


Article Figures & Data
Figures
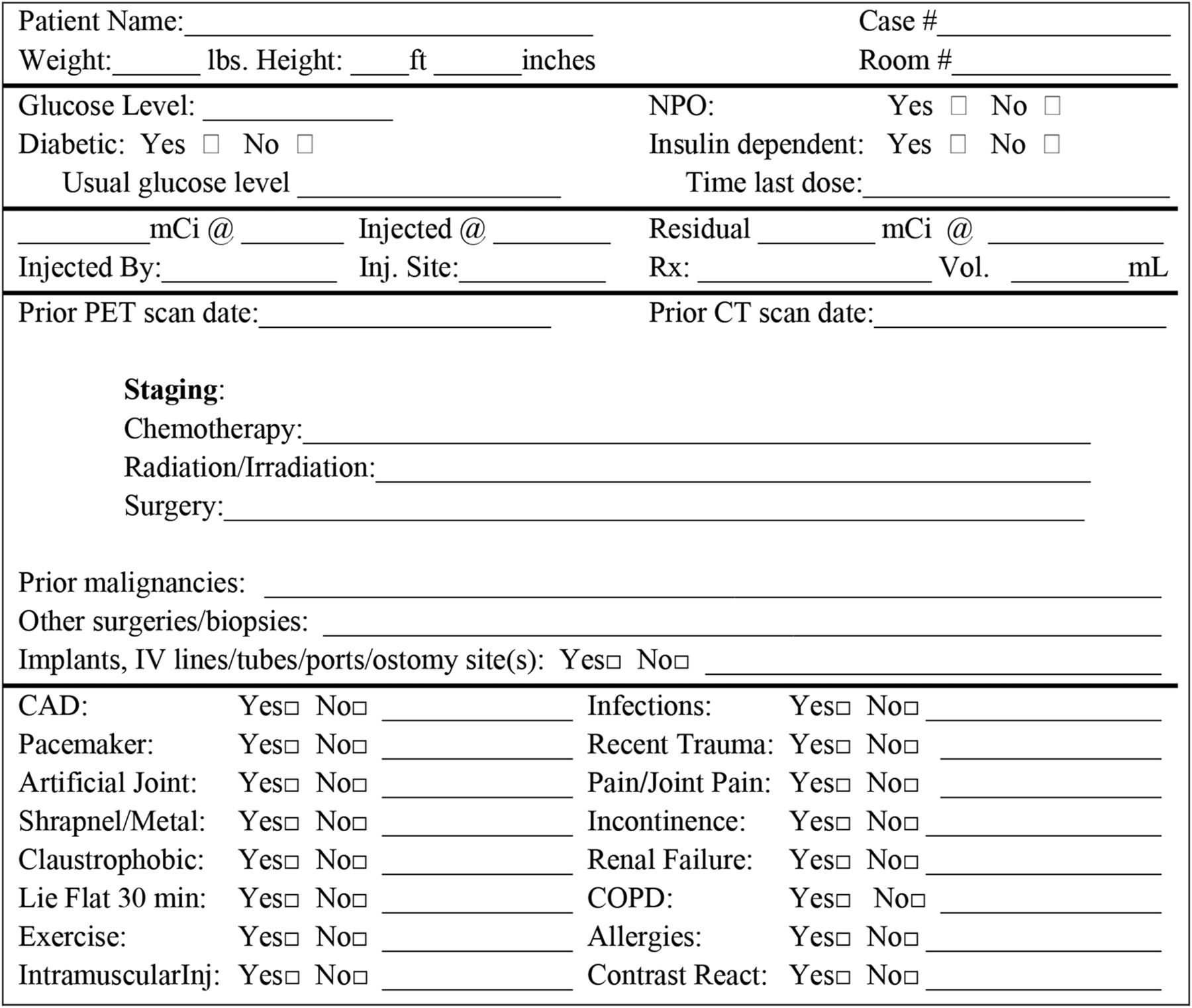
- FIGURE 1.
Scheduling interview.
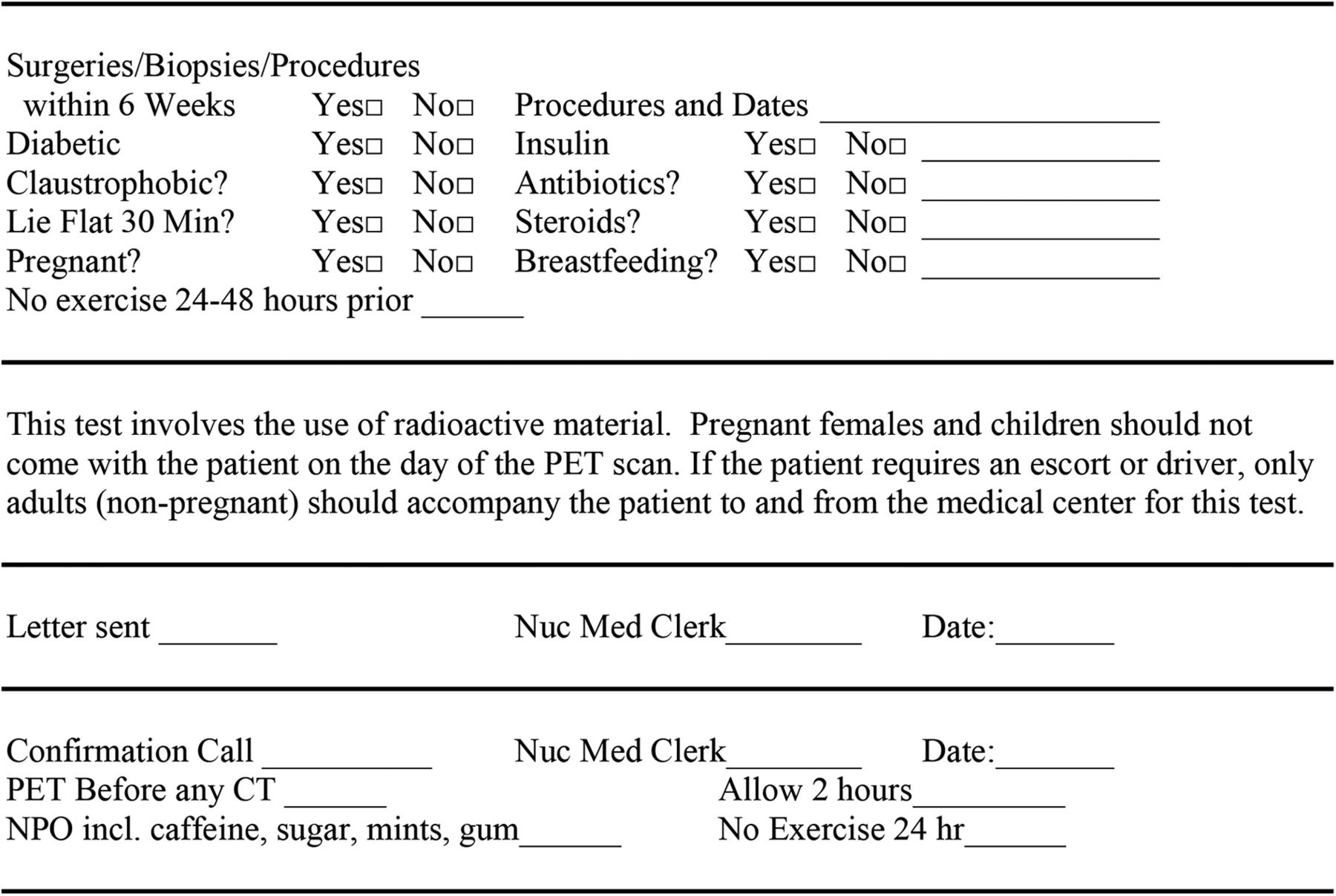
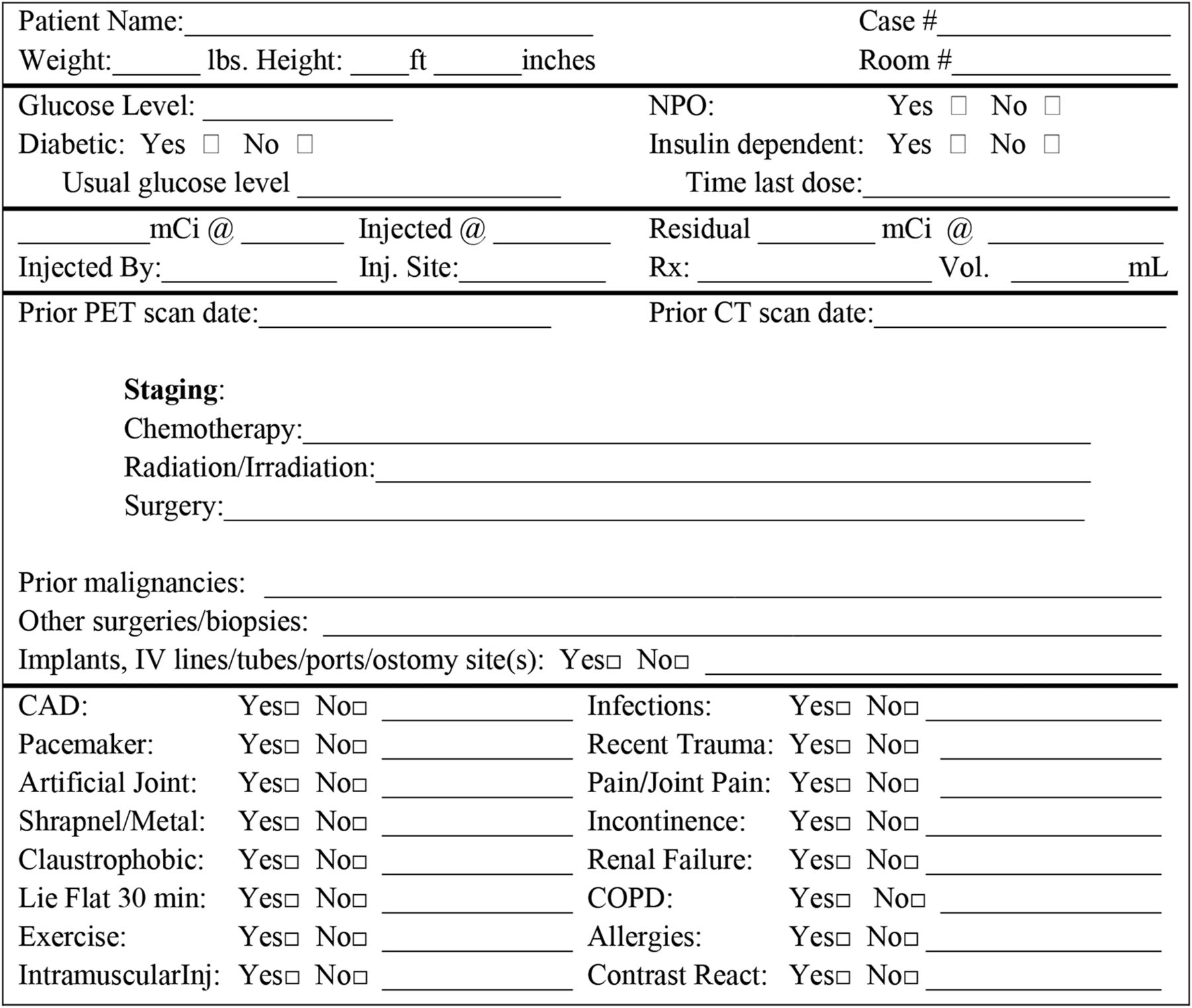
- FIGURE 2.
Preinjection interview.
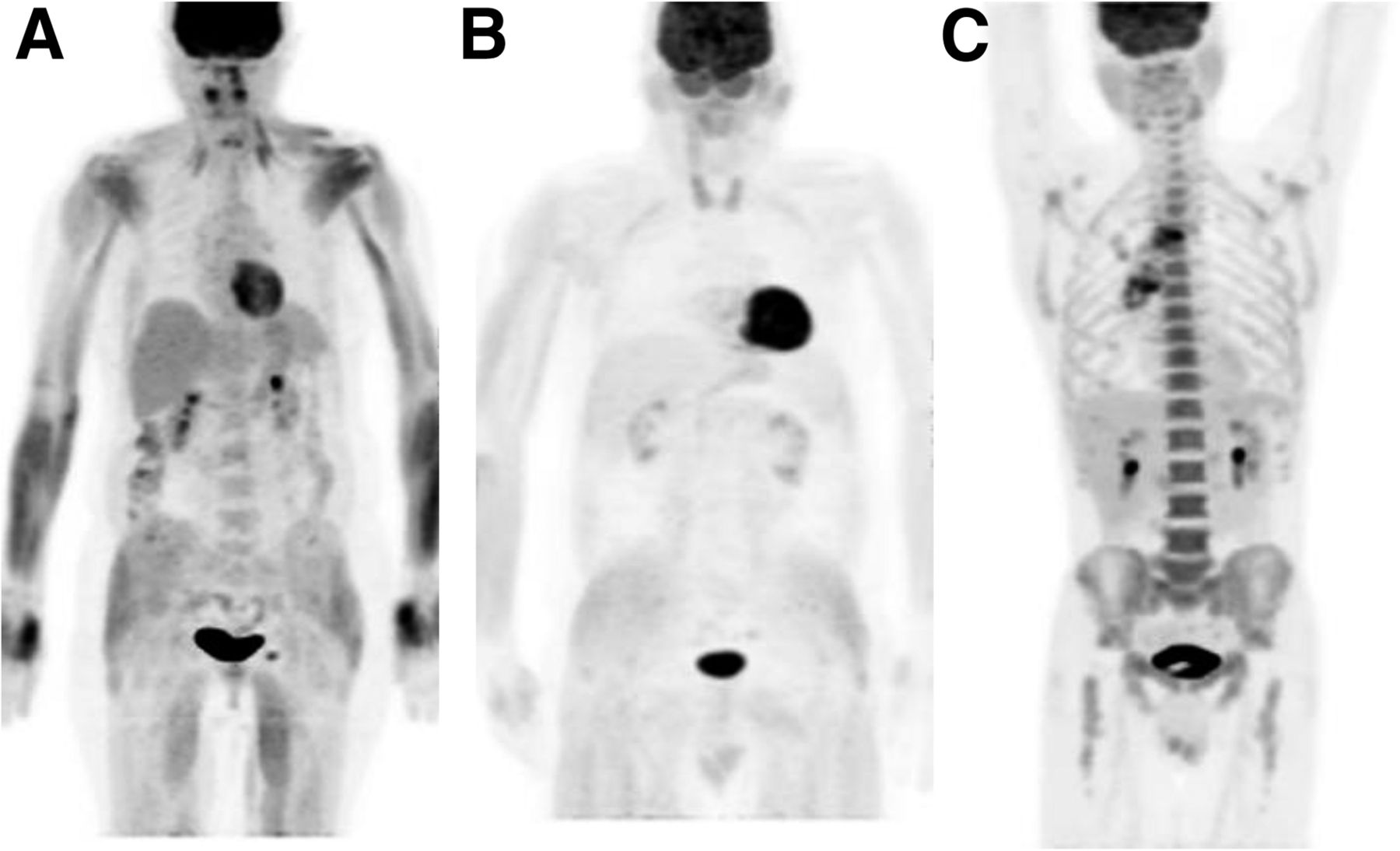
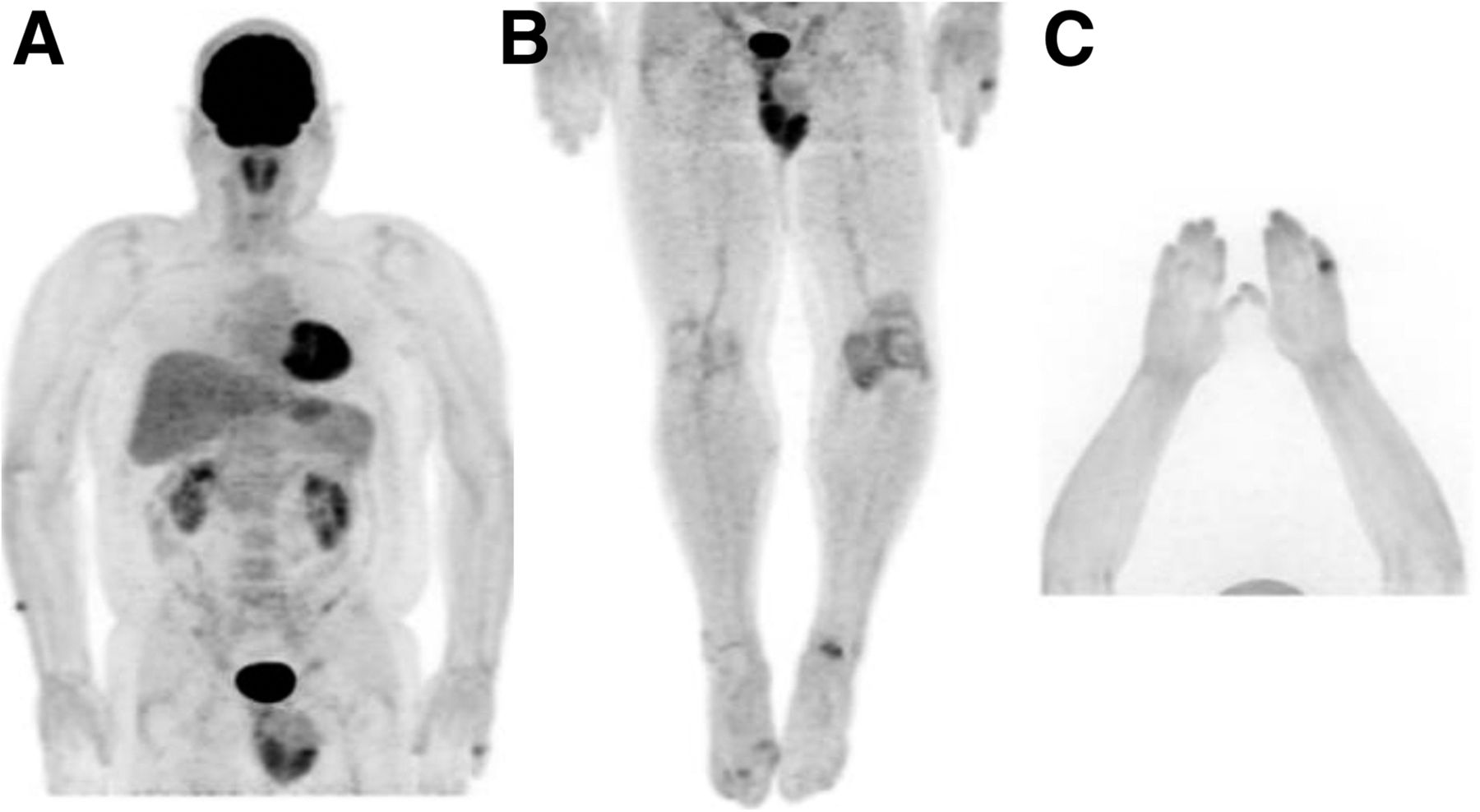
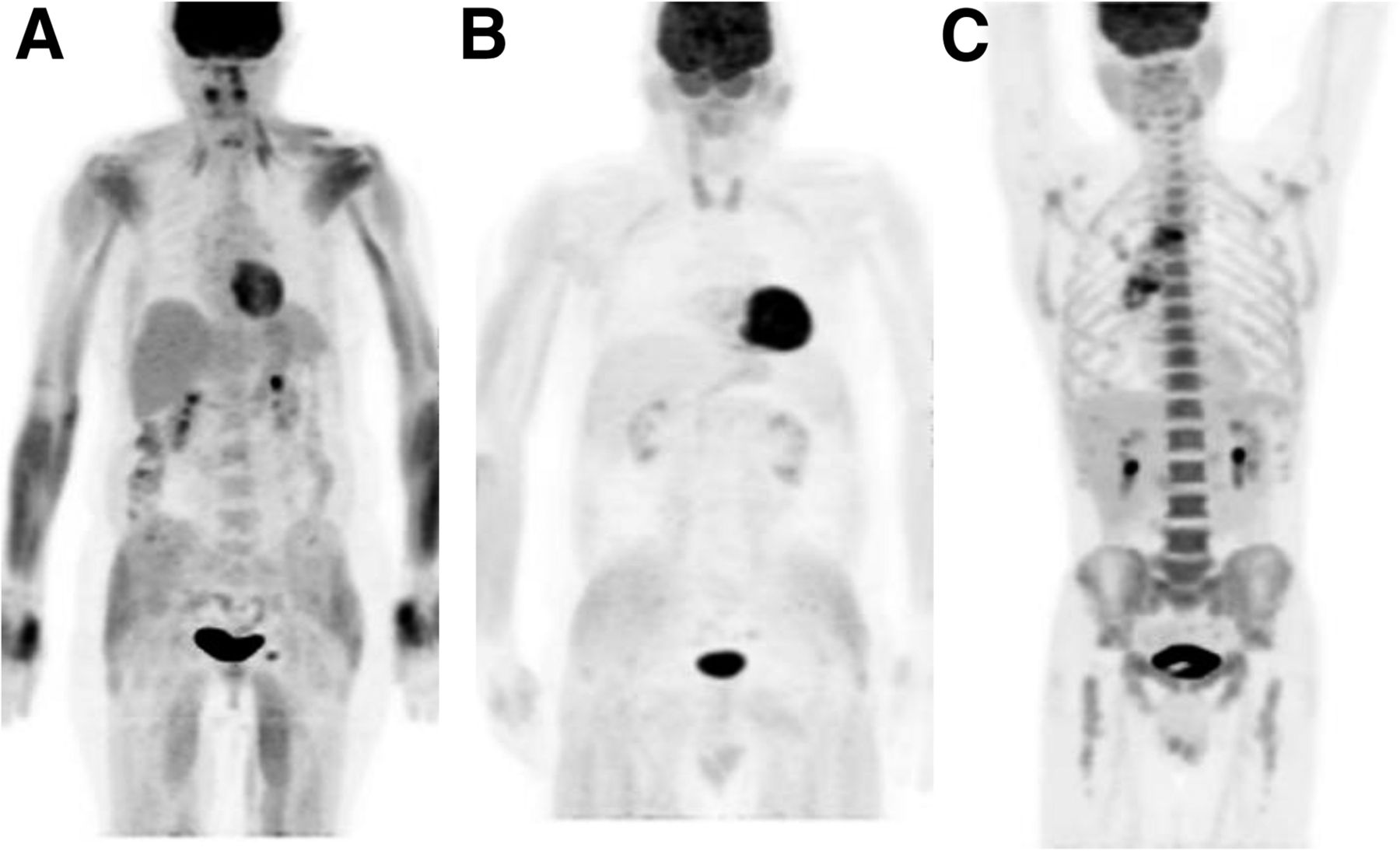
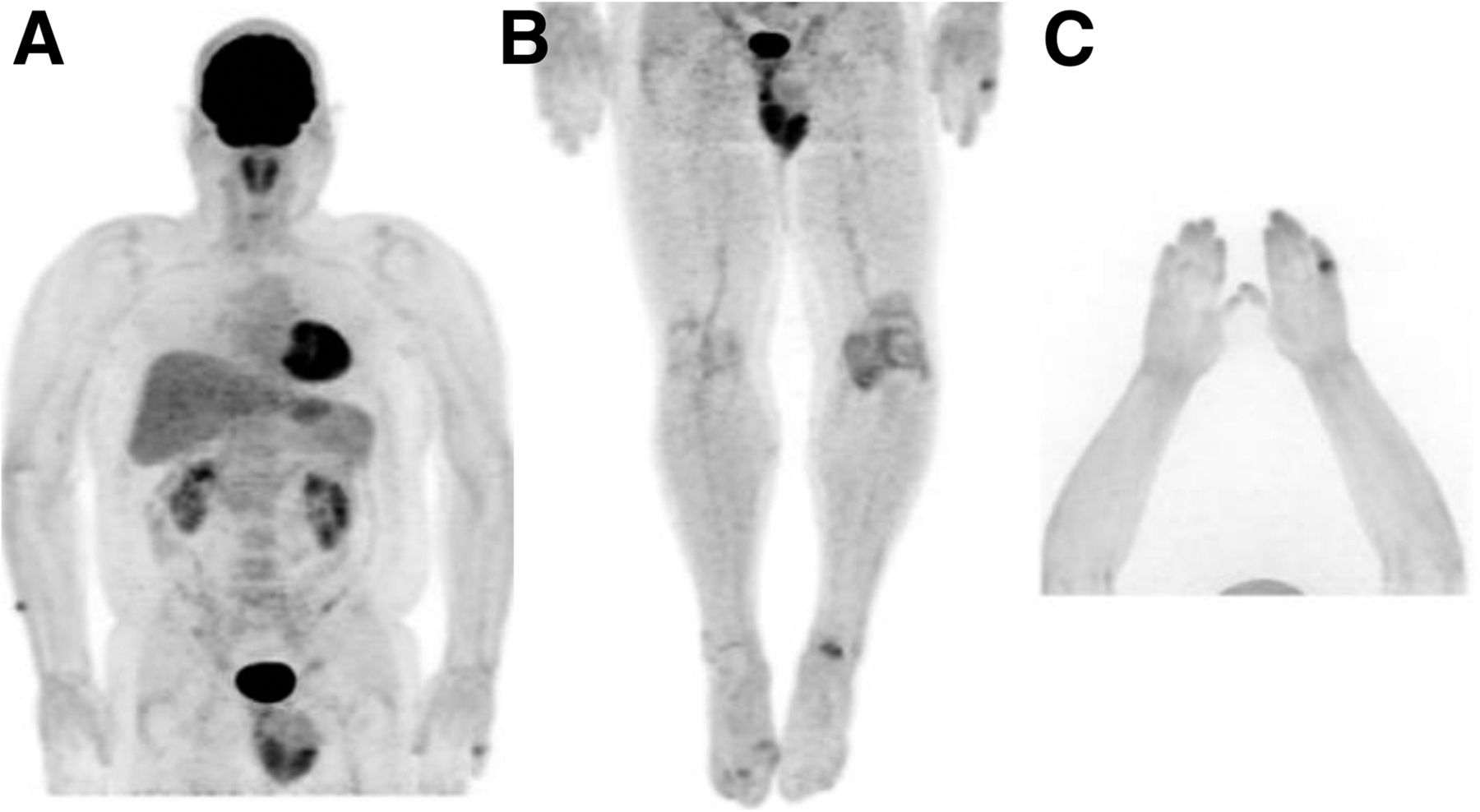
- FIGURE 3.
Maximum-intensity-pixel 18F-FDG PET images of patient who exercised strenuously 24 h before the scan (A), patient who took insulin the morning of the scan (B), and patient who was receiving granulocyte-colony-stimulating factor (C).
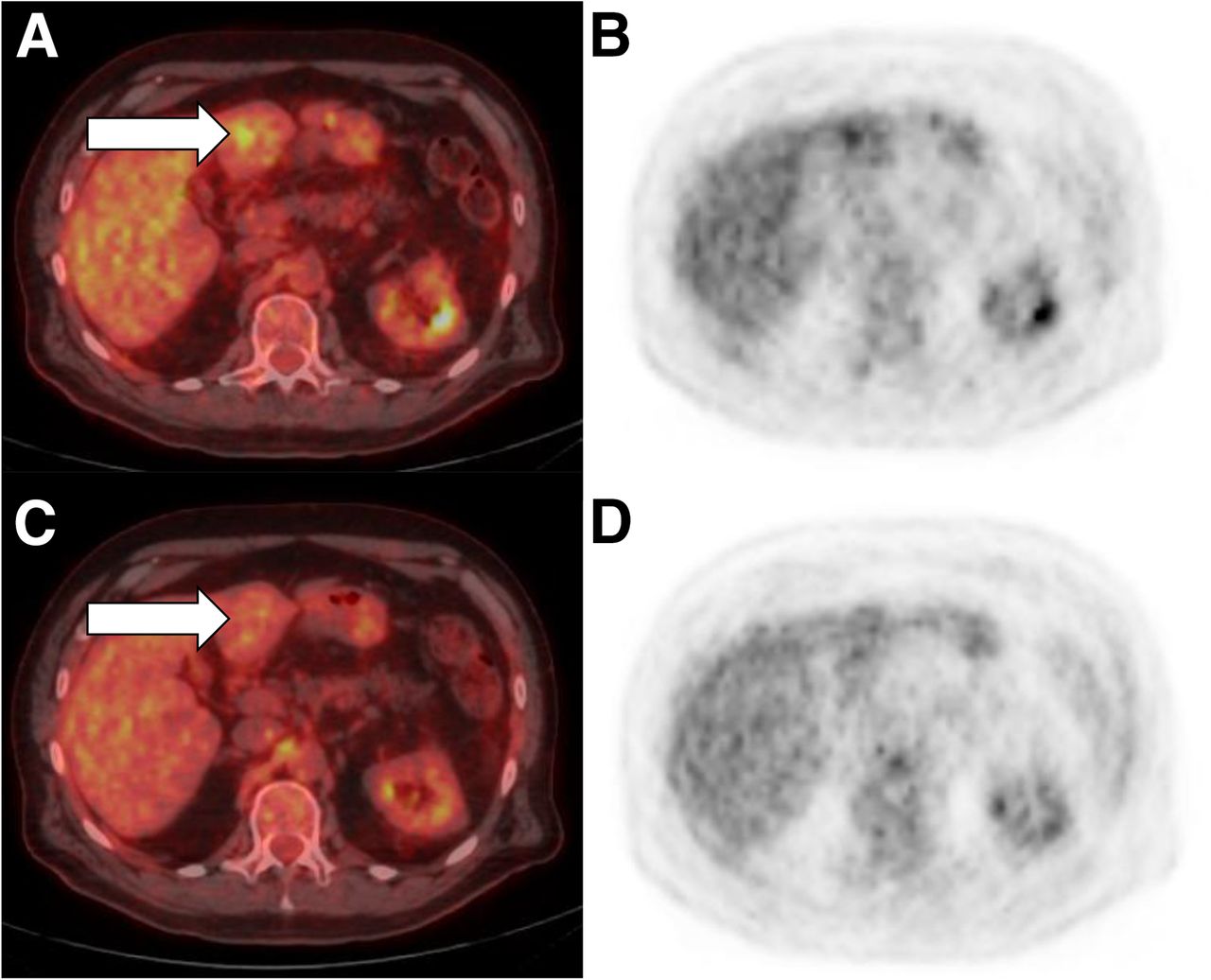
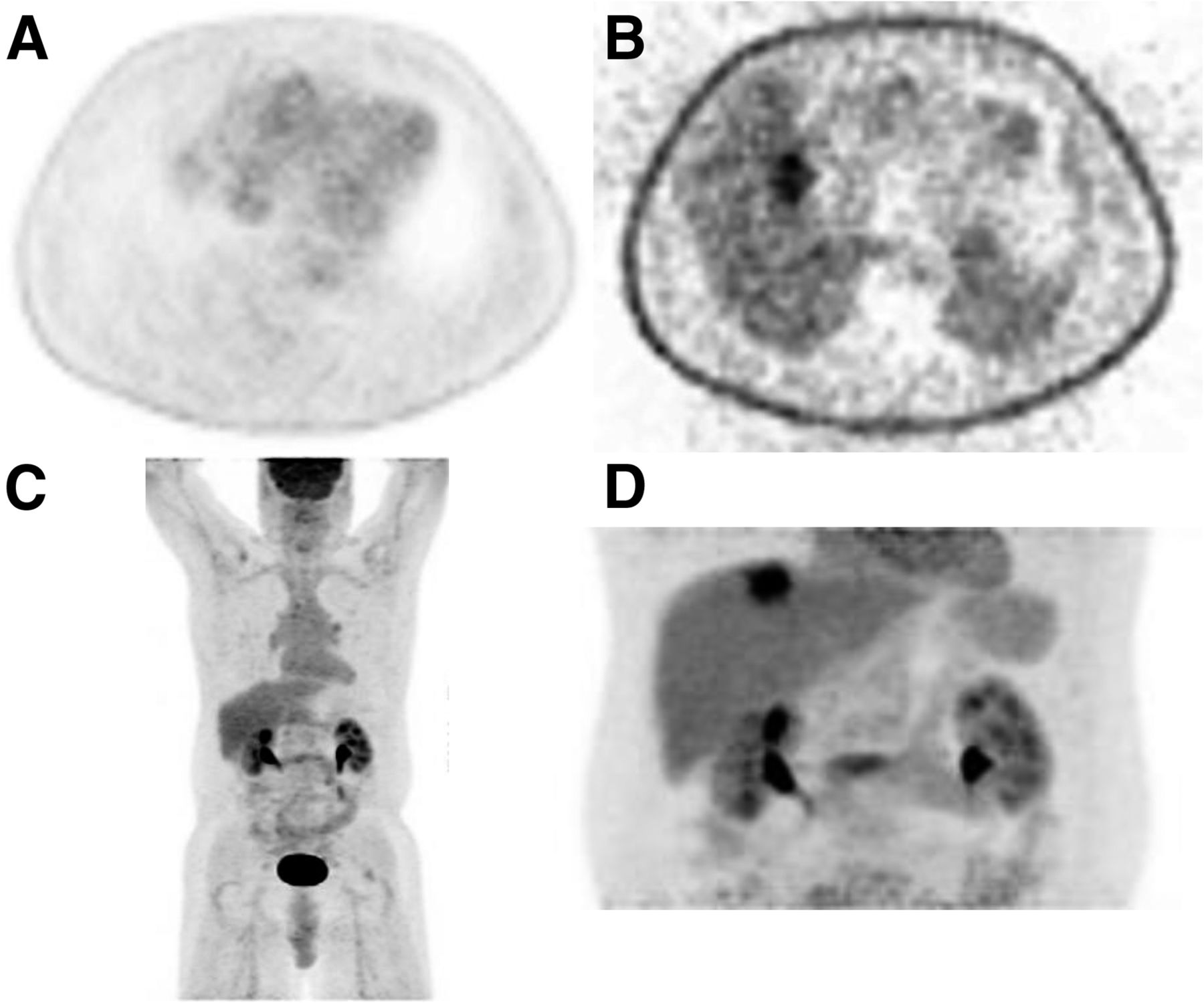
- FIGURE 4.
False-negative findings on attenuated-corrected axial image (A), non–attenuation-corrected axial image (B), maximum-intensity-pixel image (C), and maximum-intensity-pixel additional limited image with increased time to allow for more counts (D).
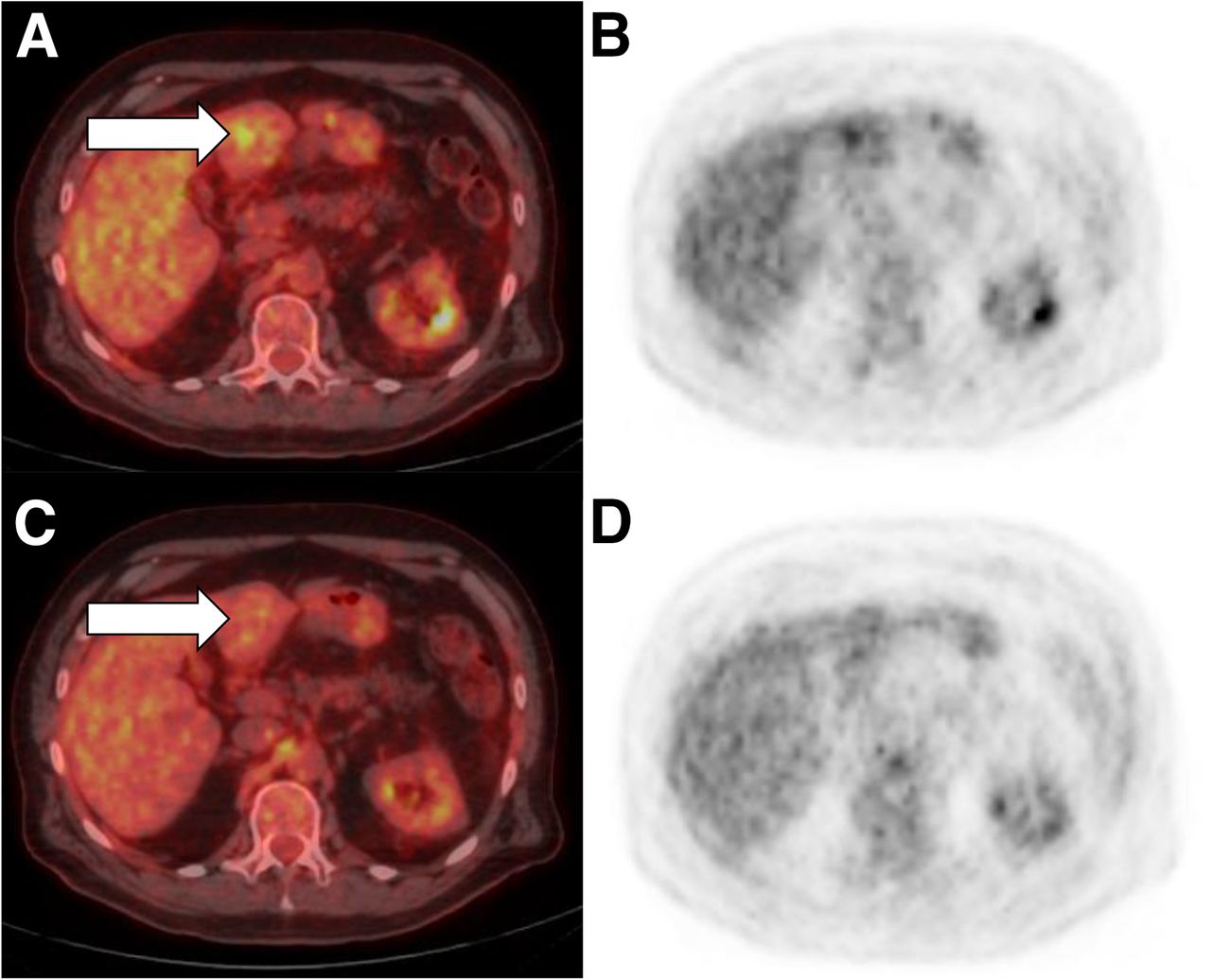
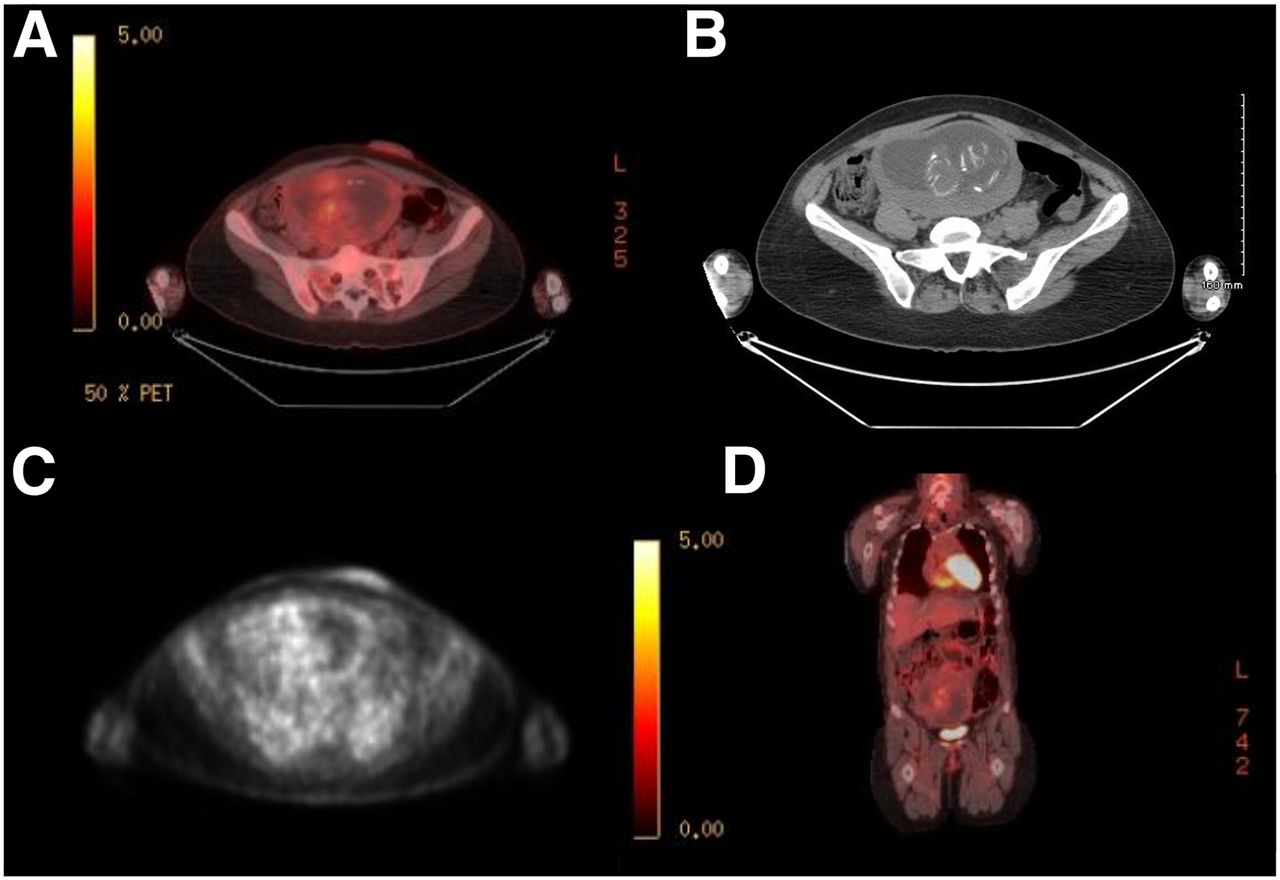
- FIGURE 5.
False-positive findings on fused axial image (A) and attenuation-corrected axial image (B). Additional limited scan was performed with delay to allow for clearance and for more counts on fused axial image (C) and attenuation-corrected axial image (D).
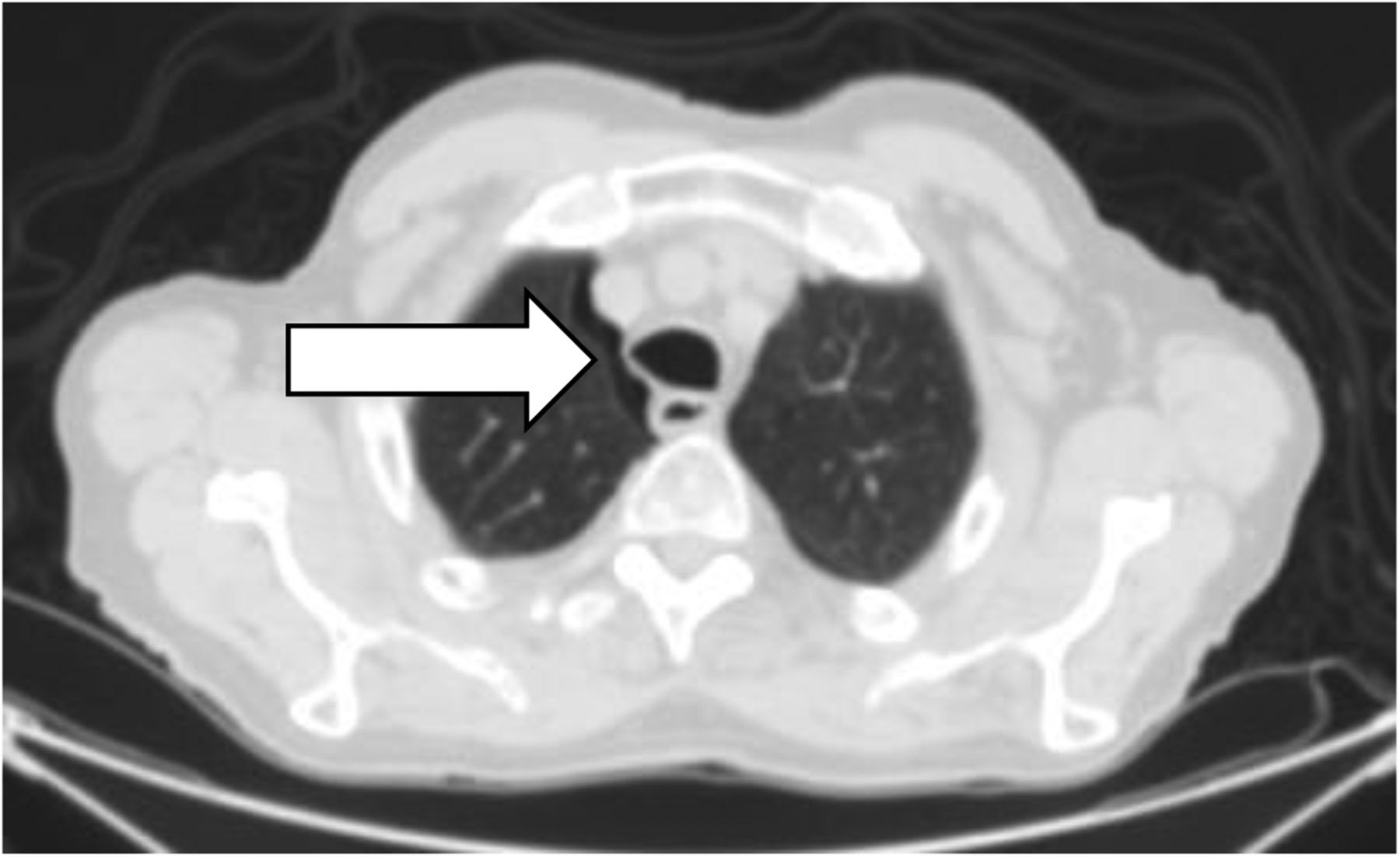
- FIGURE 6.
Pneumothorax on axial CT image displayed in lung window 1,500 and level −550.
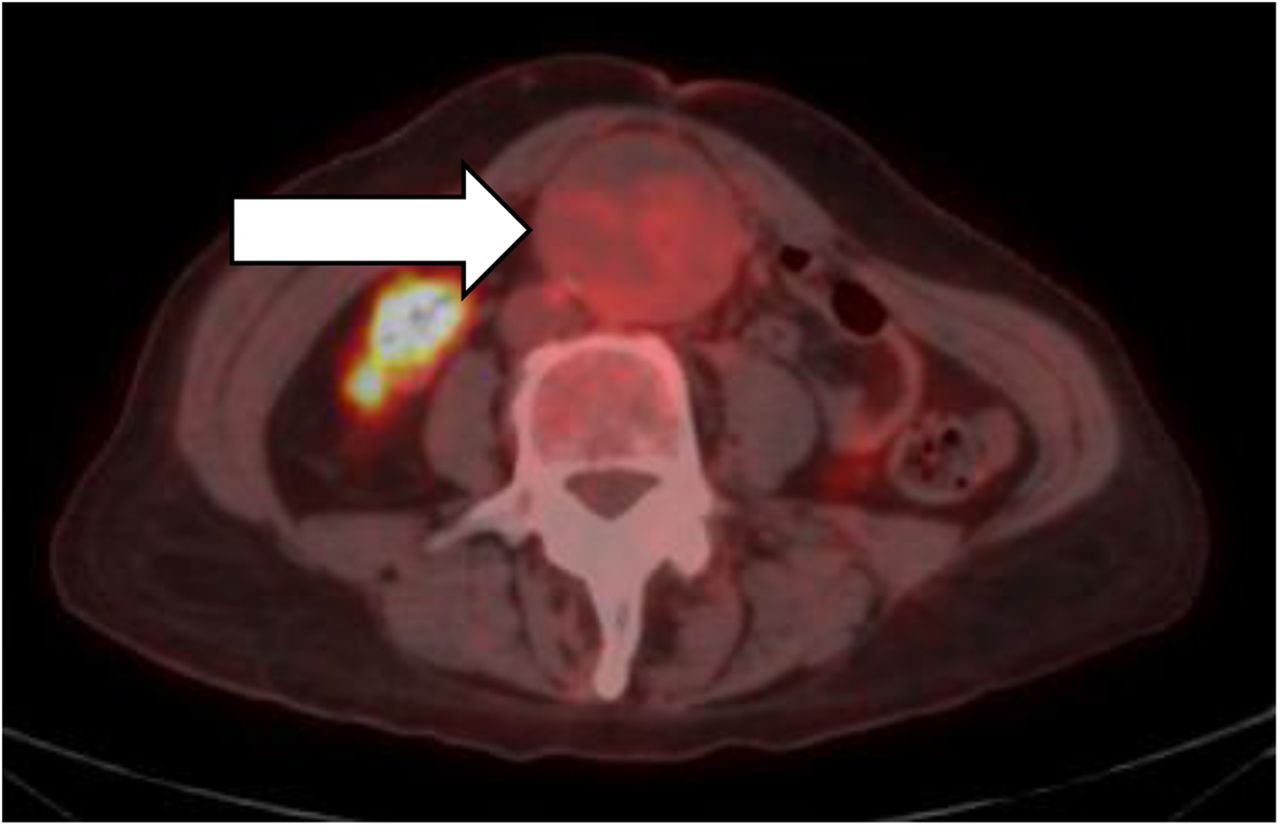
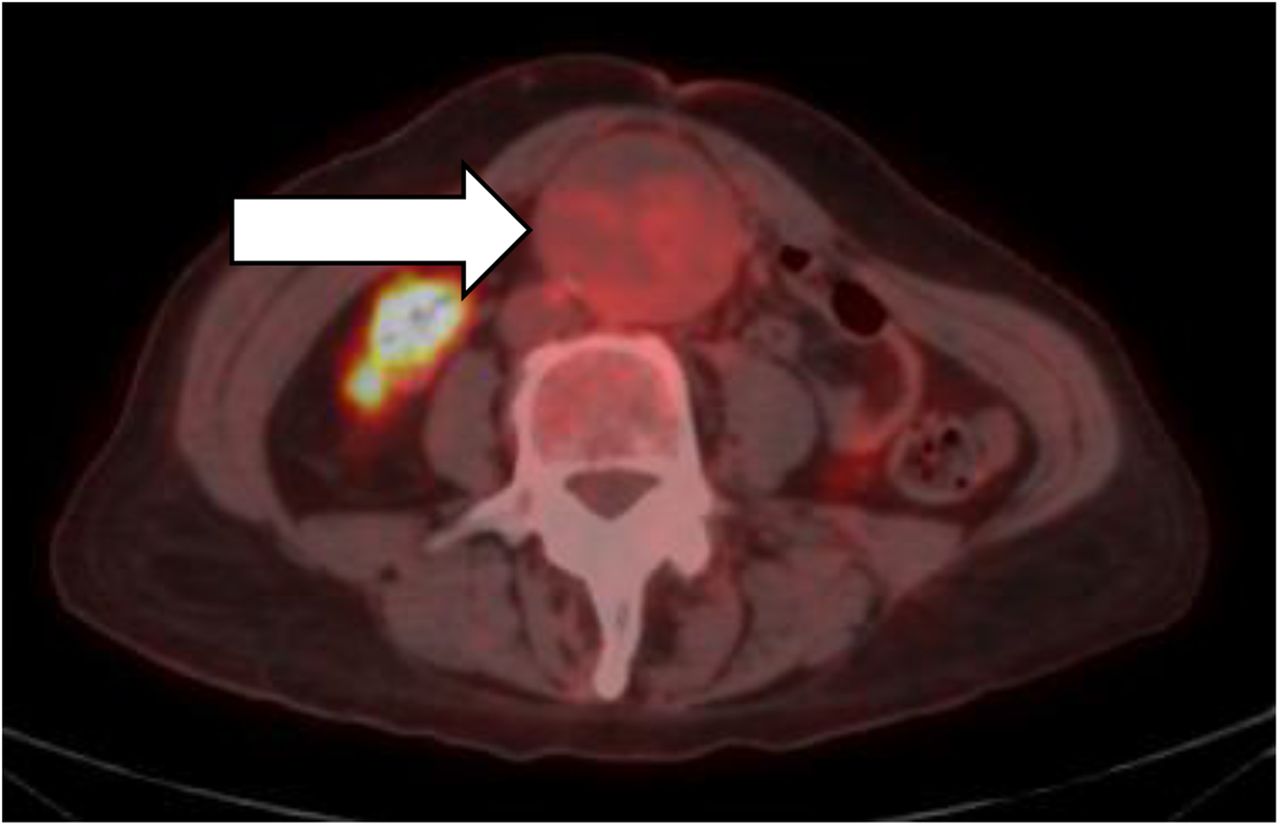
- FIGURE 7.
Abdominal aortic aneurysm on fused axial image.
- FIGURE 8.
Multiple incidental findings in melanoma patient. (A) Fifth finger of left hand was jammed while patient was playing basketball, and contamination of right forearm was suspected. (B) Left heel was broken and sore from cast; hammer toe was seen in right second toe, and bone spur was seen in right first toe. (C) After right forearm had been cleaned and a limited scan performed, contamination was confirmed.
- FIGURE 9.
Images of pregnant patient: axial fused (A), axial CT (B), axial attenuation-corrected (C), and coronal fused (D).


Tables
Questions about… Relevance Recent surgeries or biopsies After surgery or biopsy, healing may increase 18F-FDG uptake. Negative or unknown biopsy result may prompt physician to postpone imaging of area of interest. Positive result may prompt physician to proceed with imaging to look for distant metastasis (4). Diabetes Diabetic patients are best scheduled for earliest available appointment because they cannot eat or drink beforehand. Blood glucose should be <150–200 mg/dL, depending on facility’s protocol. Use of insulin degrades scans; insulin may need to be withheld or diabetes management temporarily changed (1,2). Claustrophobia Claustrophobic patients may need anxiolytic medication and a driver. Ability to lie supine for 30 min Patients need to know that scanning may take 30 min and that they will need to lie supine during it. To comply, many may require pain medication and a driver. In extreme cases, prone or on-the-side positioning may be needed. Exercise Exercise tears down and rebuilds muscle, causing 18F-FDG uptake. Scheduling scan 24–48 h after strenuous exercise allows uptake in muscles to dissipate (2,4). Antibiotics If patient is taking antibiotics because of infection, physician may postpone scan to avoid uptake by infected tissue. Steroids Learning that patient is taking steroids may reveal a current medical condition that will affect scan (5). Also, physician needs to know of steroid use because it can elevate blood glucose and decrease tumor metabolism, reducing SUVs. Pregnancy or breastfeeding Scanning is usually contraindicated in pregnant or breastfeeding patients. Some facilities may require pregnancy test on day of scan or written informed consent to scanning. Breastfeeding is withheld for 18–24 h after scan; 18F-FDG secretion into breast milk is minimal, but close contact exposes child to radiation. Also, there may be increased uptake in erector spinae muscles of mother (6). Travel to home after exam If patient lives far from exam site, traveling from exam with a pregnant woman or small child is not advisable because they will be exposed to radiation from patient. Duration of scan Patients who do not know that scanning takes 2 h may make other appointments for same day and choose to reschedule without giving advanced notice. Other scanning before PET scan If patient is scheduled for scan requiring contrast agent before PET scan, the agent may attenuate the PET signal. Nothing-by-mouth instructions Patients must not eat or drink for 4–6 h before undergoing scan. Need for any special dietary or medication arrangements should be determined (2), as well as patient’s willingness to comply with instructions. Questions about… Relevance Diabetes Current glucose level Scanning is contraindicated when blood glucose is >150–200 mg/dL. Facility reschedules scan in most cases (1) or may apply wait-period protocol. Usual glucose level If blood glucose is higher or lower than usual for individual patient, physician may reschedule scan. Time of last insulin dose* Use of insulin degrades scans; insulin may need to be withheld, its timing altered, or diabetes management temporarily changed (1,2). Injection Injection questions are asked for use by technologist and as quick reference for interpreting physician but do not substitute for entering dose on scan order or in medical record. For computerized dose tracking and SUV computation, dose is input before scanning. Staging Prior PET scan date Physician may want to compare current scan with prior scan. Patient can confirm any scans found in medical records. Technologist will scan patient in same position as before unless new information dictates otherwise. Prior CT scan date Physician may want to refer to most current CT scan when interpreting PET scan. Contrast agent from recent scan may attenuate PET signal and cause facility to apply its wait-period protocol (7). Chemotherapy and radiation therapy Chemotherapy or radiation therapy may change physiology and thus uptake; questions on therapy are asked for use by technologist and for interpreting physician’s reference (8,9). Date of recent surgeries or biopsies If scanning takes place too soon after surgery for cancer, increased uptake from healing may interfere with image interpretation (9). Prior malignancies Although patients are scanned per indication on order, knowledge of prior cancers such as melanoma may require that scan range be changed (3). Prior surgeries or biopsies Questions about whether patient has ever had surgery may elicit a problem the patient has with lying flat or still and may be helpful for physician when viewing altered physiology or anatomy. Prior experience with medical devices Information gained by asking if patient has prior experience with implants, intravenous lines, or ostomy sites may help in determining placement of bags on imaging table (after emptying, if involving urine) and patient’s ability to lie flat with such devices in place. Screening Coronary artery disease and pacemakers Questions about coronary artery disease may elicit a problem the patient has with lying flat or still. Coronary artery disease can affect clearance of intravenous contrast agents. It is helpful to know in advance that scout scan will show a pacemaker, and technologist can ensure that its implantation date was at sufficient interval before scan, in accord with facility’s protocol (10). Metallic objects Artificial joints, shrapnel, and other metallic objects may cause CT attenuation and star artifact, which, depending on type of scanner software, may affect SUV. Physician should be aware of such objects in case patient departs, and thus cannot be questioned, before images are ready for interpretation (11). Claustrophobia and lying supine for 30 min Even if patient denied, at scheduling, being claustrophobic or unable to lie supine, the question should be asked again before injection. Simply showing scanner to patient may reveal need for anxiolytic medication and rescheduling. Questioning also allows technologist to confirm that medicated patients have driver. Exercise Questioning about exercise allows technologist to confirm compliance with prior instruction not to engage in strenuous exercise for 24–48 h before scan (2,4). Intramuscular injections Intramuscular injections such as flu or other vaccinations can cause increased uptake. Awareness of any such injections is important in image interpretation, especially for melanoma patients (3). Infections Infection can cause increased uptake, especially in chemotherapy patients. Awareness of current infection allows scan to be rescheduled, if necessary, to prevent difficulty with differentiating between infection uptake and cancer uptake (12). Recent trauma If patient has sustained recent trauma, such as car accident or fall, uptake from healing may interfere with image interpretation (12). Type of trauma may also affect patient’s ability to lie flat and still during scanning. Pain Tensing muscles near site of pain can cause increased muscle uptake, just as occurs during exercise. Inquiring about pain can also elicit whether patient can lie still and flat. Renal failure In facilities that use intravenous contrast agents, knowledge of patient’s renal function is important. Also, dialysis patients requiring PET may need to be scheduled for nondialysis day, depending on facility’s protocol. Chronic obstructive pulmonary disease Answers to questions about chronic obstructive pulmonary disease can be another indicator of whether patient can lie flat. Allergies Use of intravenous contrast may be contraindicated in patients allergic to iodine or seafood. Also, in emergencies, medical responders need to be aware of any known allergies (13). Contrast reactions If intravenous contrast is to be given, patient must be questioned not only about renal function and allergies but about any prior contrast reaction, no matter how minor. In such cases, supervising physician must approve administration, facility’s intervention protocol must be followed, and patient may need to sign statement about past reaction (13). ↵* For insulin-dependent diabetic patients.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.