


Abstract
Settling of 18F-FDG in the bladder is often noted on whole-body PET/CT images, but this phenomenon has never received any careful attention and the mechanism has been unclear. The 2 patients described in this report, one with a T1 pathologic fracture and another with widespread bone and lymph node metastases from an unknown primary tumor, underwent PET/CT. Both had urinary tract infection and a distended bladder during scanning. The interesting layering of 18F-FDG in the urinary bladder was observed in both patients. The presence of this phenomenon demands careful evaluation of the urine by the clinician, and the mechanism is hypothesized to be slow 18F-FDG excretion in patients with a distended urinary bladder, resulting in delayed mixing with urine. In addition, urinary tract infection may be a potential cause. Images showing this interesting layering should be interpreted with care.
Accumulation of 18F-FDG in the urinary bladder usually makes evaluation of bladder lesions on PET/CT difficult. At our institution, urinary bladder activity is minimized by asking the patient to drink at least 500 mL of plain water and to void before image acquisition. However, settling of 18F-FDG in the urinary bladder is occasionally observed and can impose an interpretation challenge, obscuring or simulating pathologic findings (1). A recent study about intravenous contrast PET/CT stated that the higher specific gravity of the contrast material displaces the excreted 18F-FDG, resulting in anterior layering of the radiotracer (2). We report here 2 patients with bladder layering of excreted 18F-FDG on PET/CT without intravenous contrast material. We hypothesize that the phenomenon is due mainly to delayed mixing of 18F-FDG excretion with nonradioactive urine in a distended bladder and urinary tract infection. However, the mechanism needs to be further investigated in a more comprehensive study.
CASE REPORT
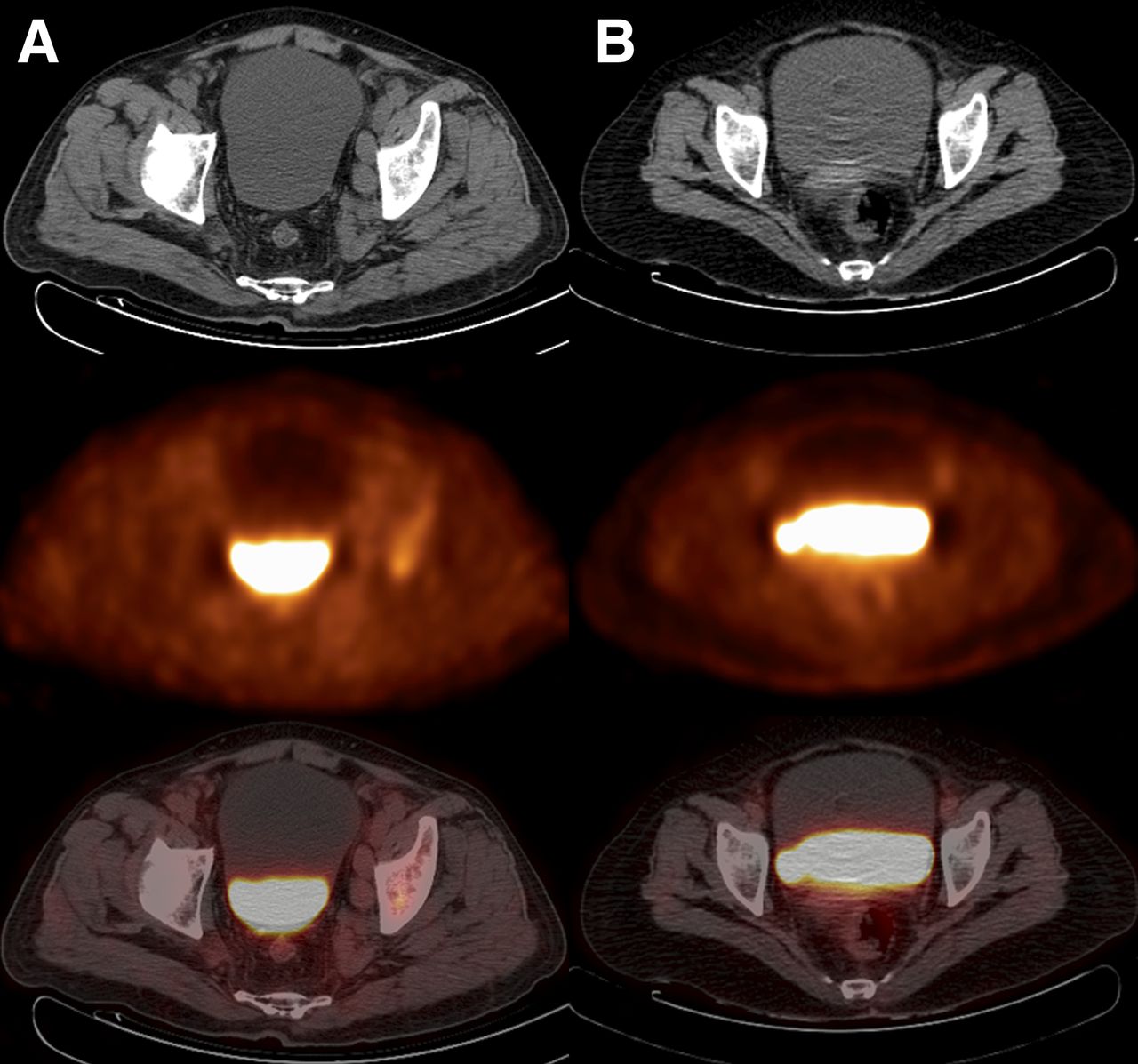
The first patient was a 63-y-old woman with neck and back pain and lower-limb weakness. She had undergone PET/CT examination, and the images showed a pathologic fracture in the first thoracic vertebra. There was interesting layering of excreted 18F-FDG in the urinary bladder, showing 18F-FDG–loaded urine at the bottom of a distended bladder and clear urine at the top (Fig. 1A). The combination of radiologic images and clinical examination revealed no bladder abnormalities but indicated a urinary tract infection. The second patient, who was 67 y old and male with fever of unknown origin, was diagnosed with widespread bone and lymph node metastases from an unknown primary tumor. In addition, he had symptoms of lung infection. A clear demarcation between the urine without 18F-FDG at the top of the bladder and 18F-FDG–loaded urine at the bottom was also seen (Fig. 1B). We noted that the urinary bladder was full during scanning. Both patients had clear symptoms of urinary tract infection. The urine was cloudy and had elevated urinary epithelial cell counts, red blood cell counts, white blood cell counts, and total protein content. Urine analysis was also positive for bacteria and fungus. The relevant features are summarized in Table 1.
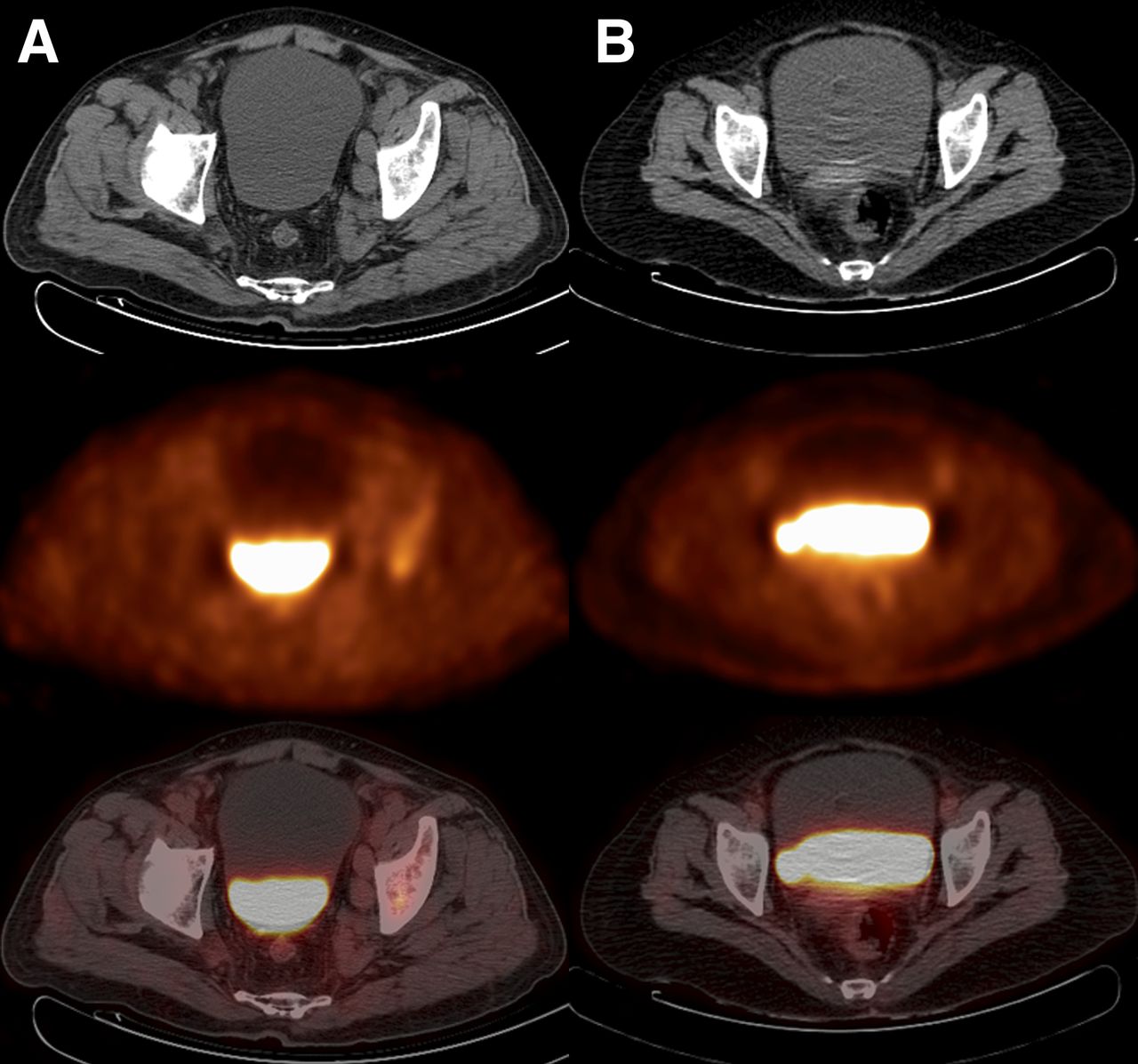
CT (top), PET (middle), and PET/CT (bottom) images showing layering of 18F-FDG in bladder. (A) A 63-y-old woman with T1 pathologic fracture and urinary tract infection. (B) A 67-y-old man with widespread bone and lymph node metastases from unknown primary tumor, also with urinary tract infection.
Clinical and Pathologic Details of the 2 Patients
DISCUSSION
Several examples of layering within the urinary bladder have been reported (3–5). Carrington et al. described a characteristic appearance on CT, with urine that contains contrast medium and has a high specific gravity being layered posteriorly in the dependent portion of the bladder, whereas lower-specific-gravity, nonopacified urine is layered at the uppermost part of the bladder (3). Another study showed that anterior layering of excreted 18F-FDG in the bladder is commonly observed on PET/CT scans obtained with intravenous iodinated contrast material and is due to displacement of 18F-FDG by excreted iodinated contrast material with higher specific gravity (5).
However, the 2 patients in our study did not undergo CT or MR imaging examinations before the PET/CT evaluation, and the urine did not contain contrast medium. Both had a urinary tract infection, and this might have caused the layering phenomenon. The metabolically active cellular components of the urine, such as inflammatory cells, bacteria, and fungi, take up excreted 18F-FDG in the urine for their metabolism, and these cells settle to the bottom of the bladder because of gravity during PET scanning, when a patient lies supine for some time (4). Some patients do not empty the bladder before scanning. The bladder already contains a considerable amount of urine with metabolically active cells and subsequently receives 18F-FDG–loaded urine during scanning. We found that the urinary bladders of our 2 patients were full during scanning. In a distended bladder, delayed mixing of 18F-FDG excretion with nonradioactive urine causes the layering. Moreover, PET/CT images of patients with an empty urinary bladder may help in further interpreting this phenomenon, as settling seems to be better visualized in a full bladder.
To the best of our understanding, there was no standard explanation for settling of 18F-FDG in the urinary bladder that may have alerted the clinicians to check more carefully for lesions on or near the bladder. We may infer that urinary tract infection and a distended bladder are capable of inducing urine layering; however, a 100% cause-and-effect relationship could not be established because of the limited number of cases and the limited information. A definitive explanation needs to be sought with a larger prospective study involving systematic analysis of urine, bladder volume, bladder pressure, and specific gravity in patients with layering, compared with those without layering.
CONCLUSION
These 2 cases illustrate the interesting layering of 18F-FDG in the bladder, the causes of which might be urinary tract infection and a distended bladder; however, the mechanism needs to be further investigated in a more comprehensive study. Moreover, if settling of 18F-FDG in the urinary bladder is seen on imaging, this finding should be reported with the aim of alerting clinicians to look at the urine more carefully. All shades of clinical presentations are possible.
DISCLOSURE
This study was supported by the National Natural Science Foundation (grants 81271532, 81171456, and 30900378) and by Fundamental Research Funds for the Central Universities (project 2015SCU04B09). No other potential conflict of interest relevant to this article was reported.
Footnotes
Published online Dec. 23, 2014.
REFERENCES
- Received for publication August 31, 2014.
- Accepted for publication October 27, 2014.





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.