


Abstract
Alzheimer disease and Lewy body dementia are the 2 most common causes of dementia. Each disease has distinctive regional metabolic reduction patterns on 18F-FDG PET. In this report, we present a rare case of an elderly man with dementia whereby 18F-FDG PET clearly showed Lewy body disease with crossed cerebellar diaschisis.
Lewy body disease and Alzheimer dementia may coexist in the same patient and may be difficult to separate clinically or by imaging. Recognition of additional occipital cortex involvement favors the diagnosis of Lewy body disease. In this report, we present a rare case of an elderly man with dementia whereby 18F-FDG PET clearly showed asymmetric Lewy body disease with crossed cerebellar diaschisis.
CASE REPORT
A 71-y-old man with parkinsonism presented with progressively worsening short-term memory loss since 2011. The patient was complaining of motor tics and had been experiencing a decline in multiple domains, including executive functioning, visuospatial functioning, memory, language, attention, and concentration. There was no history of stroke or trauma. The patient had a mini–mental state examination score of 6/30. PET with 18F-FDG was ordered to evaluate for the etiology of the dementia.
After intravenous administration of 540.2 MBq (14.6 mCi) of 18F-FDG, multiple tomographic slices of the brain were obtained. The 18F-FDG PET scan (in quantitative scale with each color step representing 1 SD from the mean [−5.0 to +5.0]) demonstrated decreased radiotracer activity in the left parietal lobe, right parietal lobe, left temporal lobe, and occipital lobes (left greater than right), which is compatible with Lewy body dementia (Figs. 1 and 2). Also, there was decreased radiotracer uptake in the right cerebellum secondary to crossed cerebellar diaschisis (Fig. 3).
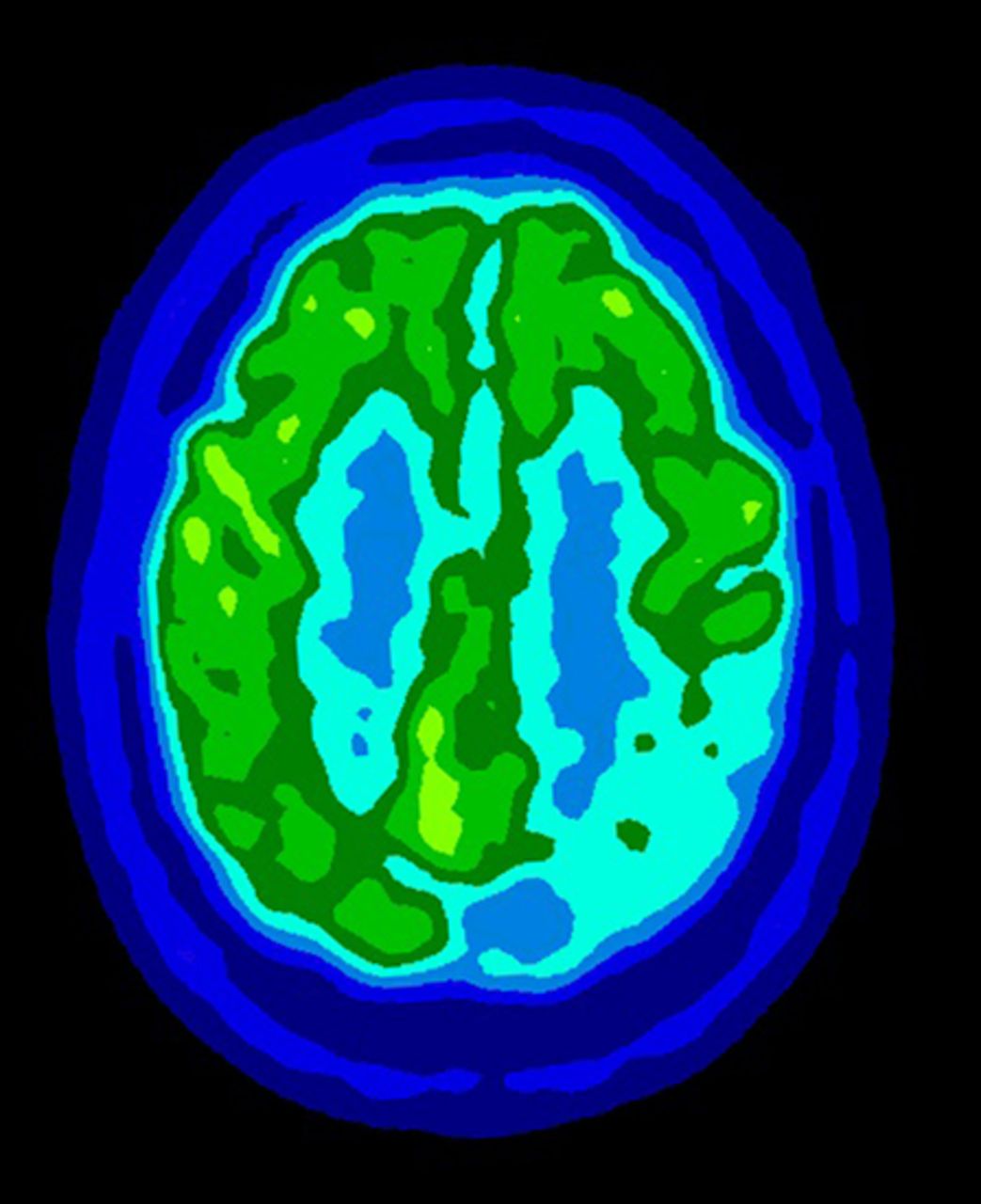
18F-FDG PET scan demonstrating severe decreased radiotracer activity in left parietal lobe and moderately decreased metabolism in right parietal lobe.

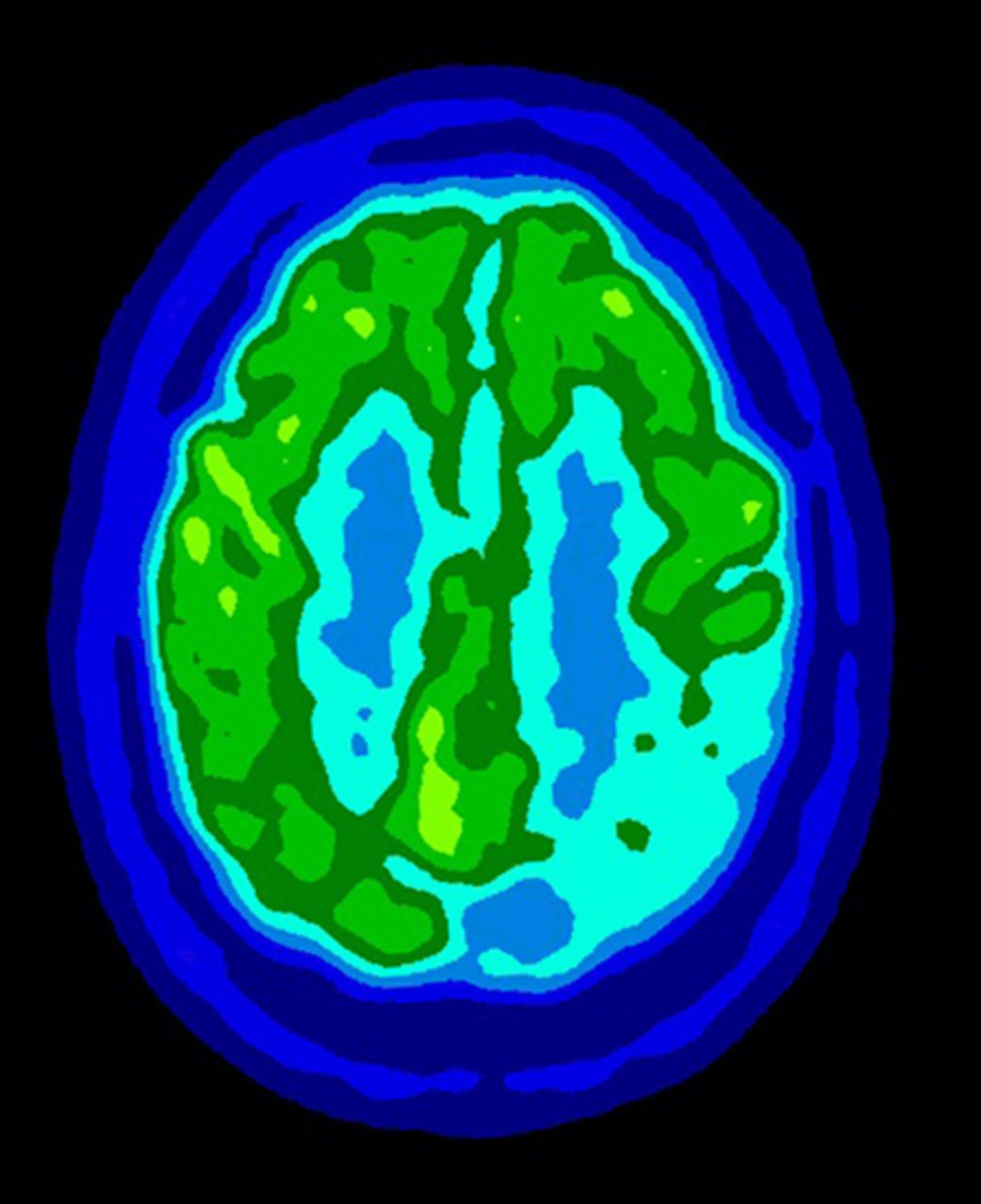
18F-FDG PET scan demonstrating severe decreased radiotracer activity in left temporal lobe and occipital lobes (left greater than right).

18F-FDG PET scan demonstrating crossed cerebellar diaschisis. This image shows mildly reduced metabolism in right cerebellum secondary to crossed cerebellar diaschisis.
DISCUSSION
Lewy body dementia is the second most common cause of dementia after Alzheimer disease. Lewy body dementia manifests as widespread neuronal degeneration. The pathologic etiology centers on deposition of Lewy bodies and Lewy neurites, which contain α synuclein as a major filamentous component (1). The diagnosis of Lewy body dementia is clinical and is based on consensus guidelines (2). In some cases, it is difficult to distinguish between Alzheimer disease and Lewy body dementia clinically, and in these cases the use of noninvasive nuclear imaging such as SPECT or 18F-FDG PET is useful (2). Lewy body dementia and Alzheimer disease have a similar hypometabolic cerebral distribution with marked decreases in association cortices and relative sparing of subcortical structures and primary somatomotor cortex. However, the metabolic reduction in the occipital cortex is the key feature to support the diagnosis of Lewy body dementia (3). The reduced metabolism in the right cerebellum is consistent with diaschisis, which is defined as depression of regional neuronal metabolism and cerebral blood flow caused by dysfunction in anatomically separate but functionally related neuronal regions (4). The mechanism appears to be an interruption of the corticopontine–cerebellar pathway (5). This phenomenon has been associated with Lewy body dementia (2) and with other cortical pathologies, specifically tumor, stroke, or trauma (5).
CONCLUSION
Alzheimer disease and Lewy body dementia are the two most common causes of dementia. Each disease has distinctive regional metabolic reduction patterns on 18F-FDG PET. Therefore, knowing these patterns is important to support the likely diagnosis.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Sep. 4, 2014.
REFERENCES
- Received for publication February 19, 2014.
- Accepted for publication April 8, 2014.





{kind=link}
{kind=link}
{kind=link}