


Abstract
Leptomeningeal carcinomatosis is an uncommon manifestation of non–central nervous system (CNS) metastatic disease. Diagnosis, however, has important prognostic and treatment implications. We present a case in which intracranial leptomeningeal carcinomatosis from a primary breast cancer was detected with 18F-FDG PET/CT, despite its low sensitivity for detection of CNS metastases from non-CNS primary tumors.
Leptomeningeal carcinomatosis (LC) is an uncommon late manifestation of non–central nervous system (CNS) solid malignancies. 18F-FDG PET/CT has a low sensitivity for detection of CNS metastases from non-CNS primary tumors (1). 18F-FDG PET/CT detection of LC from other non-CNS primary tumors has been described (1), and a few cases of 18F-FDG PET/CT detection of spinal LC from breast cancer (2,3) have been reported. To our knowledge, however, this is the first reported case of intracranial LC from breast cancer detected with 18F-FDG PET/CT.
CASE REPORT
A 38-y-old woman with stage IV inflammatory ductal carcinoma of the breast metastatic to the bones presented with ataxia 2 wk after completion of palliative chemotherapy. Contrast-enhanced brain MR imaging demonstrated nodular leptomeningeal enhancement primarily of the cerebellar folia (Fig. 1). A differential diagnosis of LC versus infectious meningitis was provided. A total of 4 cerebrospinal fluid (CSF) samples were negative for infection and metastatic disease.
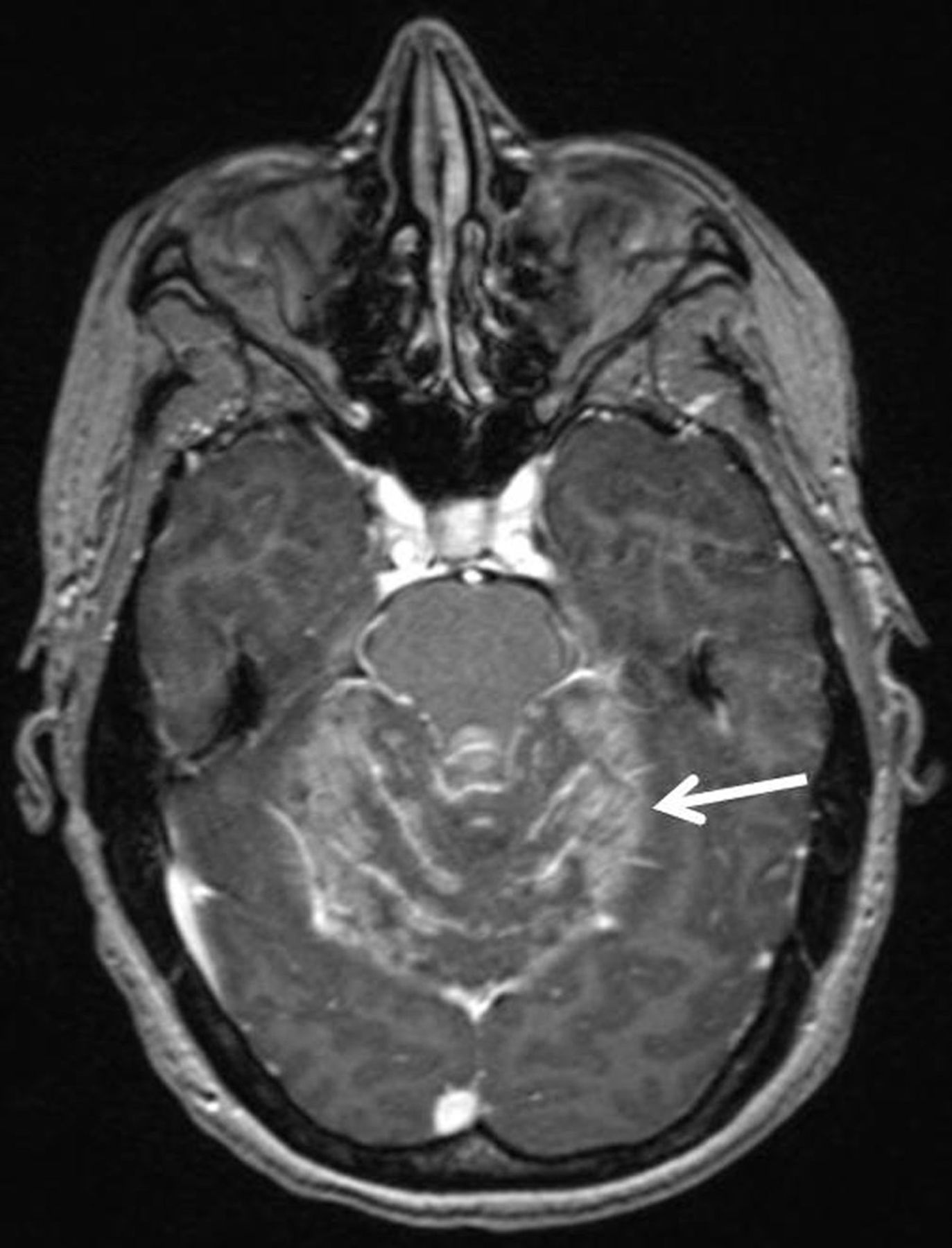
Postcontrast axial T1-weighted image of brain demonstrating leptomeningeal enhancement of cerebellar folia (arrow).
18F-FDG PET/CT was performed for restaging purposes. Imaging from the skull vertex through the mid femora was begun 90 min after intravenous injection of 384 MBq of 18F-FDG. Imaging revealed increased 18F-FDG avidity conforming to the sites of leptomeningeal enhancement on brain MR imaging, as well as progression of osseous metastatic disease (Fig. 2). Despite negative CSF cytology results, the presence of other metastatic disease detected on 18F-FDG PET/CT and a lack of infectious symptoms supported a diagnosis of LC. Neurologic symptoms rapidly regressed after placement of a ventriculostomy and initiation of high-dose steroids and intrathecal chemotherapy.
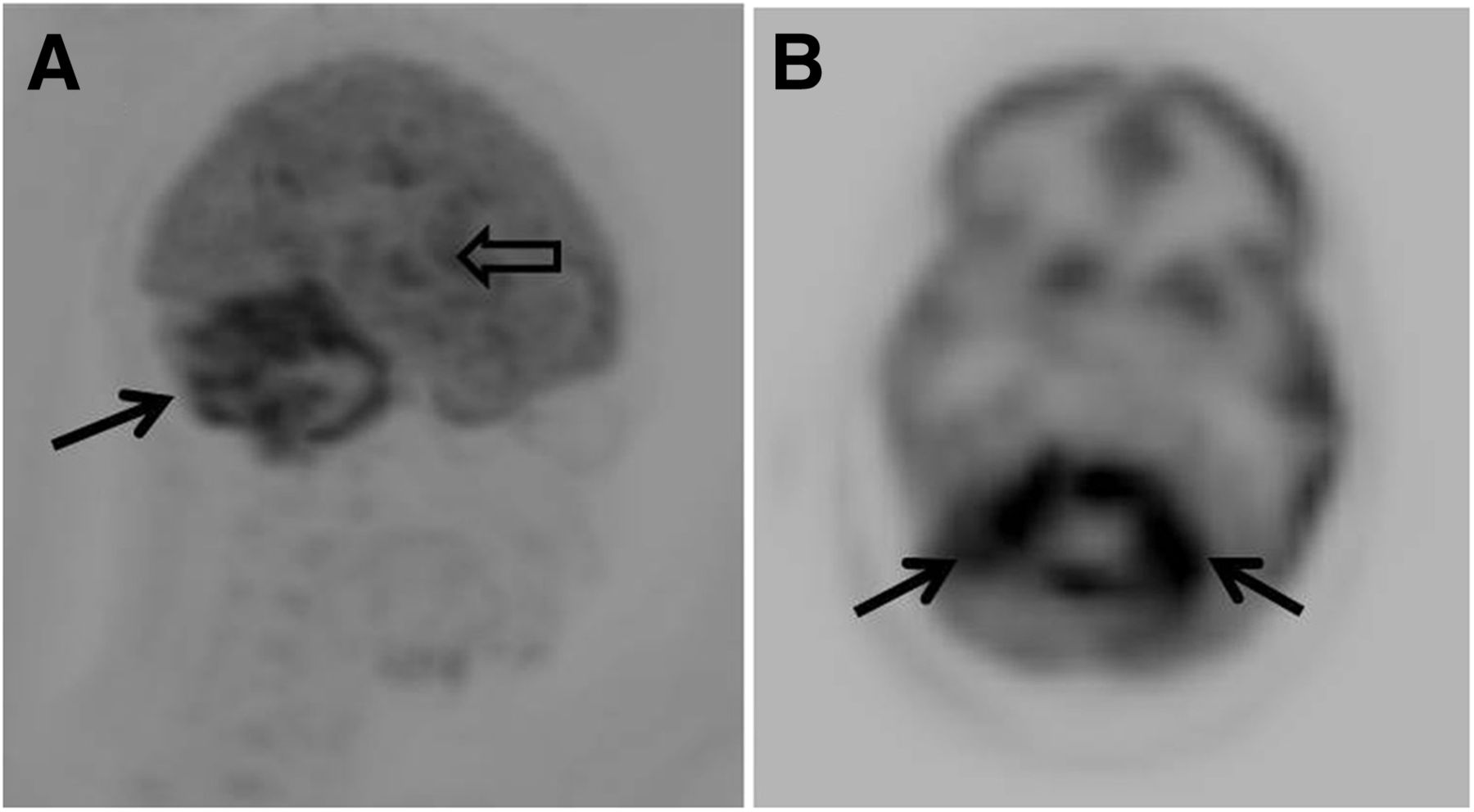
Maximum intensity projection (A) and axial image (B) from 18F-FDG PET showing increased leptomeningeal radiotracer uptake in cerebellum (solid arrows) and temporal lobe (open arrow).
DISCUSSION
The most common intracranial locations of CSF tumor seeding are the basilar cisterns and cerebellum. Although breast cancer is the most common nonhematologic tumor with leptomeningeal spread, the incidence remains low at only 1%–5% (4,5). LC has a poor prognosis, with median survival of only 2–4 mo (2).
Detection of metastatic cells within the CSF remains the gold standard for diagnosis, but the yield is poor, with detection rates of only 50% on initial CSF sampling (4). Contrast-enhanced MR imaging is the imaging modality of choice for diagnosis showing leptomeningeal enhancement. Despite its low sensitivity, 18F-FDG PET/CT may show increased leptomeningeal metabolic activity (1).
Leptomeningeal enhancement and increased 18F-FDG avidity are both nonspecific findings and can be seen in infectious meningitis, LC, or neurosarcoidosis. In conjunction with clinical information, however, they can suggest the diagnosis of LC. Although MR imaging is likely more sensitive in detecting LC, whole-body 18F-FDG PET/CT has the advantage of demonstrating other metastatic disease, an important finding because LC is usually a late manifestation of metastatic disease and less commonly seen in isolation (5).
CONCLUSION
Although the sensitivity of 18F-FDG PET/CT for detection of CNS metastases is poor, routine staging examinations cover the most common locations of intracranial leptomeningeal metastases. Detection is therefore possible and has important prognostic and treatment implications. Although MR imaging is the imaging modality of choice for diagnosing leptomeningeal metastasis, whole-body 18F-FDG PET/CT is uniquely able to detect other systemic metastatic disease, important information supporting a diagnosis of LC.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Feb. 5, 2015.
REFERENCES
- Received for publication September 19, 2014.
- Accepted for publication November 13, 2014.





{kind=link}
{kind=link}