


Abstract
We present a case demonstrating how correlative imaging with 123I-ioflupane SPECT and 18F-FDG PET can be used to help make the diagnosis of Lewy body disease more specific.
This case demonstrates how correlation of 18F-FDG PET with 123I-ioflupane SPECT imaging can help to diagnose Lewy body disease, currently termed neurocognitive disorder with Lewy bodies (1). Lewy body disease is an elusive diagnosis that can be confirmed only at autopsy (2), yet it represents the second most common type of neurocognitive disorder, behind Alzheimer disease (3). The following case illustrates how molecular imaging techniques can help increase the certainty of the diagnosis.
CASE HISTORY
An 82-y-old man presented with progressive memory loss and decline in function that had started 6 mo beforehand. He was no longer able to perform activities of daily living and was restricted from driving.
A neuropsychologic work-up revealed mild depression with significant cognitive decline, including severe deficits in recall, attention, problem solving, object recognition, spatial reasoning, insight, and semantic fluency, as well as dressing dyspraxia. He complained of bilateral hand tremors (right > left) but denied hallucinations. The overall findings were suggestive of multifactorial dementia; however, the rapid progression of symptoms was initially suspected to be due to metabolic encephalopathy. Blood work showed a normal vitamin B12 level, no heavy metals, and no treponemal antibody. An MR imaging and MR angiography study from an outside institution had unremarkable findings.
A brain PET study was performed to evaluate for Alzheimer disease versus frontotemporal dementia. PET/CT was performed with concurrent CT for attenuation correction after injection of 388 MBq (10.5 mCi) of 18F-FDG. The patient was allowed a 90-min uptake period in a quiet, semidarkened room, with eyes open.
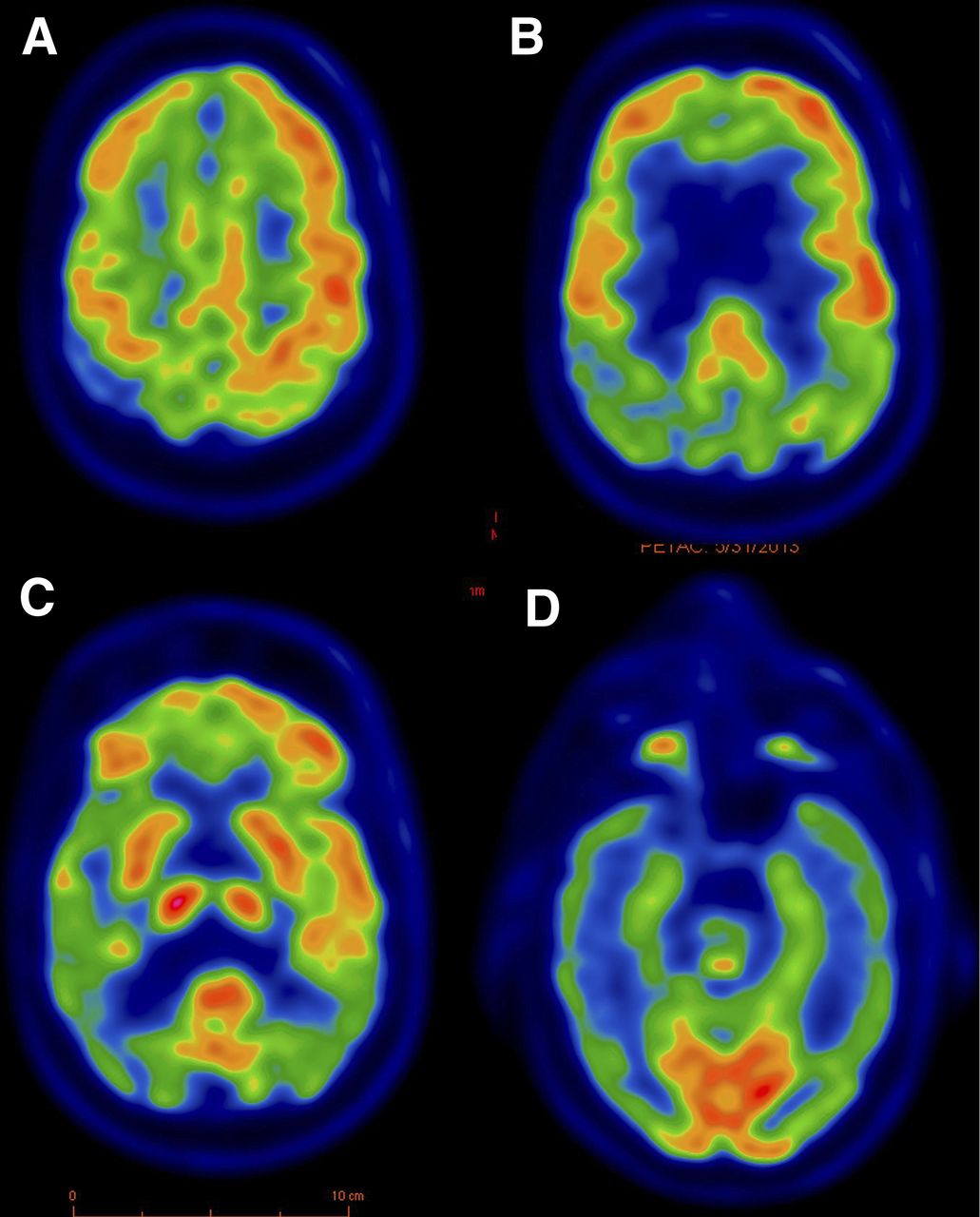
The 18F-FDG PET images (Fig. 1) demonstrated decreased glucose metabolism in the temporal and parietal lobes, slightly worse on the right than the left. This pattern is suggestive of Alzheimer disease rather than frontotemporal dementia (4). There was also decreased activity bilaterally in the lateral occipital lobes but with sparing of the primary visual cortex. These findings raised the possibility of Lewy body disease but were not pathognomonic (3,5). A 123I-ioflupane brain SPECT study (Fig. 2) was recommended for confirmation. It was performed using fanbeam collimators 4 h after injection of 159 MBq (4.3 mCi) of 123I-ioflupane. The images demonstrated decreased activity in the putamina and slightly decreased activity in the right caudate nucleus.

18F-FDG PET brain scan is shown in 4 axial slices progressing craniocaudally from A to D. Activity is preserved in frontal lobes (A–C) and basal ganglia (C) but markedly decreased in parietal (B) and lateral occipital lobes (C), worse on right side. Activity is also significantly decreased in temporal lobes but is preserved in primary visual cortex located in medial occipital lobes (D).
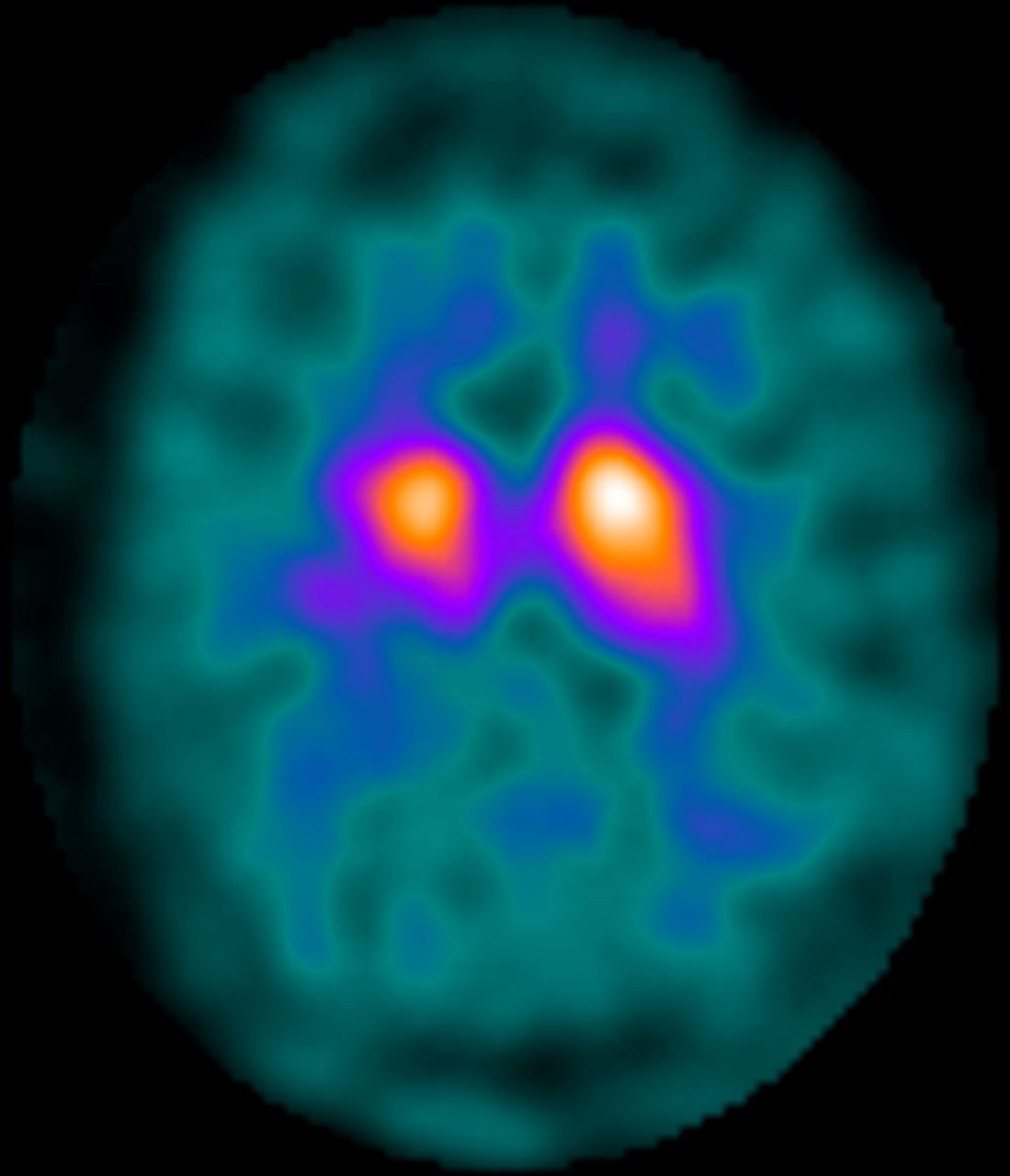
123I-ioflupane SPECT image shows markedly decreased uptake in bilateral putamina—right worse than left—and decreased activity in right caudate nucleus relative to left.
In light of the patient’s symptoms, and the correlation between the 18F-FDG PET and 123I-ioflupane SPECT results, Lewy body disease could be diagnosed with reasonable certainty (5).
DISCUSSION
At present, 123I-ioflupane imaging is approved in the United States only for differentiation of essential tremor from neurodegenerative movement disorders (Parkinson disease, multiple system atrophy). However, in Lewy body disease 123I-ioflupane uptake is known to be abnormal with high sensitivity (3). Our case illustrates that even with an atypical appearance on 18F-FDG PET, correlation with 123I-ioflupane would make one much more comfortable in stating that the findings are consistent with Lewy body disease.
Lewy body disease is difficult to diagnose clinically because of a variable clinical presentation. The disease may include motor features of Parkinson disease (shuffling gait, low speech volume, cogwheel movements, and blank expression) but more typically presents with cognitive impairments resembling Alzheimer disease. The only differentiating feature is the presence of visual hallucinations, which are reported in approximately two thirds of the patients (2).
Consideration of the pathophysiology explains the pattern on 18F-FDG PET and 123I-ioflupane SPECT. Lewy body disease causes dysfunction of the basal ganglia, partially through denervation of the dopaminergic neurons in the striatum, which in turn causes decreased uptake of 123I-ioflupane because of decreased availability of the dopamine transporters (2,5). However, glucose metabolism in the basal ganglia remains intact, hence the normal uptake on 18F-FDG PET. Although all neurodegenerative movement disorders appear similar on 123I-ioflupane scanning, they can be differentiated by clinical symptoms. Additionally, there is evidence that each disorder may have its own characteristic appearance on 18F-FDG PET (6).
Lewy body disease also causes loss of the acetylcholine-producing neurons, which brings about significant cognitive impairment in a process similar to Alzheimer disease (2). This similarity explains why both Lewy body disease and Alzheimer disease have temporal-parietal deficits on 18F-FDG PET (4–6). The visual hallucinations of Lewy body disease are likely a manifestation of decreased glucose metabolism involving the visual cortex.
CONCLUSION
Combined molecular imaging with 123I-ioflupane SPECT and 18F-FDG PET can be a highly specific tool for differentiating Lewy body disease from Alzheimer disease—conditions that previously have been difficult to definitively diagnose.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Jul. 17, 2014.
REFERENCES
- Received for publication September 25, 2013.
- Accepted for publication December 17, 2013.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.