


Abstract
Os acromiale is an anatomic variant that in rare cases can cause pain. 99mTc-methylene diphosphonate bone scintigraphy with SPECT/CT can play an important role in diagnosing this clinical entity. We present a male football player with shoulder pain secondary to a symptomatic os acromiale, and we demonstrate the findings on bone scanning with limited SPECT/CT that diagnosed this important clinical abnormality.
In this report, we present a male football player with shoulder pain secondary to a symptomatic os acromiale. We demonstrate the findings on bone scanning with limited SPECT/CT that diagnosed this important clinical abnormality.
CASE REPORT
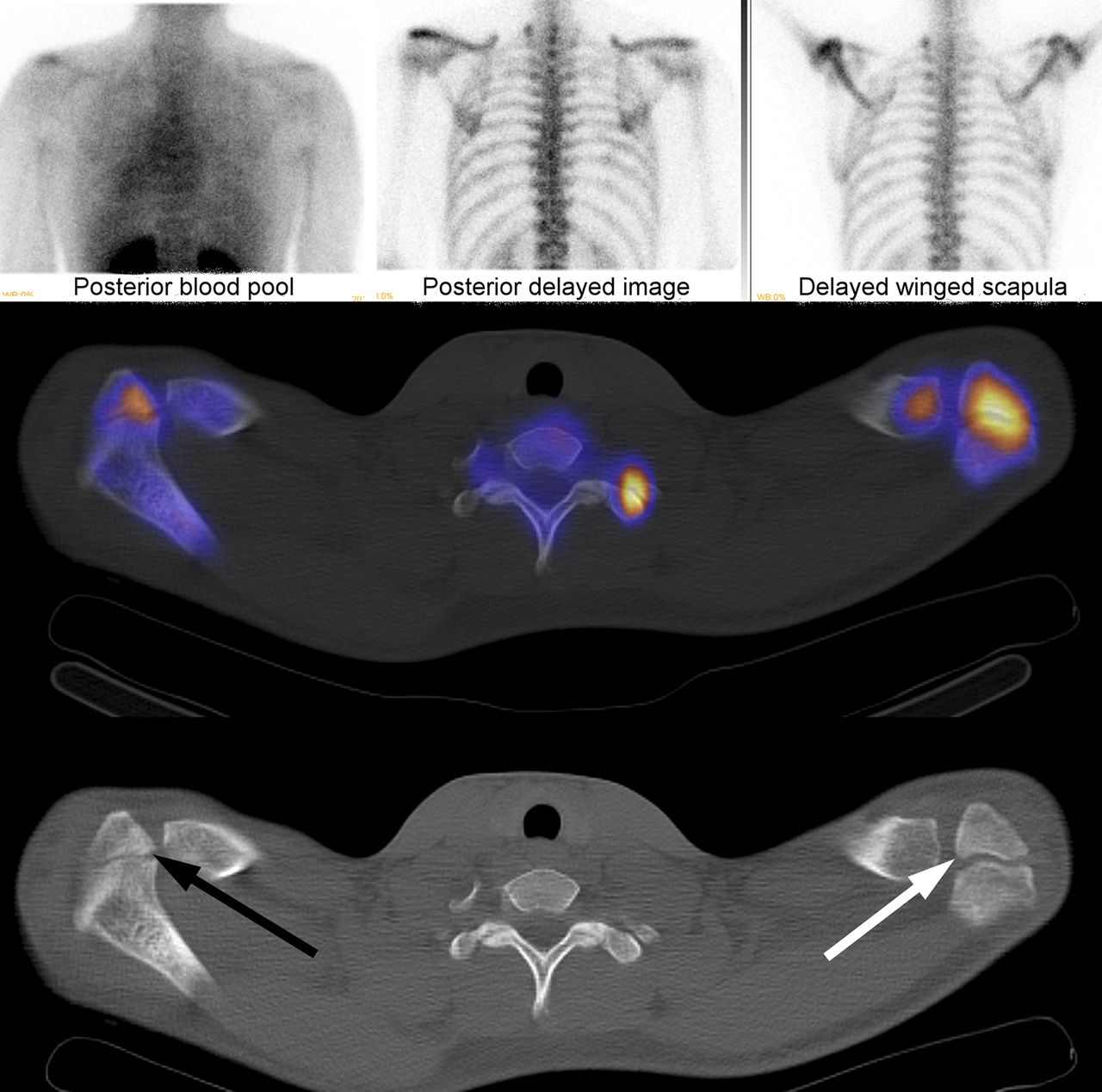
An 18-y-old male American football player presented with persistent left shoulder pain and the inability to abduct his arm beyond 45° for the past 6 mo. Plain radiography was unremarkable, and MR imaging did not reveal a rotator cuff tear. 99mTc-methylene diphosphonate bone scintigraphy was performed using 897.6 MBq (24.26 mCi) on a dual-head camera fitted with high-resolution, low-energy collimators. Blood-pool images were obtained shortly after injection, and delayed static images were obtained approximately 3 h after the initial injection. The images revealed asymmetric increased activity near the left acromion process on the early blood-pool and delayed static images. SPECT/CT was performed for further anatomic localization with the field of view restricted to the shoulders. The images demonstrated incomplete fusion of both acromion processes, which could be age-related in this patient. However, the ossification center in the left apophysis occurred at the meso-acromion rather than at the preacromion (as on the right side) and was associated with more activity (Fig. 1), indicating ongoing osteoblastic activity likely from incomplete fusion. This finding was consistent with painful os acromiale.
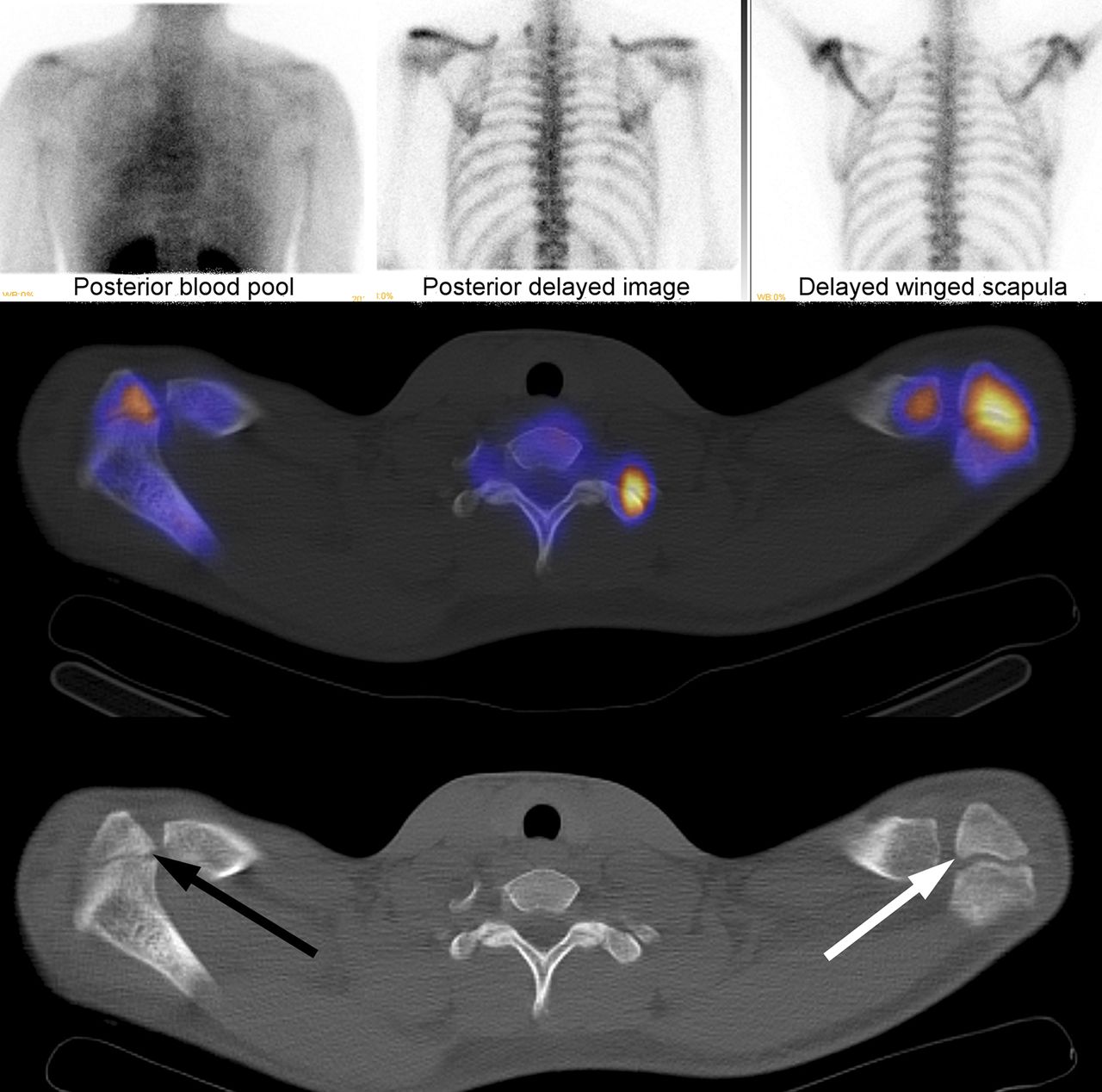
Top row shows static bone scan and blood-pool images, middle row images shows fused SPECT/CT images, and bottom row shows attenuation correction CT. Arrows are placed at ossification centers of apophyses. Center is at meso-acromion on left (white arrow) but at preacromion on right (black arrow). Right apophysis is nearly fused and has less activity than unfused apophysis of left acromion.
DISCUSSION
Os acromiale is an anatomic variant caused by the failure of the anterior acromial apophysis to fuse to the acromion process. Instead, it is joined to the scapular spine by fibrocartilaginous tissue rather than ossified bone (1). Os acromiale is typically an incidental finding that is present in about 8% of the population (1,2). It is rare for os acromiale to be symptomatic, but it has been implicated in shoulder impingement syndromes mimicking rotator cuff injuries (3). There are multiple cases that described painful os acromiale and were diagnosed with plain radiographs (4). However, this is the first time to our knowledge that painful os acromiale has been described on bone scintigraphy with SPECT/CT.
After failure of conservative treatment including physical therapy, nonsteroidal antiinflammatory agents, and subacromial corticosteroid, these patients usually undergo surgical intervention (5). Our patient failed conservative management and was subsequently referred for surgical resection of the incompletely fused ossification center to relieve his pain.
CONCLUSION
Os acromiale is an anatomic variant that in rare cases can cause pain. 99mTc-methylene diphosphonate bone scintigraphy with SPECT/CT can play an important role in diagnosing this clinical entity.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Feb. 5, 2015.
REFERENCES
- Received for publication October 14, 2014.
- Accepted for publication December 15, 2014.





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.