


Abstract
The goal of this study was to evaluate the diagnostic accuracy, cost-effectiveness, and appropriate use of SPECT myocardial perfusion imaging (SMPI) versus stress echocardiography in the preoperative evaluation of patients for kidney transplantation. Methods: A single-institution, retrospective study was performed. SMPI was performed with regadenoson and stress echocardiography predominantly with dobutamine. Findings on subsequent coronary angiography were correlated. A cost analysis for SMPI versus stress echocardiography was modeled using reimbursements from the Center for Medicare Services. Results: One hundred thirteen patients underwent imaging (53 SMPI and 60 stress echocardiography). One hundred percent of SMPI studies were diagnostic, compared with only 80% (48/60) in the stress echocardiography group, and this result was statistically significant (χ2 = 7.96, P < 0.01). The most common reason for a nondiagnostic test was not reaching the target heart rate. In the SMPI group, 15% (8/53) of patients had ischemia on imaging and all underwent subsequent coronary angiography, which confirmed obstructive coronary lesions. One patient with a negative SMPI result underwent a subsequent angiogram that was negative. In the stress echocardiography group, 5% (3/60) of patients had ischemia on imaging and 2 underwent subsequent angiography, which was negative. Three of 12 patients with nondiagnostic examinations underwent further testing. One patient underwent a follow-up positive SMPI scan but no subsequent coronary angiography. The other 2 patients underwent coronary angiography, which was negative. Of the 45 negative stress echocardiography patients, 6 (13%) underwent angiography, with a positive result for obstructive coronary artery disease in 3 of 6. For the modeling of cost analysis, rates of $1,173 and $1,521 (Center for Medicare Services) were used for SMPI and stress echocardiography, respectively. The model assumed that all nondiagnostic imaging would be referred for further stress testing (i.e., nondiagnostic stress echocardiography would be referred for SMPI). This model estimated that initial noninvasive testing with stress echocardiography versus SMPI resulted in a 50% greater cost. Conclusion: For the preoperative evaluation of kidney transplantation, SMPI is more often diagnostic than stress echocardiography. A cost model estimates that initial noninvasive diagnostic testing with stress echocardiography would result in an approximately 50% greater cost than SMPI. Our data also suggest that SMPI has greater diagnostic accuracy than stress echocardiography. Therefore, this single-institution experience supports SMPI as the more appropriate test.
Kidney transplantation candidates represent a unique patient population with often higher than average medical complexity and comorbidity burden. Cardiovascular disease, specifically coronary artery disease (CAD), is a leading cause of morbidity and mortality for this population before and after transplantation. Estimates of the cumulative incidence of myocardial infarction based on Medicare billing claims have ranged from 8.7% to 16.7% by 3 y after kidney transplantation listing and from 4.7% to 11.1% after kidney transplantation between 6 and 36 mo (1,2). The surgery for kidney transplantation is typically considered an elevated-risk procedure and cardiac-risk stratification is warranted to identify patients who are at increased risk for perioperative cardiac events due in part to the pathophysiology of end-stage renal disease. Cardiac evaluation practices vary among institutions and clinicians. The Clinical Practice Guidelines published in 2012 by the American Heart Association and the American College of Cardiology aimed to provide the framework in which to conduct perioperative cardiac assessment, cardiovascular risk prediction, and treatment algorithm in the most recent version of the American Heart Association/American College of Cardiology scientific statement Cardiac Disease Evaluation and Management Among Kidney and Liver Transplantation Candidates (3).
The value of cardiac screening for myocardial ischemia is to identify those likely to benefit from revascularization or optimization of medical management. Even though there is no strong evidence for or against cardiac screening of asymptomatic patients, the current consensus justifies screening based on the presence of multiple CAD risk factors, regardless of stratification by functional status as assessed by estimated metabolic equivalents of task (3). Relevant risk factors include advanced age, diabetes mellitus, prior cardiovascular disease, more than 1 y on dialysis, left ventricular hypertrophy, age greater than 60 y, smoking, hypertension, and dyslipidemia (Class IIb; Level of Evidence C).
Methods of screening vary from exercise or pharmacologic stress nuclear myocardial perfusion imaging to exercise or pharmacologic stress echocardiography and direct cardiac catheterization with coronary angiography without preceding noninvasive testing. Noninvasive stress testing is reported as the most common first approach to cardiac evaluation (4). Prospective randomized controlled trials are not available on optimal screening strategies for the presence of clinically or physiologically significant CAD to guide the approach and choice of a perioperative cardiac imaging modality. For patients who cannot exercise, there are currently no randomized controlled trials comparing different pharmacologic stress-testing methods. In light of insufficient data, local expertise in performing stress testing, patient-specific factors, and specific clinical questions should be considered in decisions about the most appropriate diagnostic test. Both nuclear myocardial perfusion imaging with SPECT and stress echocardiography can reliably detect stress-induced myocardial ischemia, myocardial viability, and CAD (3). The established sensitivity and specificity for detecting angiographically defined CAD (≥50% luminal diameter reduction) are roughly comparable between the 2 established modalities. Sensitivity for SPECT versus stress echocardiography has been shown in various studies to be 85%–90% versus 75%–80% and specificity 65%–70% versus 80%–85%, respectively (5–12). More important, in a recent meta-analysis, echocardiographic and nuclear perfusion imaging are equivalent for the diagnosis of inducible ischemia, with a negative predictive value of 98% for adverse cardiovascular outcomes over the next 3 y (13). Therefore, the invariably high prognostic value of a negative result validates the essential role of nuclear myocardial perfusion imaging and stress echocardiography in cardiac risk stratification as an initial screening modality for CAD.
The paucity of literature directly comparing various methodologies for cardiac stress testing in the preoperative evaluation for kidney transplantation population is the motivation for our investigation. At our institution, a regionally accredited abdominal transplantation center, all patients undergoing preoperative evaluation for kidney transplantation are routinely imaged for CAD with either SPECT myocardial perfusion imaging (SMPI) or stress echocardiography. Our professional and technical staff members have similarly high expertise in performing and interpreting both modalities. This multidisciplinary investigation was undertaken as a quality initiative study, with the participation of team members from medical imaging, cardiology, and abdominal transplantation. We set out to perform a direct comparison by systematically evaluating the diagnostic performance, economics, safety, and appropriate use of SMPI versus stress echocardiography in the kidney transplantation population. In addition, a hypothetic cost-per-patient model was created to reflect the cost-effectiveness of one modality compared with the other.
MATERIALS AND METHODS
Study Design and Patient Population
A single-institution, retrospective study was performed. The institutional review board approved this study, and the requirement to obtain informed consent was waived. Data were collected on all consecutive patients with end-stage renal disease who were evaluated for kidney transplantation from 2012 to 2014. All patients had been entered into a prospectively maintained database after initial consultation with a transplant surgeon or transplant nephrologist. One hundred ninety-eight patients were analyzed. Data included age, sex, cardiac risk factors, medical comorbidities, and cardiac imaging results with any reported adverse events. Cardiac risk factors including advanced age, prior history of CAD, diabetes mellitus, hypertension, dyslipidemia, peripheral vascular disease, cerebrovascular disease, family history of early CAD death, and duration of dialysis were documented. A complete chart review was performed on each patient via the electronic health record. Physician documentation of the history and physical, hospitalization record, clinic follow-up visit, and any cardiac adverse event documented were obtained.
Image Acquisition and Data Analysis
All SMPI studies were performed with the pharmacologic agent regadenoson. Stress echocardiography studies were predominantly performed with the pharmacologic agent dobutamine, and a small subset used treadmill exercise. Image acquisition and interpretation methods were in accordance with standard rest–stress protocols. Positive findings of ischemia were correlated with findings on subsequent coronary angiography, as the gold standard of reference. A diagnosis of significant coronary artery stenosis or obstructive lesions was defined as 50% or more luminal diameter narrowing. Two physicians reviewed in a masked manner the results of coronary angiography for concordance with results of SMPI or stress echocardiography. A cost analysis for SMPI versus stress echocardiography was modeled using reimbursement rates from the Center for Medicare Services (14).
Statistical Analysis
Analysis was performed using StatView statistical software (SAS Institute Inc.). Results are presented as mean ± SD. Group comparisons for nominal variables were performed using the χ2 comparison test. Group comparisons for scale variables were performed using the 1-way ANOVA test. All tests were performed using 2-tailed analysis. A P value of 0.05 or less was considered to be statistically significant.
RESULTS
Patient Demographics
One hundred thirteen patients underwent noninvasive cardiac imaging to evaluate for CAD, with 53 SMPI and 60 stress echocardiography (51 dobutamine and 9 treadmill exercise) studies. A relatively homogeneous group was defined, with a study population that did not differ substantially in clinical characteristics. Both groups had similar demographics and cardiac risk factors. For the SMPI cohort, 35 patients were men and 18 were women; the mean age (±SD) was 55 ± 10 y (age range, 35–77 y). For the stress echocardiography group, 30 were men and 30 were women; the mean age (±SD) was 54 ± 10 y (age range, 22–70 y). No patient in either group had active cardiac symptoms. Cardiac risk factors for both groups were comparable with regard to the following: all patients had at least 2 cardiac risk factors, with diabetes being the most common. Specifically, with regard to prior history of CAD, the SMPI group had 9 patients, and the stress echocardiography group had 6 patients. These patients had a documented history of myocardial infarction, angiographic evidence of coronary stenosis, with or without percutaneous coronary intervention or coronary artery bypass grafting. With regard to dialysis dependency, 32 (60%) patients in the SMPI group were on dialysis at the time of kidney transplantation evaluation, whereas 42 (70%) patients in the stress echocardiography group had dialysis-dependent renal failure. Five patients had undergone kidney transplantation, and 5 patients were deceased from non–cardiac-related death at the time of data analysis.
Comparison Between SMPI Versus Stress Echocardiography
One hundred percent of SMPI studies were diagnostic, compared with only 80% (48/60) in the stress echocardiography group, and this result was statistically significant (χ2 = 7.96, P < 0.01). Commensurately, 20% (12/60) of the stress echocardiography examinations were not diagnostic. The most common reason for a nondiagnostic test was not reaching target heart rate (85% maximal age predicted heart rate) in 12 patients.
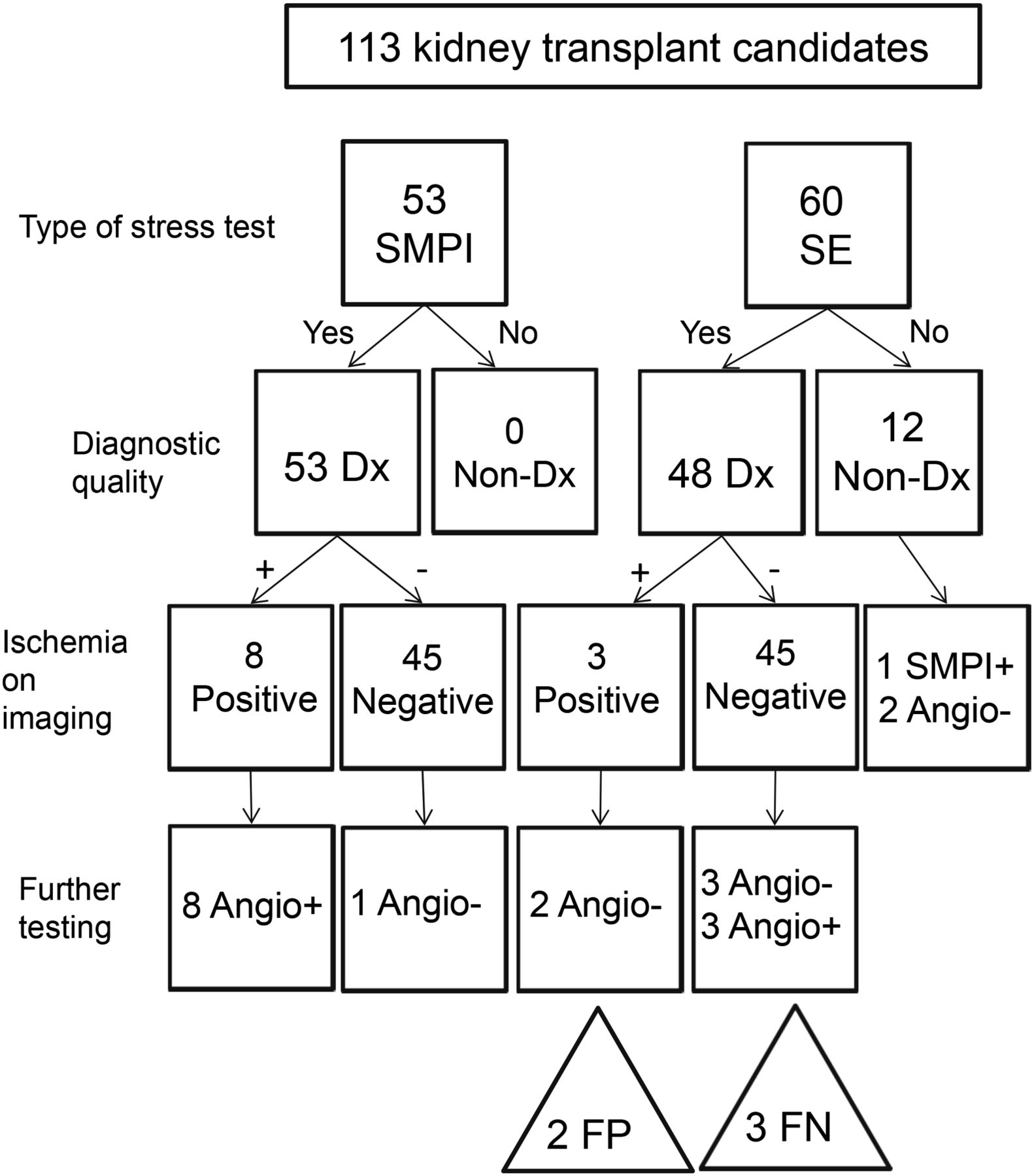
In the SMPI group, 15% (8/53) of patients had ischemia on imaging and all 8 had subsequent coronary angiography, which confirmed obstructive coronary lesions. One patient with a negative SMPI result underwent subsequent angiography, which was negative. In the stress echocardiography group, 5% (3/60) had ischemia on imaging and 2 of 3 patients underwent subsequent angiography, which was negative. Three of 12 patients with nondiagnostic examinations underwent further testing. One patient had a follow-up positive SMPI result but no subsequent coronary angiography. The other 2 patients underwent coronary angiography, which was negative. Of the 45 negative stress echocardiography patients, 6 (13%) underwent angiography, with a positive result for obstructive CAD in 3 of 6 (Fig. 1).

Flow chart of testing for cardiac risk stratification showing breakdown of patients according first to SMPI versus stress echocardiography and then by diagnostic quality and further testing. + = positive; - = negative; Dx = diagnostic; FN = false-negative; FP = false-positive; SE = stress echocardiography.
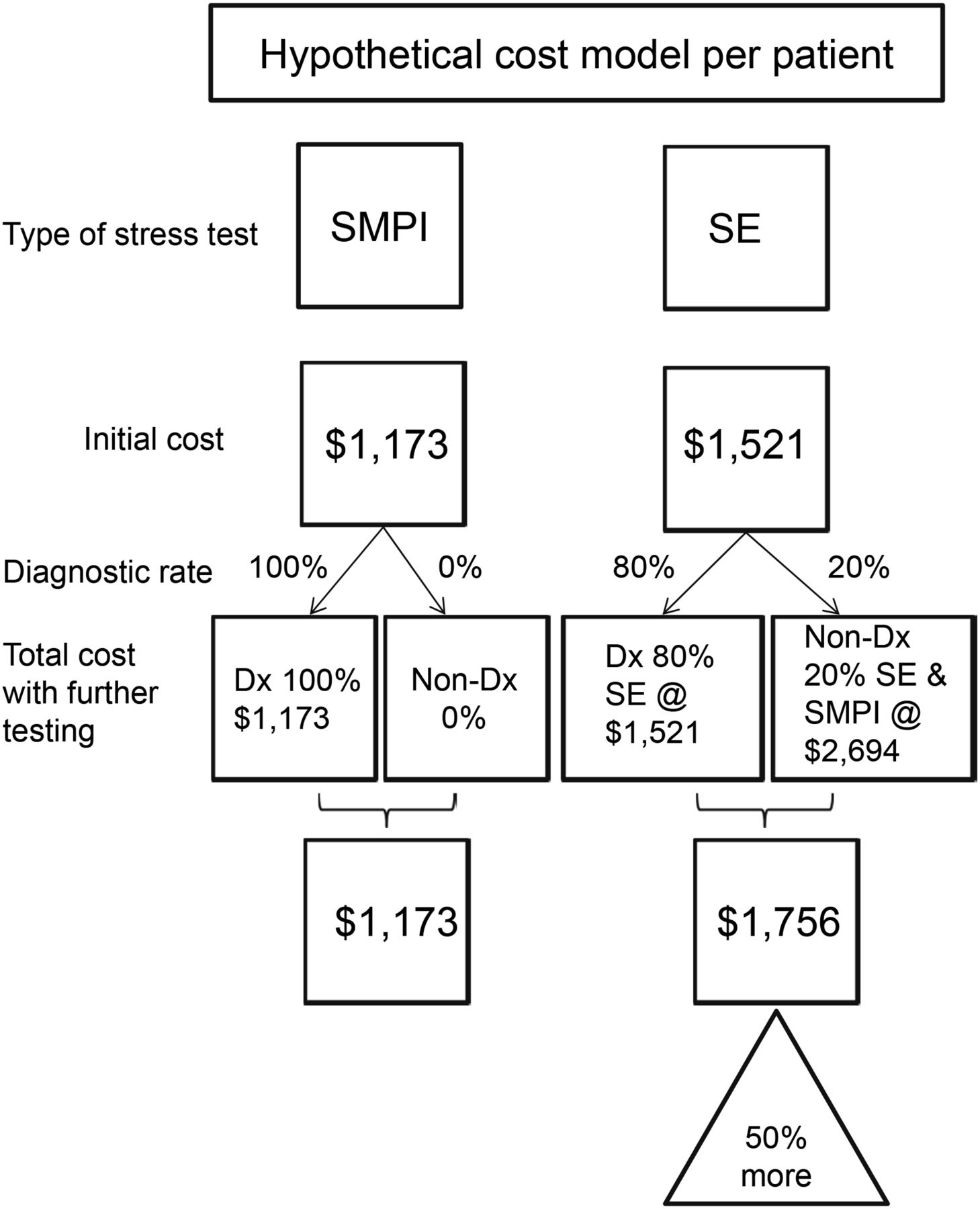
For the modeling of cost analysis, Center for Medicare Services hospital charges for 2014 of $1,173 and $1,521 were used for SMPI and stress echocardiography, respectively (14). The model assumed that all nondiagnostic imaging would be referred for further stress testing (i.e., nondiagnostic stress echocardiography would be referred for SMPI). After data from our institution were input, the model estimated that initial noninvasive testing with stress echocardiography versus SMPI resulted in a 50% greater cost (Fig. 2).
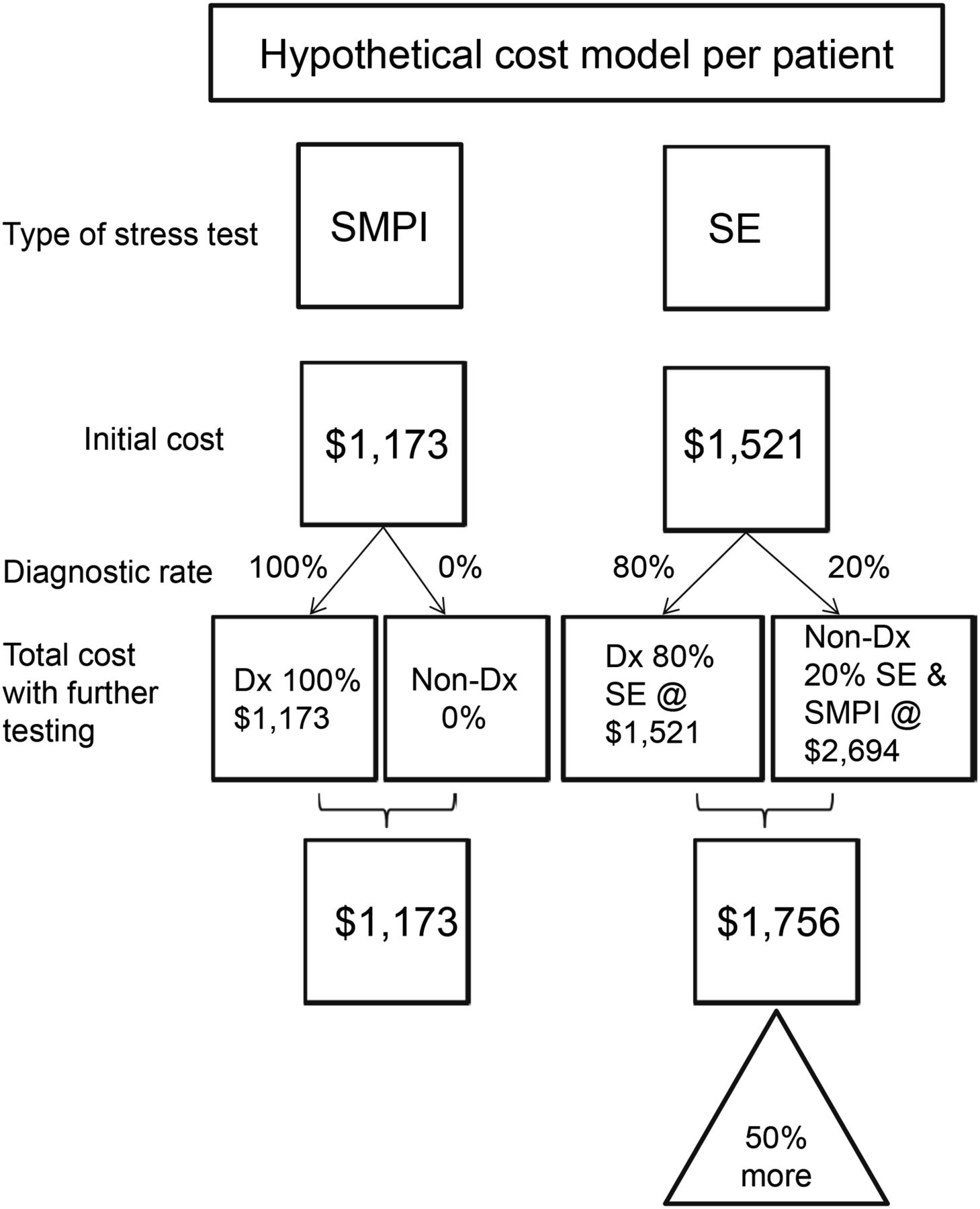
Hypothetic cost model per patient based on Center for Medicare Services hospital charges. Dx = diagnostic; SE = stress echocardiography.
Complications of Procedure
Although not statistically significant, we found that 6% (4/60) of patients who underwent stress echocardiography had a significant transient adverse effect, with 2 necessitating premature termination of the procedure. One case was reported for each of these events: atrial fibrillation, dizziness, shortness of breath, loss of consciousness (nonresponsiveness, which prompted cardiopulmonary resuscitation), and hypertensive urgency with severe headache. Two of these patients had a nondiagnostic test. There were no procedure-related complications in the SMPI group.
DISCUSSION
In this complex, high-risk population, these results support that SMPI with regadenoson is more often diagnostic and more cost-effective than stress echocardiography. Patients undergoing preoperative evaluation for kidney transplantation routinely undergo cardiac stress imaging as part of their preoperative work-up for risk stratification. Commonly, noninvasive stress testing is used first-line, followed by coronary angiography, if indicated. Infrequently, invasive coronary angiography was sought directly without prior noninvasive testing. Because of the lack of randomized controlled trial data comparing different modalities to support an optimal testing approach to preoperative cardiac evaluation, at present this decision-making process is left to the discretion of the referring physician and thus subject to physician’s preference. Ultimately, results of these tests would guide the decision with regard to optimal medical therapy or coronary revascularization in cases of inducible ischemia in the presence of physiologically significant coronary stenosis.
Although myocardial perfusion nuclear imaging and stress echocardiography are both validated methodologies as initial testing modalities for CAD, each technique has its utility, advantages, and limitations. Practical considerations, such as resource availability and use, clinical and technical expertise, and cost constraints, must also be considered when deciding on the best diagnostic approach. This study presented comparative data from our institutional experience with both modalities to guide further testing. A statistically significant difference was found between SMPI and stress echocardiography in the diagnostic rate (100% vs. 80%). Although not statistically significant, SMPI had 100% diagnostic accuracy whereas stress echocardiography was associated with false-positive and false-negative results. A significant adverse event rate was also higher in the stress echocardiography group, when compared with none in the SMPI group. The cost-effectiveness of SMPI versus stress echocardiography was further evaluated with a hypothetic cost model, which estimated that initial noninvasive testing with stress echocardiography versus SMPI resulted in a 50% greater cost. Limitations of this study included small sample size. Also single-institution experience may not be generalizable because of differences in local expertise, technical staff, and equipment. Patient demographics were similar; however, the stress echocardiography group did have more women than men, compared with the SMPI group. An additional limitation is the lack of long-term follow-up and data on clinical outcome.
CONCLUSION
Our single-institution experience showed that, for the preoperative evaluation of kidney transplantation, myocardial perfusion nuclear stress with SPECT (SMPI) is more frequently diagnostic than stress echocardiography and therefore can be modeled to be the more cost-effective initial noninvasive testing for obstructive CAD. Given that our data also show a trend toward greater accuracy of SMPI over stress echocardiography, SMPI does not sacrifice accuracy for cost-effectiveness.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. Phillip H. Kuo is a consultant for GE Healthcare and received grant support from Astellas. Aiden Abidov received grant support from the National Institutes of Health (NIH), Astellas, and GLOBAL and is a consultant for GLOBAL. He is on the advisory board of Advance Cardiac Imaging Consortium (ACIC) and Cardinal Health. No other potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank Amy M. Brewer-Burton for help with the cost benefit analysis.
Footnotes
Published online Jun. 25, 2015.
REFERENCES
- Received for publication April 15, 2015.
- Accepted for publication June 2, 2015.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.