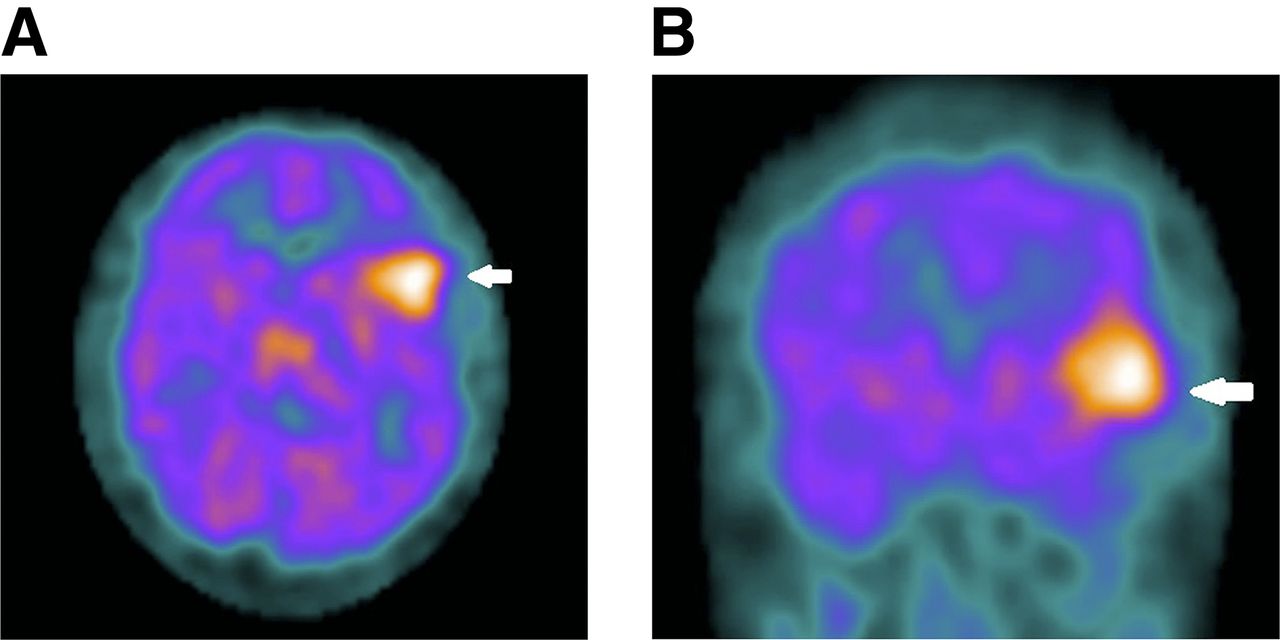
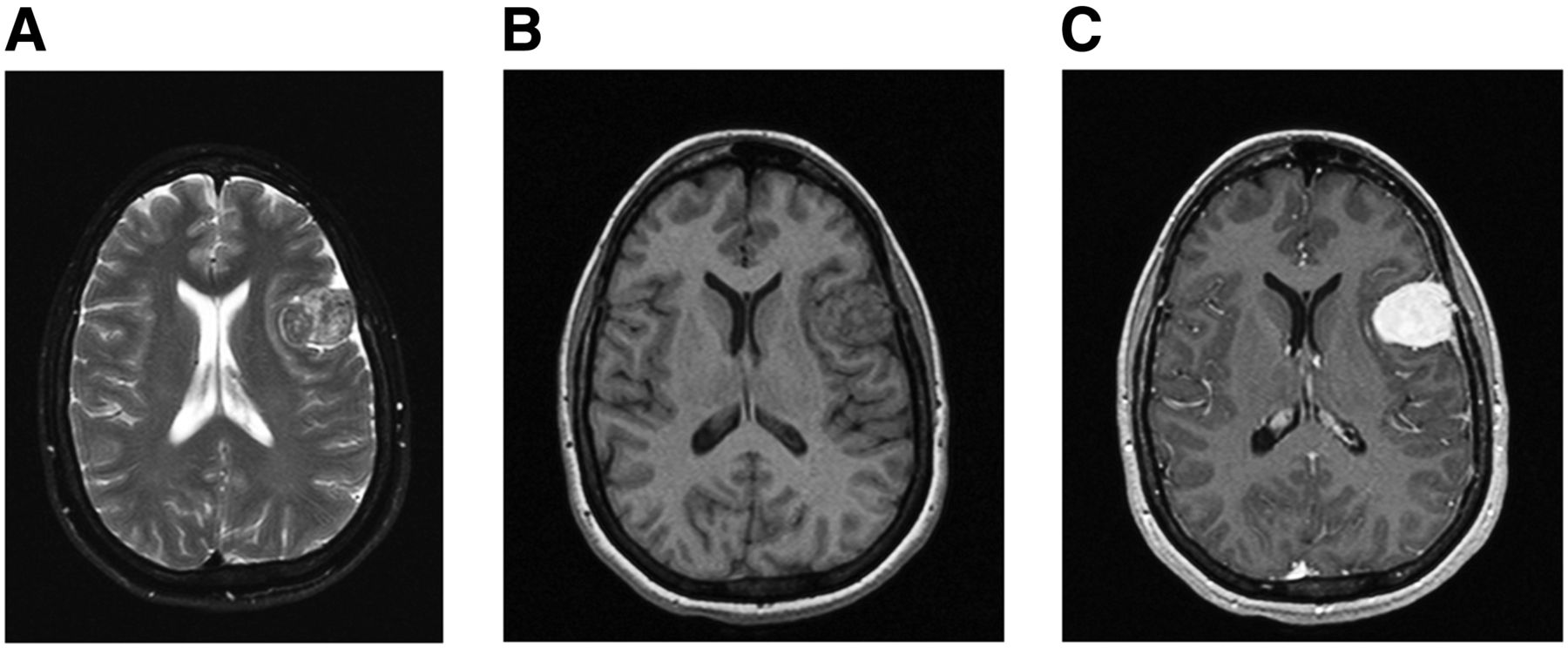
The SPECT images showed a large focus of radiotracer uptake in the left frontotemporoparietal region (Fig. 1). A differential diagnosis of infection, seizure focus, and neoplasm was given, with high suspicion of meningioma. MR imaging of the brain was subsequently performed and demonstrated a solid, enhancing extraaxial mass in the same area, with an appearance consistent with meningioma (Fig. 2).

SPECT images of brain obtained with 99mTc-HMPAO show intense focal radiotracer uptake in left frontal area (arrows) on representative axial (A) and coronal (B) slices.
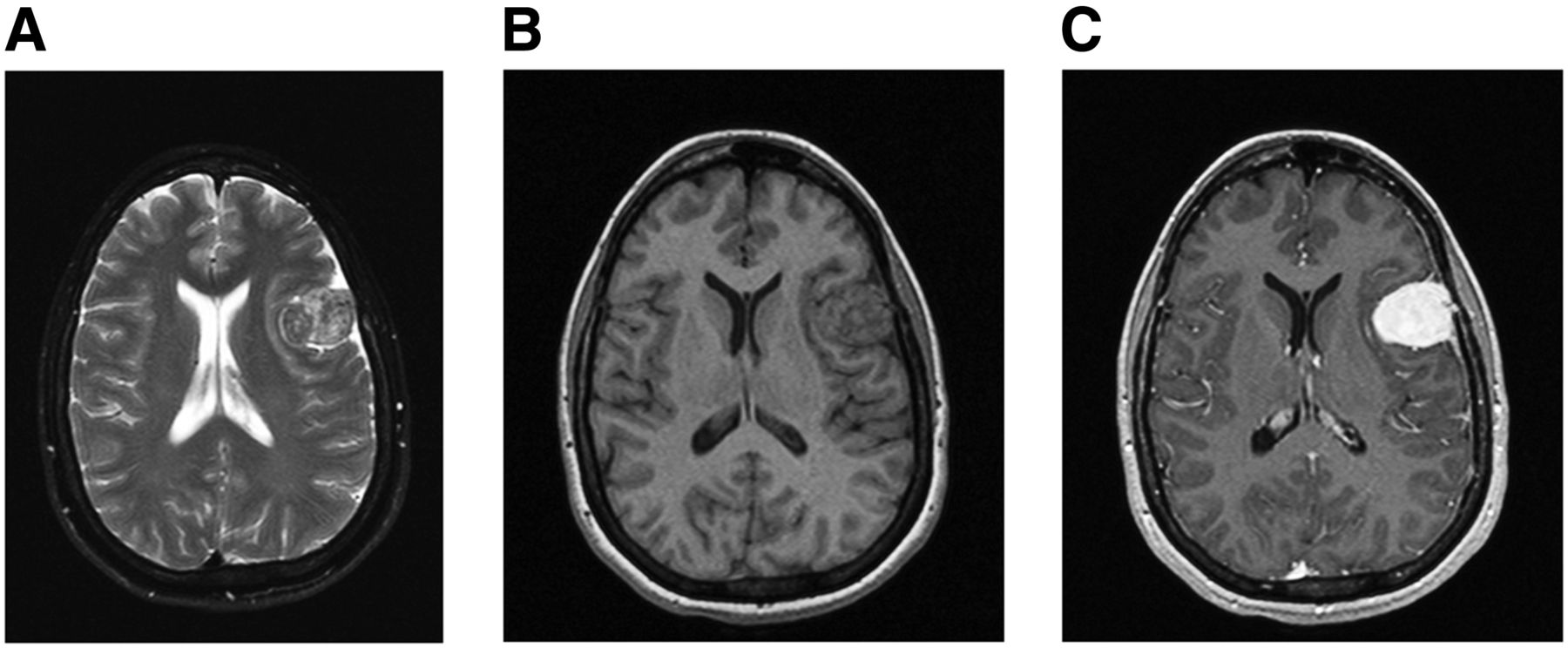
Axial T2-weighted (A) and axial unenhanced (B) and enhanced (C) T1-weighted MR images demonstrate solid 3.2 × 3.5 cm enhancing extraaxial mass with enhancing dural tail overlying left frontal lobe.
99mTc-HMPAO is a lipophilic compound that passes the intact blood–brain barrier freely (1,2). It can be labeled with 99mTc to assess high-flow lesions (1,2). Meningiomas typically present with high radiotracer uptake on 99mTc-HMPAO SPECT (1,2). Conversely, in patients with calcified meningioma there will be decreased radiotracer uptake (2). Patients with stroke also can have decreased to absent 99mTc-HMPAO uptake. Findings are time-dependent and have the highest prognostic value during the first 48 h after a stroke; strokes due to occlusion of a major cerebral artery produce focal absence of perfusion, and a normal brain perfusion result on SPECT during the first 6 h after a stroke implies minor or lacunar stroke (3). There are some reports of brain tumors with increased 99mTc-HMPAO accumulation other than meningioma, such as glioblastoma multiform, pituitary adenoma, high-grade astrocytoma, and multiple myeloma (1). Shih et al. showed cases of meningiomas without 99mTc-HMPAO uptake, possibly explained by a skull defect due to previous craniotomy, replacement of normal brain tissue by tumor, or functioning arteriovenous shunting due to tumor vascular blush, as demonstrated on cerebral angiograms (4). Further characterization with MR imaging was necessary to confirm the diagnosis.
MR images demonstrated a solid, 3.2 × 3.5 cm enhancing extraaxial mass with an enhancing dural tail overlying the left frontal lobe. Meningioma typically appears isointense to hypointense to gray matter on T1-weighted images and isointense to hyperintense on T2-weighted images (5). A dural tail is a nonspecific finding that often suggests meningioma but can be seen with other tumors. Meningiomas can also be associated with mass effect and cerebral edema (6). Our findings were most consistent with the diagnosis of meningioma.
CONCLUSION
On SPECT brain perfusion imaging, a primary brain lesion presents as a localized defect that corresponds to the mass lesion. 99mTc-HMPAO images generally show a focal defect in the region of abnormality, whether containing necrotic tissue, recurrent tumor, or both. Further characterization with MR imaging is needed to confirm the diagnosis.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Oct. 15, 2015.
REFERENCES
- Received for publication July 2, 2015.
- Accepted for publication September 10, 2015.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.