


Abstract
18F-FDG PET imaging of tumors has pitfalls and pearls of wisdom that begin at the point of scheduling and continue through the patient interview, the resting phase, the scan itself, and the image review. Interviewing the patient at the time of scheduling, followed by placing a reminder phone call shortly before the appointment, can save a nuclear medicine department the financial loss of wasted doses and missed appointment slots in the schedule. The pitfalls and pearls of wisdom in tumor imaging are ever changing, and the technologist is in a constant state of inquiry about the patient’s disease process and ability to comply. Consideration of each item on the worksheets in this article affects every scan. On completing this article, the reader will be able to identify questions that should be asked in the scheduling and preinjection patient interviews, interpret the answers to those questions, determine how the images may be affected, and adapt the scan.
PET imaging of tumors using 18F-FDG has pitfalls and pearls of wisdom that begin at the point of scheduling and continue through the patient interview, the resting phase, the scan itself, and the image review. Interviewing the patient at the time of scheduling, followed by placing a reminder phone call shortly before the appointment, can save a nuclear medicine department the financial loss of wasted doses and missed appointment slots in the schedule. The patient may also be spared the anxiety and expense of taking a day off from work and traveling to the facility, only to be disappointed that the scan cannot be completed. The interview provides important information in addition to the ordering physician’s indication for the PET scan. After the scan, the image review process also provides information about whether additional limited scans or potential emergent patient care is needed. This article is not intended as a guideline for imaging but as a discussion of a few pitfalls and pearls of wisdom that may assist the technologist and nuclear medicine department in reaching the goal of completing PET scans of diagnostic quality within a reasonable time frame. An added goal is to accomplish the scan in a manner that reduces stress on the patient and strain on the imaging facility’s resources.
18F-FDG, a glucose analog used in PET, can be transported and phosphorylated in the cell but cannot be metabolized rapidly and is trapped in the cell in the same proportion as glucose. Because many malignancies present with increased glucose use, PET imaging can provide a sensitive method of staging various cancers and monitoring the effects of therapies (1,2).
THE SCHEDULING INTERVIEW
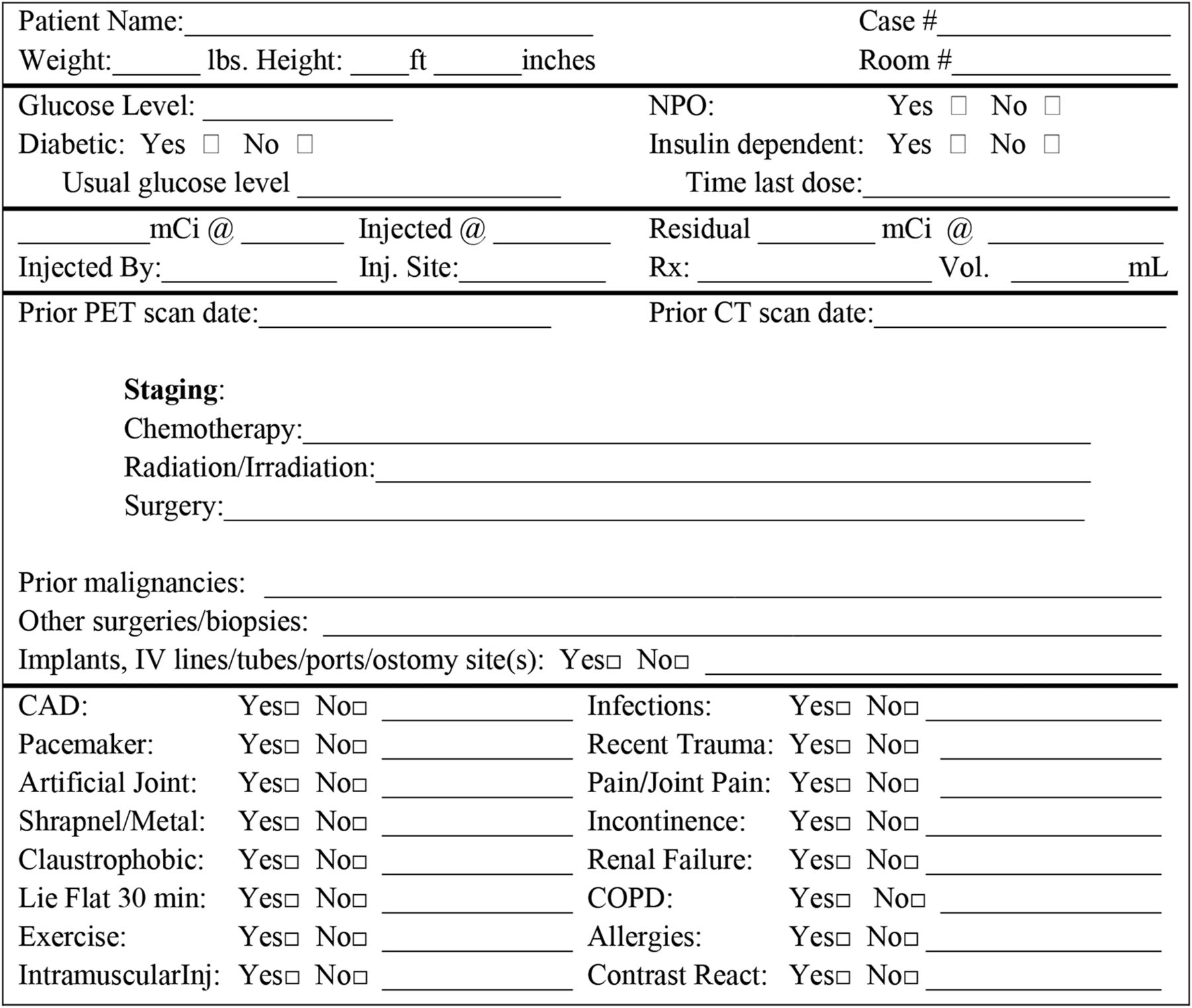
After a physician has ordered a PET scan and its indication has been found to be appropriate both for the patient’s condition and for insurance reimbursement, the technologist or another member of the staff contacts the patient to schedule an appointment. Because there are many considerations in determining an appropriate date and time for the appointment, as well as many factors that can affect the quality of the scan, the scheduler uses a worksheet to record the patient’s answers to a series of questions. An example worksheet is presented in Figure 1 and discussed in Table 1.
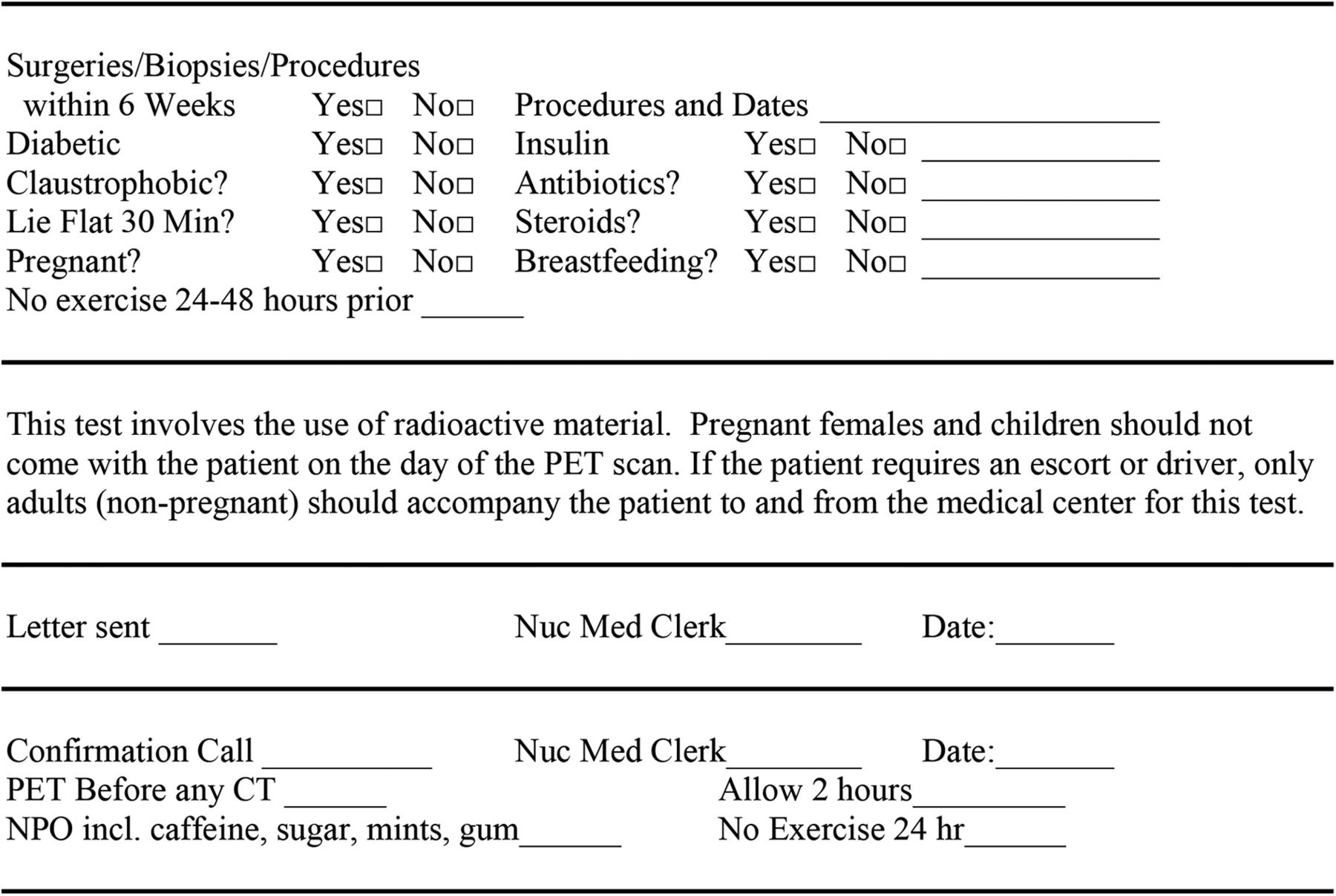
Scheduling interview.
Questions to Ask at Scheduling
These questions are a valuable tool for screening and scheduling and can help reach the goal of completing PET scans of diagnostic quality within a reasonable time frame. Efficiency in scheduling also reduces patient stress and improves management of disease. Although each physician and facility may have slightly differing procedures and protocols for the issues addressed by these questions, all the answers should be considered in scheduling the appointment.
THE CONFIRMATION LETTER AND REMINDER PHONE CALL
Many PET patients are feeling the burden of their disease on their energy level and alertness, and pain medications may increase forgetfulness. It is a good practice to send a confirmation letter immediately after scheduling and to place a reminder phone call within a few days before the appointment. The latter allows for screening for new developments, maintenance of scheduling, reinforcement of instructions, and avoidance of wasted doses. The preexam phone call is also critical if the examination is scheduled by a centralized center whose staff may not be familiar with the importance of patient preparation for PET scans.
THE PREINJECTION INTERVIEW
After arriving for the appointment and before receiving the injection, the patient is asked another series of questions that may assist the technologist in completing the scan and the physician in interpreting the images. An example worksheet for recording the answers is presented in Figure 2 and discussed in Table 2. Screening questions about pregnancy and breastfeeding are also always necessary. These questions can be added to the main worksheet or maintained on a separate sheet, and it is wise to have the patient sign a statement about her pregnancy status. Likewise, questions about previous contrast reactions may be added to the main sheet or maintained separately and the patient’s signature again obtained. For easy reference, the worksheet can be divided into sections such as demographics, glucose information, injection information, and staging and screening questions.
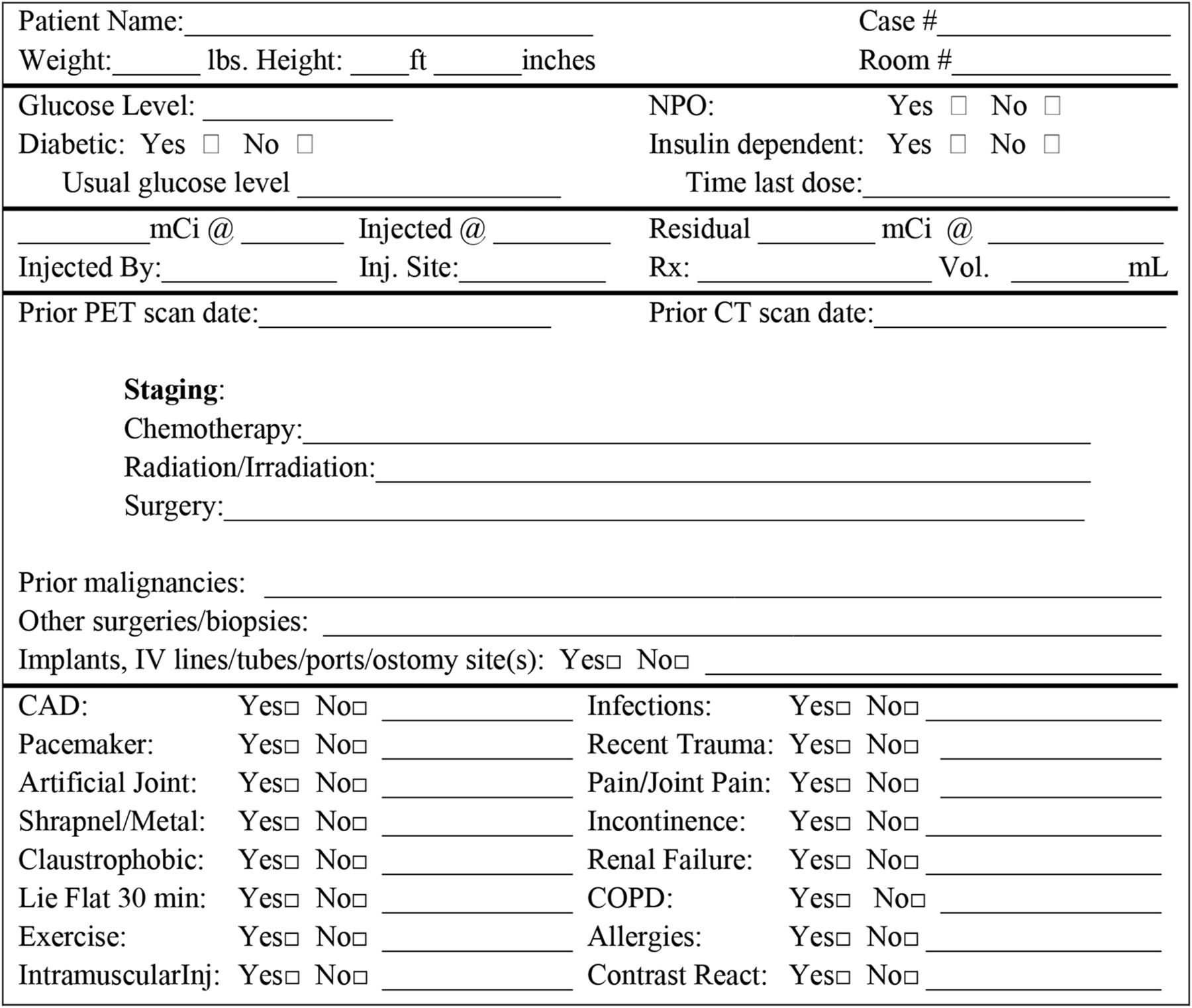
Preinjection interview.
Question to Ask Before Injection of 18F-FDG
The worksheet can be printed in half-sheet size and clipped to the order, helping the interview stay on track if the technologist is temporarily pulled away from it or has to transfer the patient’s care to another technologist.
The worksheet can also help with decisions on how to scan the patient. For instance, a facility’s protocol may dictate that patients be scanned from the middle of the thigh to the base of the skull (“thigh to eye”) to allow for scanning of the bladder before it has a chance to fill. However, for a claustrophobic patient or a patient with dementia, scanning in the opposite direction may be beneficial. When scanned from thigh to eye, the patient is taken through the gantry to the thigh and slowly brought back into the scanner. Claustrophobic patients may panic when nearing the enclosed space and may move or refuse to complete the scan. Patients with dementia may have trouble remembering to keep their head still for the entire duration of a lengthy scan. Scanning the head first so that it exits the gantry first helps claustrophobic patients to complete what is, to them, the worst part of exam early and lie still for the remainder; likewise, head movement in patients with dementia will have a lower impact if the head is scanned first. Another example of how the preinjection interview can help decide the direction of scanning is a patient who requires PET for lung cancer but, on questioning, reveals previous melanoma. The technologist might then ask the interpreting physician whether to scan from the top of the head to the bottom of the feet because melanoma can metastasize not only to organs but to other areas on the skin (3).
The patient history recorded on the worksheet can also alert the physician to factors that may affect interpretation of the scan.
THE CASE OF INACCURATE ANSWERS
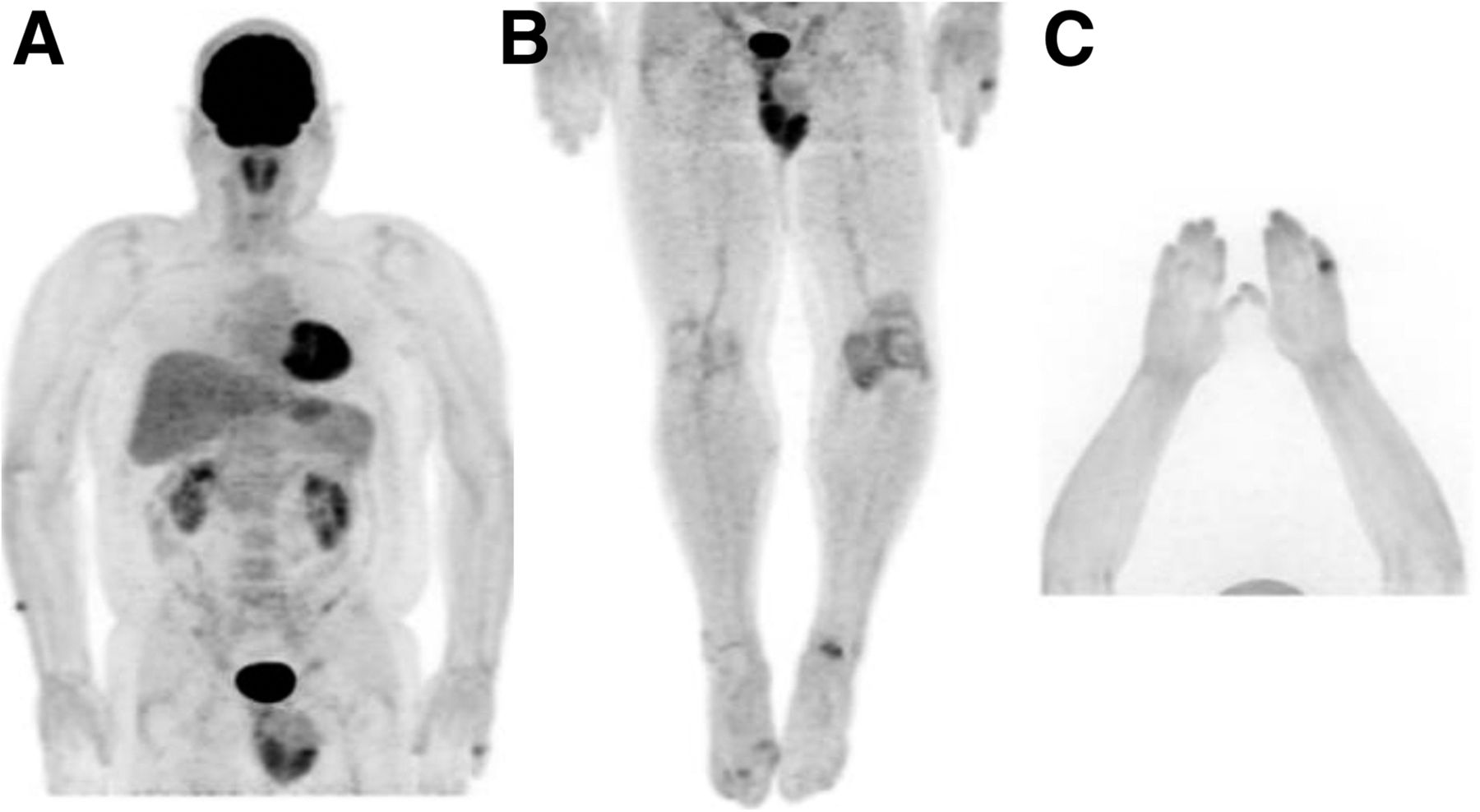
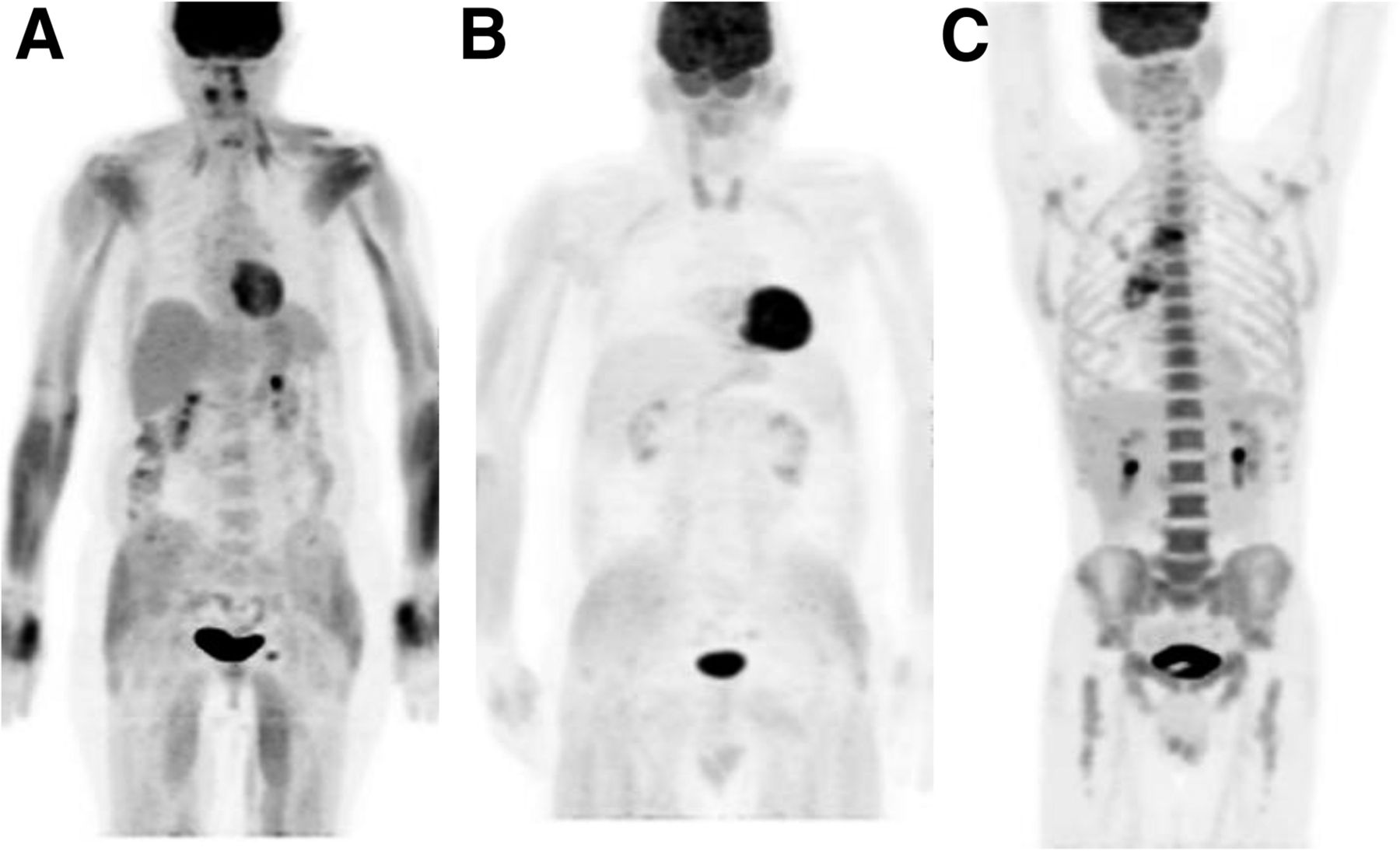
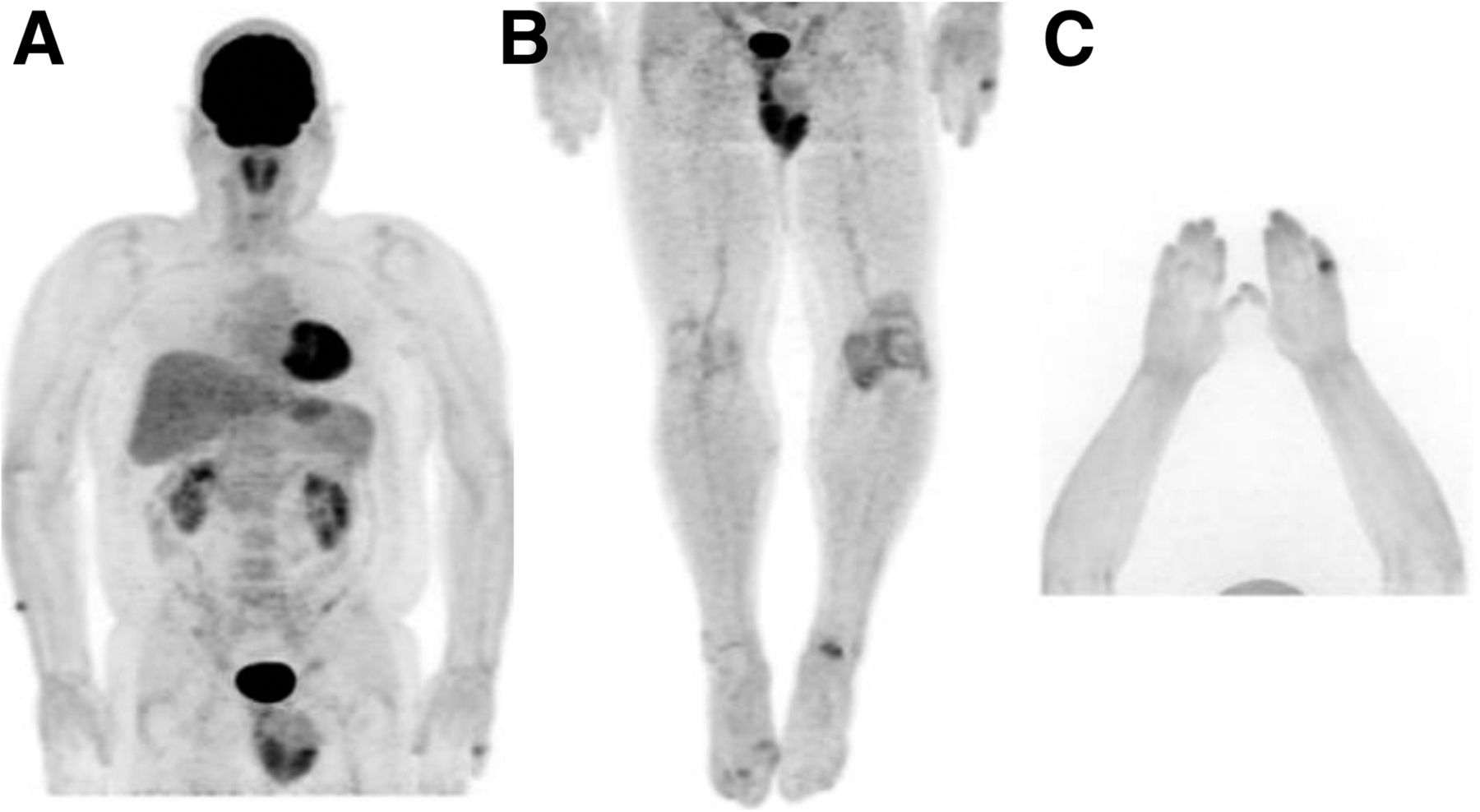
Patients who feel burdened by illness or take medications that increase forgetfulness may not answer a question truthfully or even fully understand it or remember the correct answer. For example, a patient who claims not to have done any strenuous exercise within the last 24–48 h may have images indicating otherwise. After being scanned and then questioned further, the patient in Figure 3A admitted that he had actually “pulled a fence” the day before.
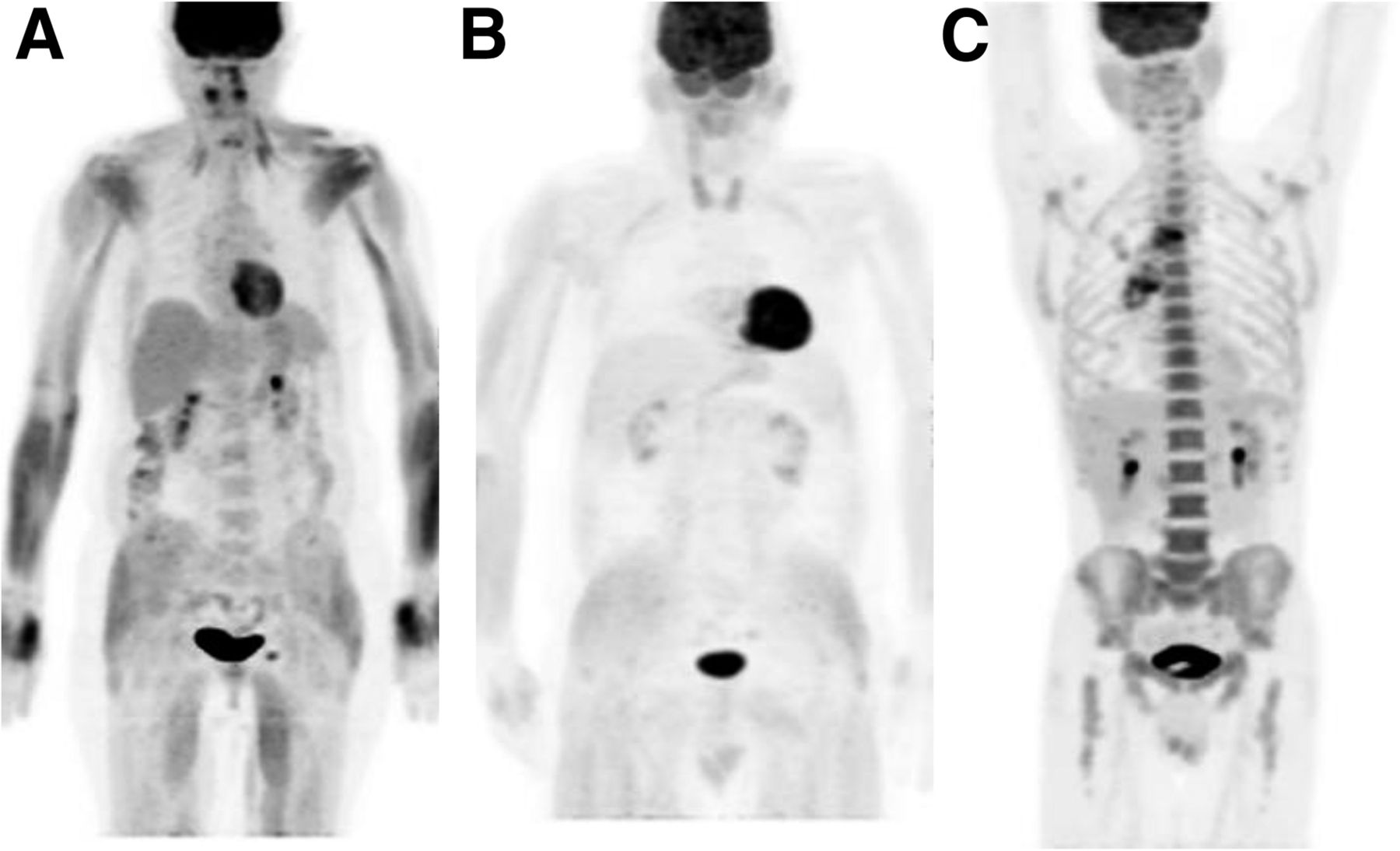
Maximum-intensity-pixel 18F-FDG PET images of patient who exercised strenuously 24 h before the scan (A), patient who took insulin the morning of the scan (B), and patient who was receiving granulocyte-colony-stimulating factor (C).
If a patient denies taking insulin but actually did, images such as Figure 3B may reveal the truth. In this example, the patient denied taking insulin before injection, testing showed his glucose to be within the desired range, and the scan was performed. After imaging and on further questioning by both the technologist and the radiologist, the patient continued to deny taking insulin until finally admitting to taking it on the morning of the scan to lower his glucose level to below the facility limit.
Some patients may be receiving granulocyte–colony-stimulating factor, which may increase bone marrow activity on an 18F-FDG scan, resulting in images such as Figure 3C. Activity in the spleen can be increased as well. Additionally, both increased bone marrow activity and increased splenic activity can be seen in anemic patients (2).
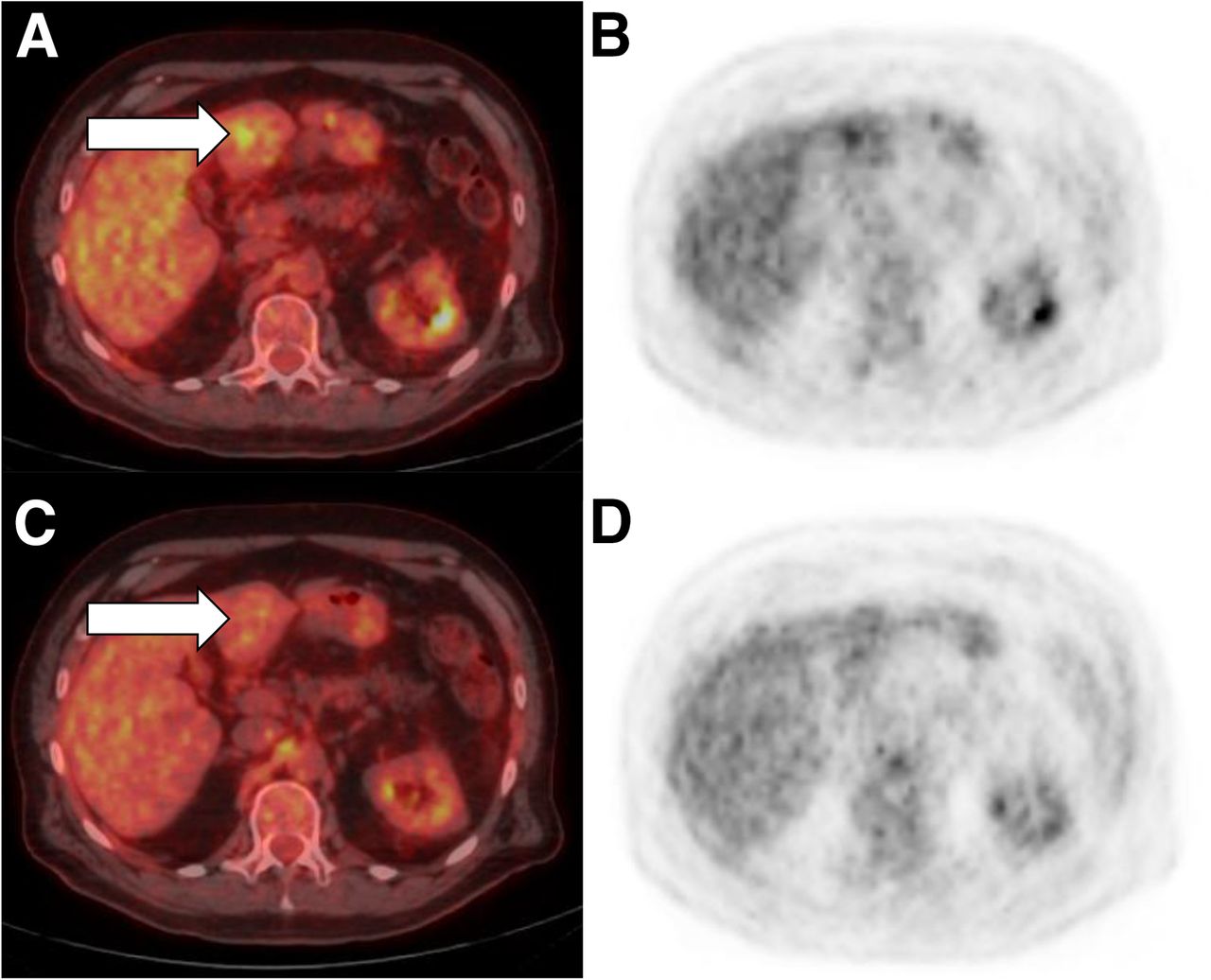
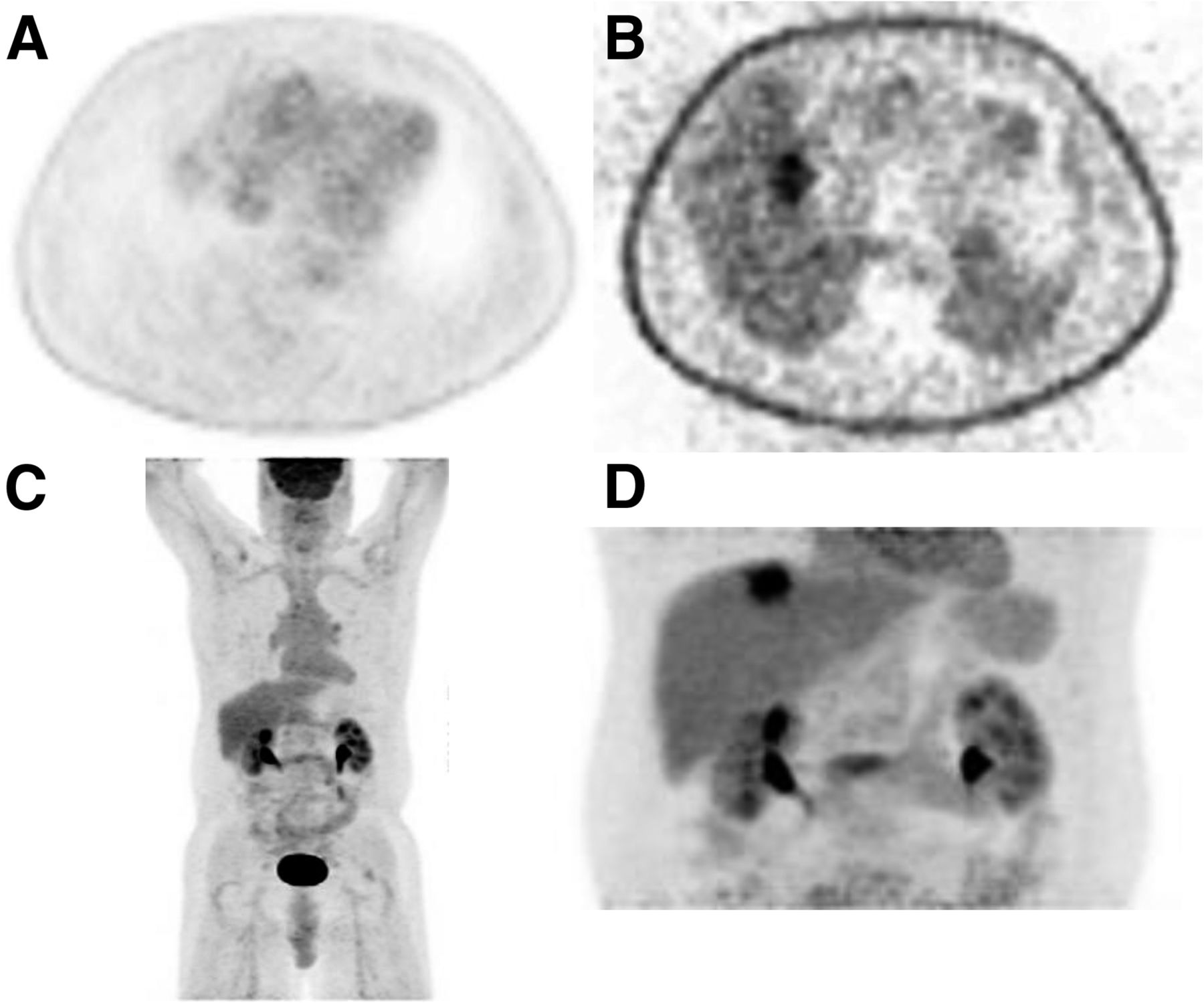
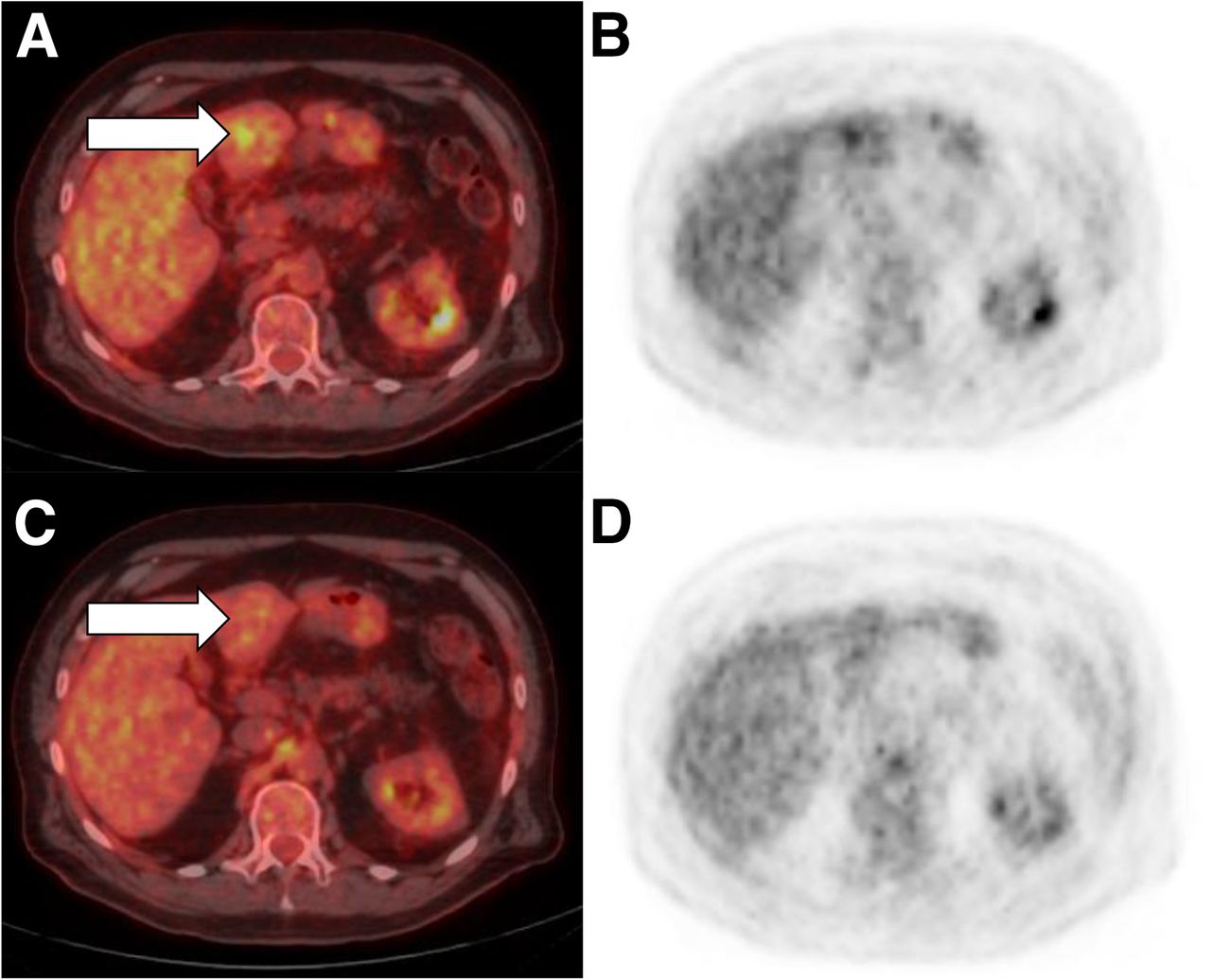
It is important to check non–attenuation-corrected images for false-negative findings, especially in the base of the lung and dome of the liver, where breathing motion occurs. For example, the attenuation-corrected image in Figure 4A and the maximum-intensity-pixel image in Figure 4C do not seem to reveal a lesion, whereas the non–attenuation-corrected image in Figure 4B clearly indicates a positive site. A follow-up limited scan with additional time to allow for more counts can reveal the lesion, as seen in Figure 4D, or can reveal that a positive site is actually false-positive, as seen in Figure 5.

False-negative findings on attenuated-corrected axial image (A), non–attenuation-corrected axial image (B), maximum-intensity-pixel image (C), and maximum-intensity-pixel additional limited image with increased time to allow for more counts (D).
False-positive findings on fused axial image (A) and attenuation-corrected axial image (B). Additional limited scan was performed with delay to allow for clearance and for more counts on fused axial image (C) and attenuation-corrected axial image (D).
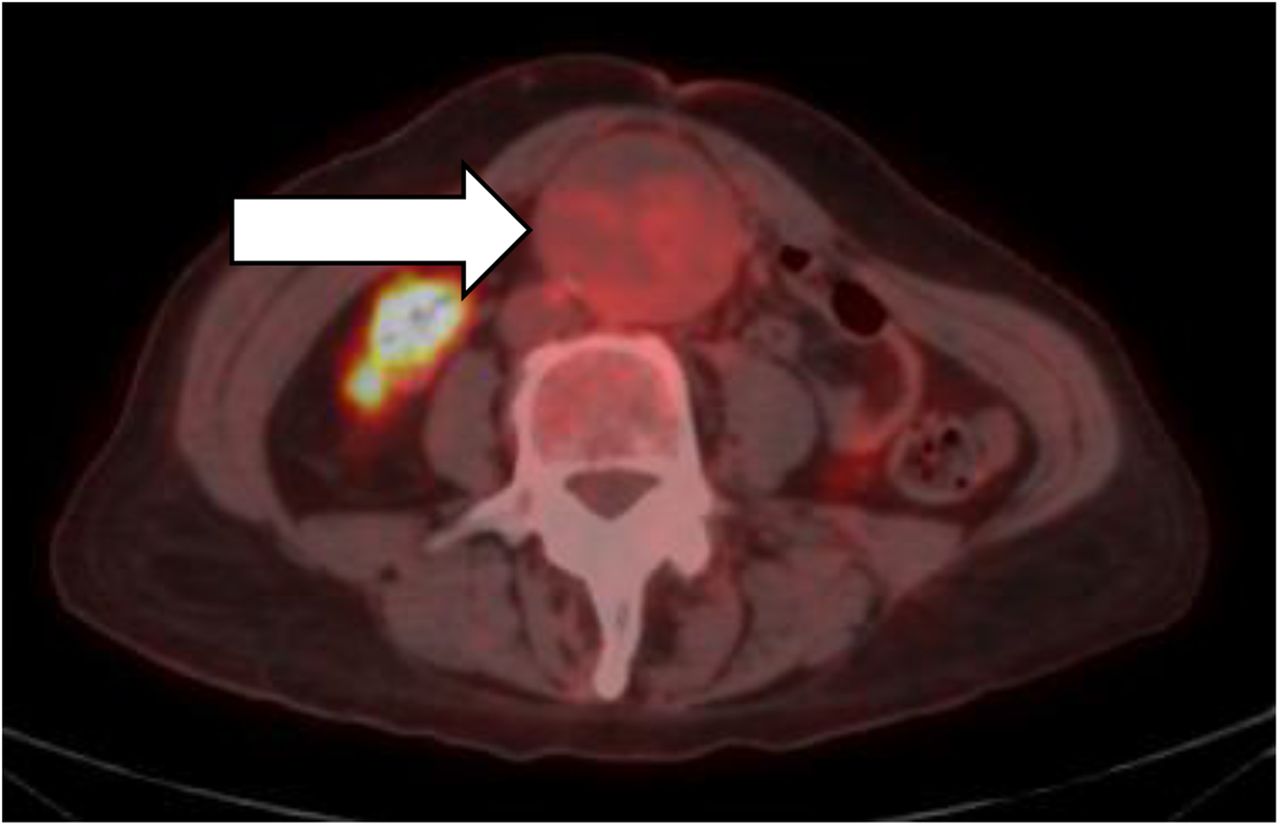
During the image review process, it is also important to check for the possibility of a pneumothorax (Fig. 6), especially in lung cancer patients. Likewise, the aorta should be checked from the arch through the bifurcation for an abdominal aortic aneurysm. A physician should be notified if a pneumothorax or an abdominal aortic aneurysm is discovered, to determine whether immediate medical intervention is required (Fig. 7).
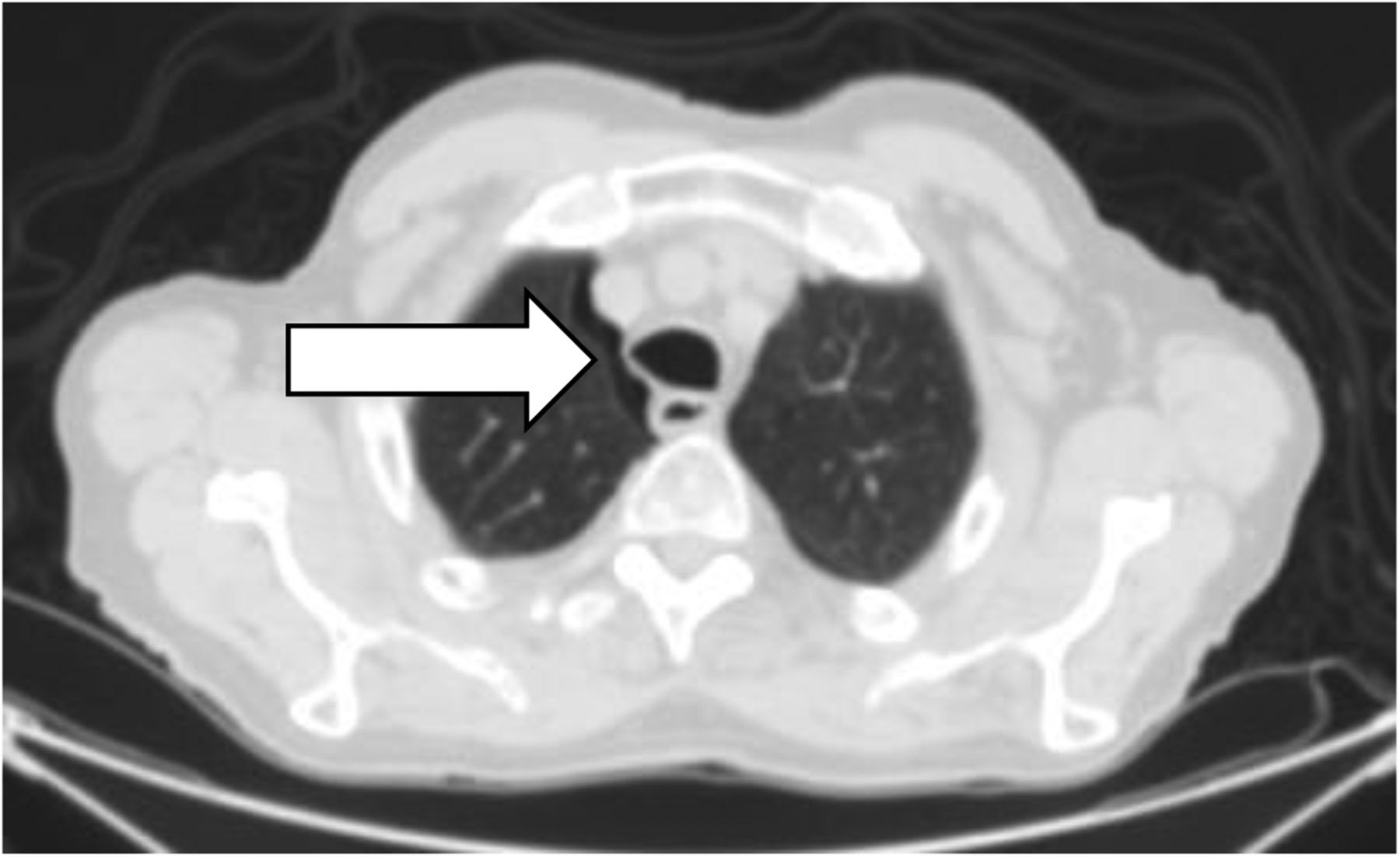
Pneumothorax on axial CT image displayed in lung window 1,500 and level −550.
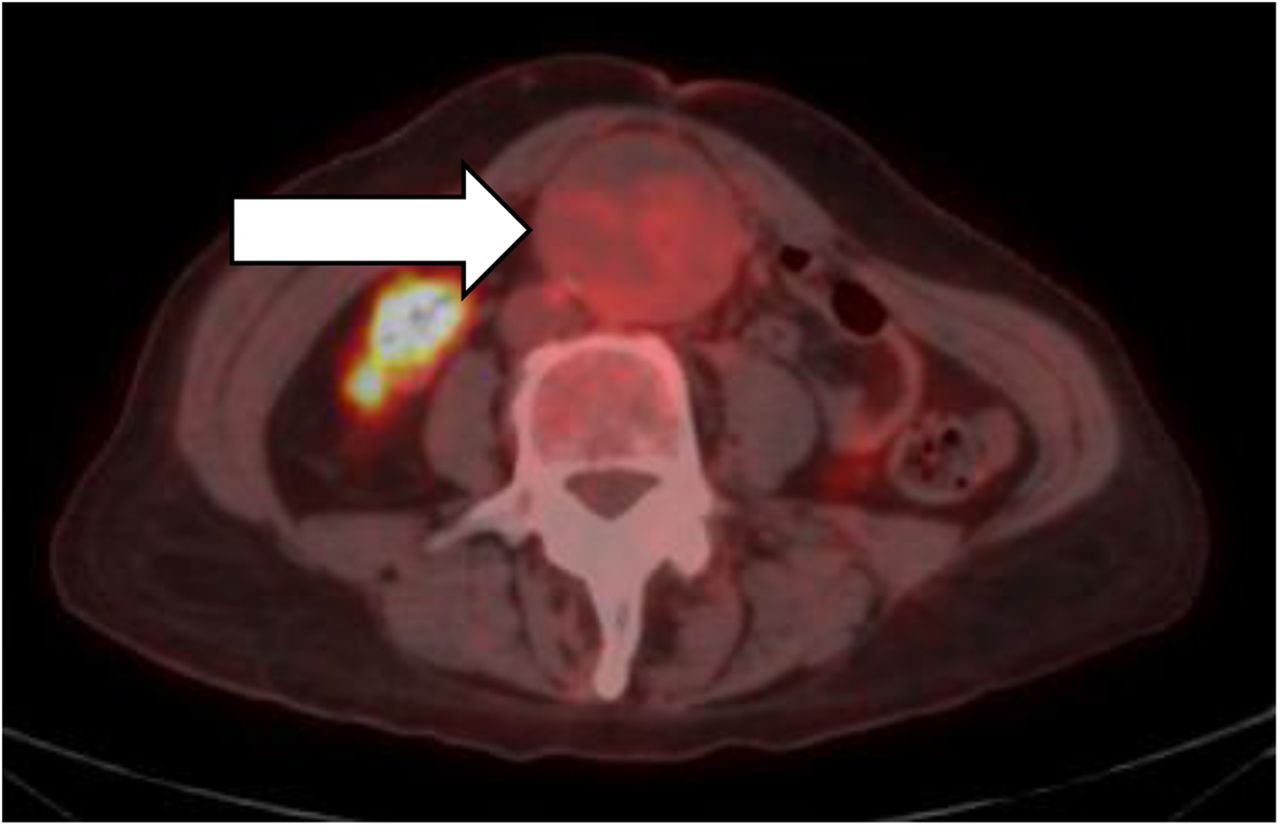
Abdominal aortic aneurysm on fused axial image.
The importance of the patient interview can again be illustrated by the multiple incidental findings in the melanoma patient shown in Figure 8. Findings that at first seemed to be positive matched the history given by the patient and were instead determined to be incidental. The patient indicated that the fifth finger on the left hand had been jammed playing basketball, the left heel had been broken and was sore from a cast, the right second toe was a hammer toe, and the right first toe had a bone spur. There was an area of possible contamination on the right forearm that was confirmed as such after it was cleaned and a limited scan of that area performed.
Multiple incidental findings in melanoma patient. (A) Fifth finger of left hand was jammed while patient was playing basketball, and contamination of right forearm was suspected. (B) Left heel was broken and sore from cast; hammer toe was seen in right second toe, and bone spur was seen in right first toe. (C) After right forearm had been cleaned and a limited scan performed, contamination was confirmed.
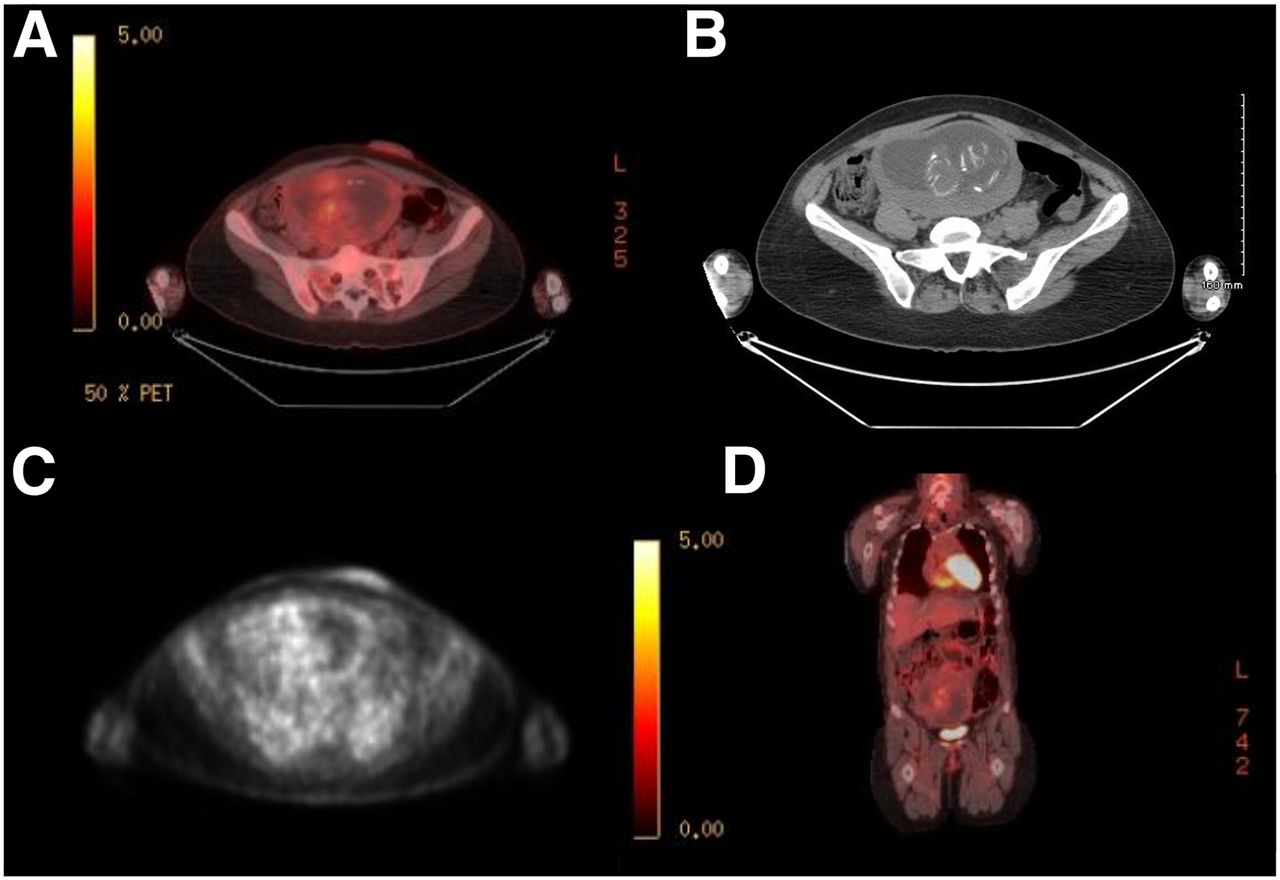
It is ingrained in us as radiologic science professionals to always screen female patients within a certain age range for the possibility of pregnancy before administering any dose of ionizing radiation. Although some facilities require a pregnancy test of such patients before proceeding with imaging, many facilities require only the patient’s attestation verbally or in writing. Patients may intentionally lie or may honestly believe there is no possibility they could be pregnant. Many undergoing treatment for cancer, especially cancer of the reproductive organs, are under the impression that they cannot conceive. However, if a patient’s reproductive organs are intact and she is sexually active, she might conceive. A urine or serum pregnancy test remains the best way to ensure a patient is not pregnant and protect the facility from legal repercussions. Figure 9 shows a PET scan of a patient who, on being interviewed by the technologist, adamantly swore there was no chance she could be pregnant; she insisted that she was not pregnant and had not been sexually active. After completing the scan, the technologist was quite surprised to see a fully formed fetus on the images. The interpreting radiologist determined through femur measurements that the fetus was at a gestational age of approximately 14–15 wk. It was also determined that the patient had undergone a PET scan 3 mo previously, about 2 wk after conception. This example highlights the importance of ensuring without doubt that a patient is not pregnant before proceeding with an examination.

Images of pregnant patient: axial fused (A), axial CT (B), axial attenuation-corrected (C), and coronal fused (D).
CONCLUSION
From the time of receiving the physician’s order until the time of scheduling the appointment, interviewing the patient, injecting the 18F-FDG, performing the scan, and reviewing the images, the technologist is in a constant state of inquiry about the patient’s disease process and ability to comply. Consideration of each item on the worksheets in this article affects every scan. Avoiding the ever-changing pitfalls and learning the ever-increasing pearls of wisdom is sometimes a tiring endeavor but can be rewarding even if only by improving future success in obtaining diagnostic-quality scans within a reasonable time and with reduced stress on the patient and strain on the facility’s resources.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank Lindsay Wendel, RT(CT)(N), for her contributions to the worksheets in this article.
Footnotes
Published online Apr. 21, 2016.
CE credit: For CE credit, you can access the test for this article, as well as additional JNMT CE tests, online at https://www.snmmilearningcenter.org. Complete the test online no later than June 2019. Your online test will be scored immediately. You may make 3 attempts to pass the test and must answer 80% of the questions correctly to receive 1.0 CEH (Continuing Education Hour) credit. SNMMI members will have their CEH credit added to their VOICE transcript automatically; nonmembers will be able to print out a CE certificate upon successfully completing the test. The online test is free to SNMMI members; nonmembers must pay $15.00 by credit card when logging onto the website to take the test.
REFERENCES
- Received for publication December 3, 2015.
- Accepted for publication February 22, 2016.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}