


Article Figures & Data
Figures
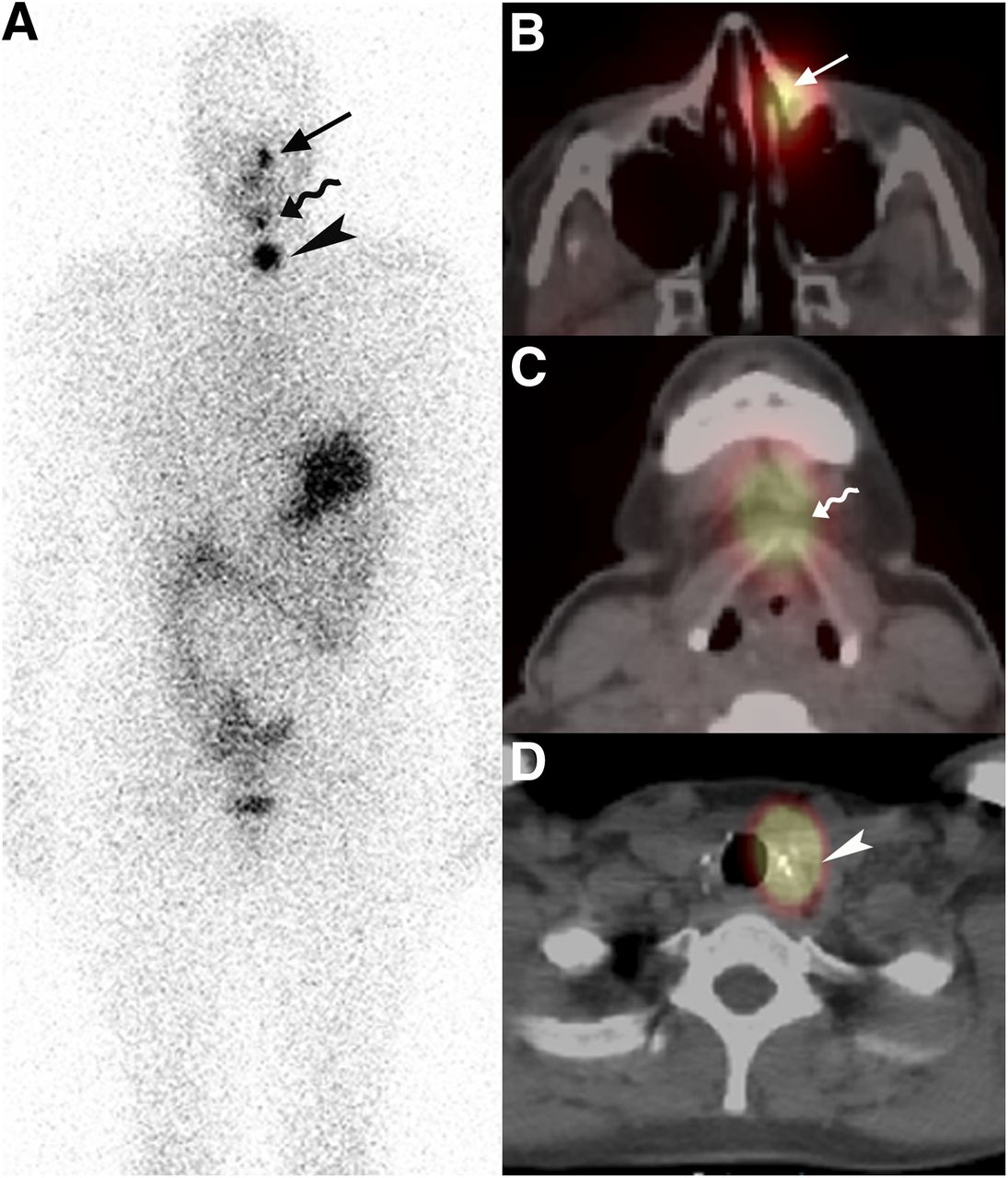
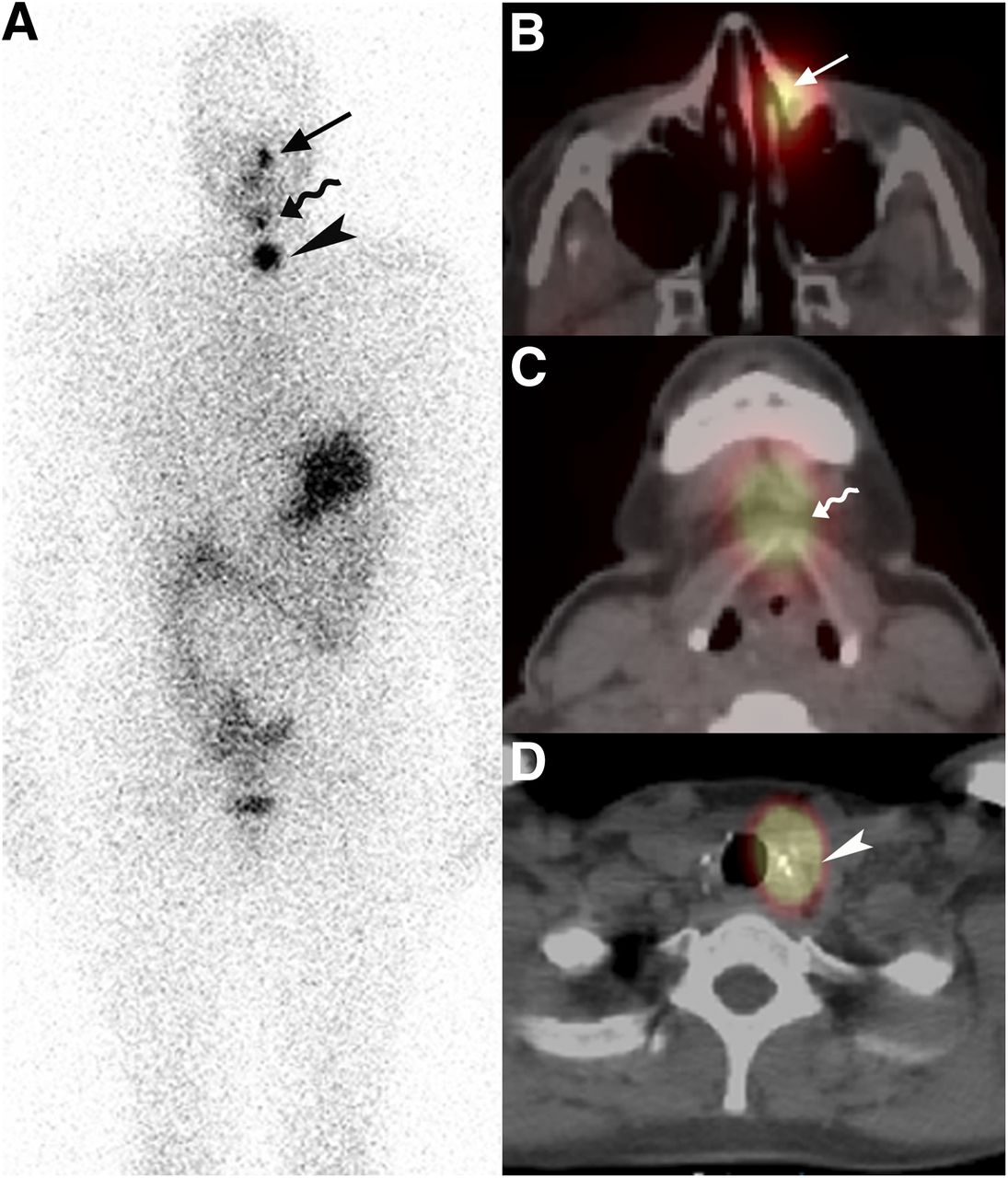
- FIGURE 1.
Diagnostic 131I scan obtained 24 h after oral administration of 37 MBq (1 mCi) of 131I in 37-y-old woman after total thyroidectomy for multifocal papillary thyroid cancer (two 1.1-cm tumors). Patient had stimulated thyroglobulin level of less than 0.5 ng/mL; however, measurement was unreliable because specimen contained antithyroglobulin antibodies. (A) Planar whole-body anterior image demonstrates 3 distinct foci of radioactivity, with most superior focus just left of midline in the face (arrow). Two additional foci of activity are seen in neck (wavy arrow and arrowhead). (B) Correlative axial fused SPECT/CT demonstrates localization of superior focus to nasolacrimal duct (arrow), consistent with benign radioiodine accumulation within lacrimal secretions draining into nasal cavity, excluding metastatic osseous lesion to maxilla. (C) Middle focus is centered at tip of hyoid bone and is consistent with thyroglossal duct remnant (wavy arrow), formed by rests of thyroid cells along thyroglossal duct during embryologic migration of thyroid from base of tongue to its final position in lower neck. This is a commonly encountered normal variant, and SPECT/CT improves characterization compared with planar imaging. (D) Lower focus of activity is located paratracheally in left thyroid bed in close association with surgical clips (arrowhead), consistent with thyroid remnant. Focal paratracheal central neck activity can be characterized as benign thyroid remnant when surgical pathology review demonstrates no evidence of tumor extrathyroidal extension and negative surgical excision margins.
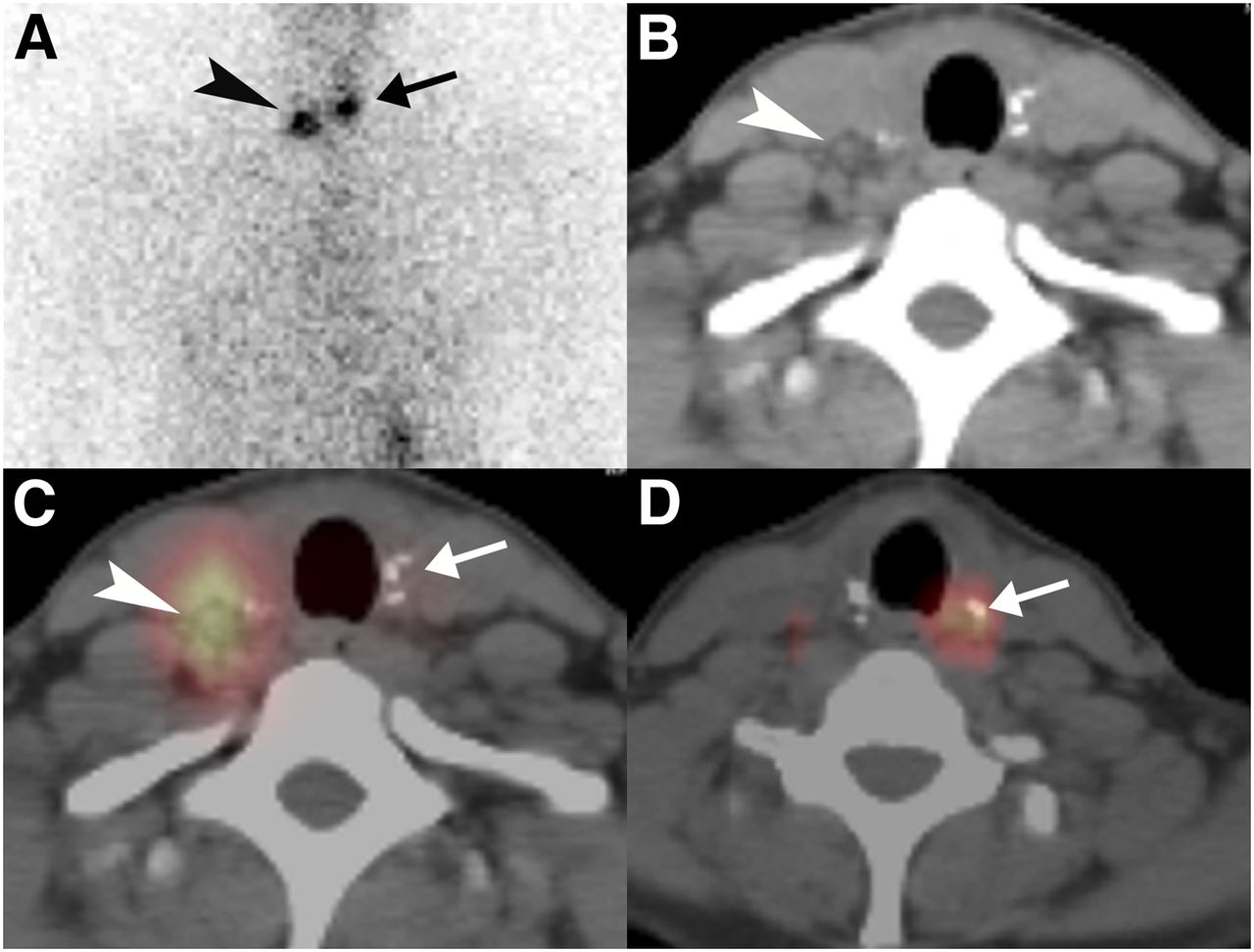
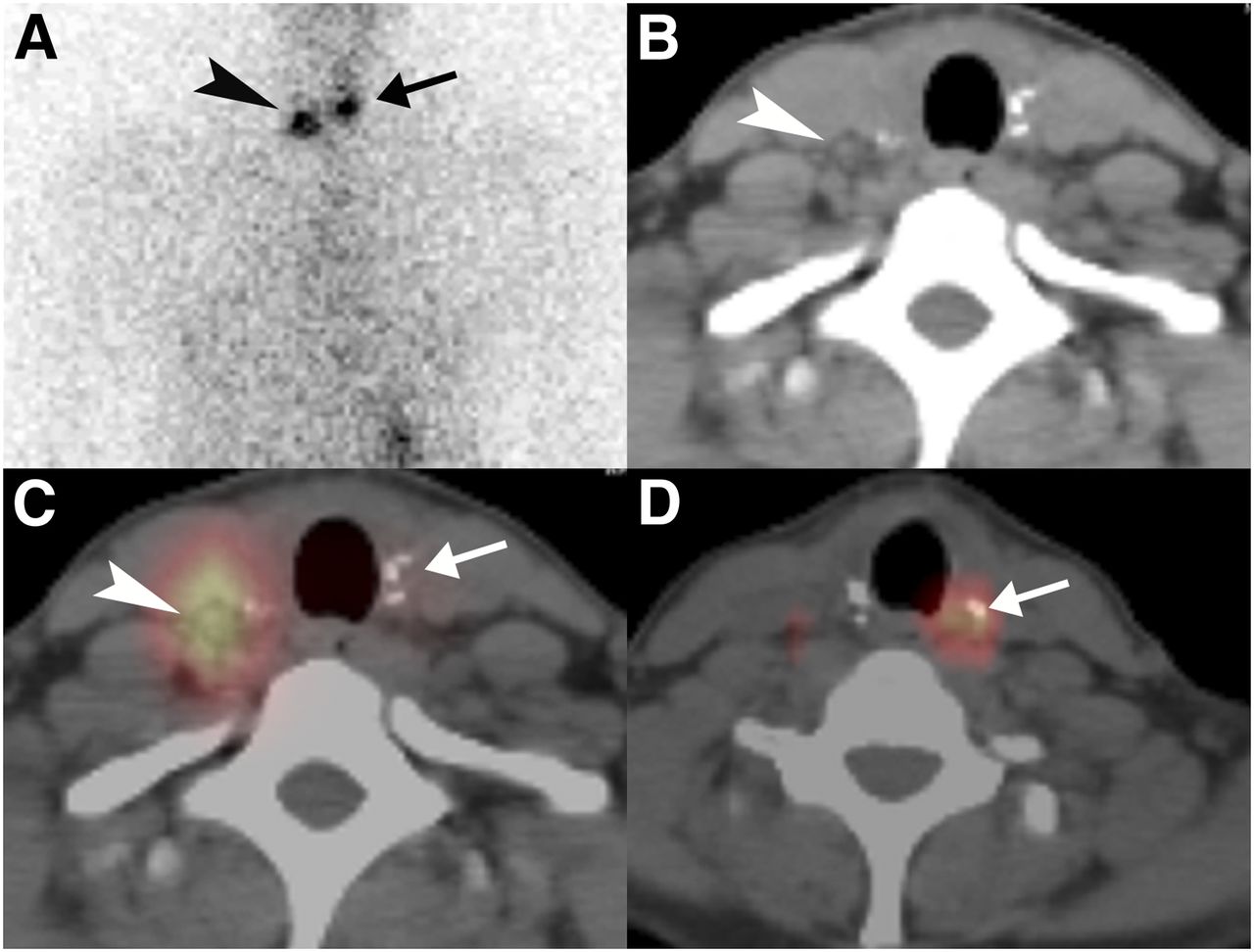
- FIGURE 2.
Diagnostic 131I scan obtained 24 h after oral administration of 37 MBq (1 mCi) of 131I in 36-y-old woman after total thyroidectomy for multifocal papillary thyroid cancer (3.0- and 0.6-cm tumors). Patient’s stimulated thyroglobulin level was less than 0.5 ng/mL; however, measurement was unreliable because specimen contained antithyroglobulin antibodies. (A) Planar static anterior view of chest demonstrates 2 foci of activity, one in left neck (arrow) and the other in right lower neck (arrowhead). (B–D) Correlative axial CT (B) and axial fused SPECT/CT (C and D) localize left neck focus to left thyroidectomy bed in close association with surgical clips (arrow), consistent with thyroid remnant. Right neck focus corresponds to 0.5-cm nodule adjacent to right carotid neurovascular bundle (arrowhead), consistent with nodal metastasis.
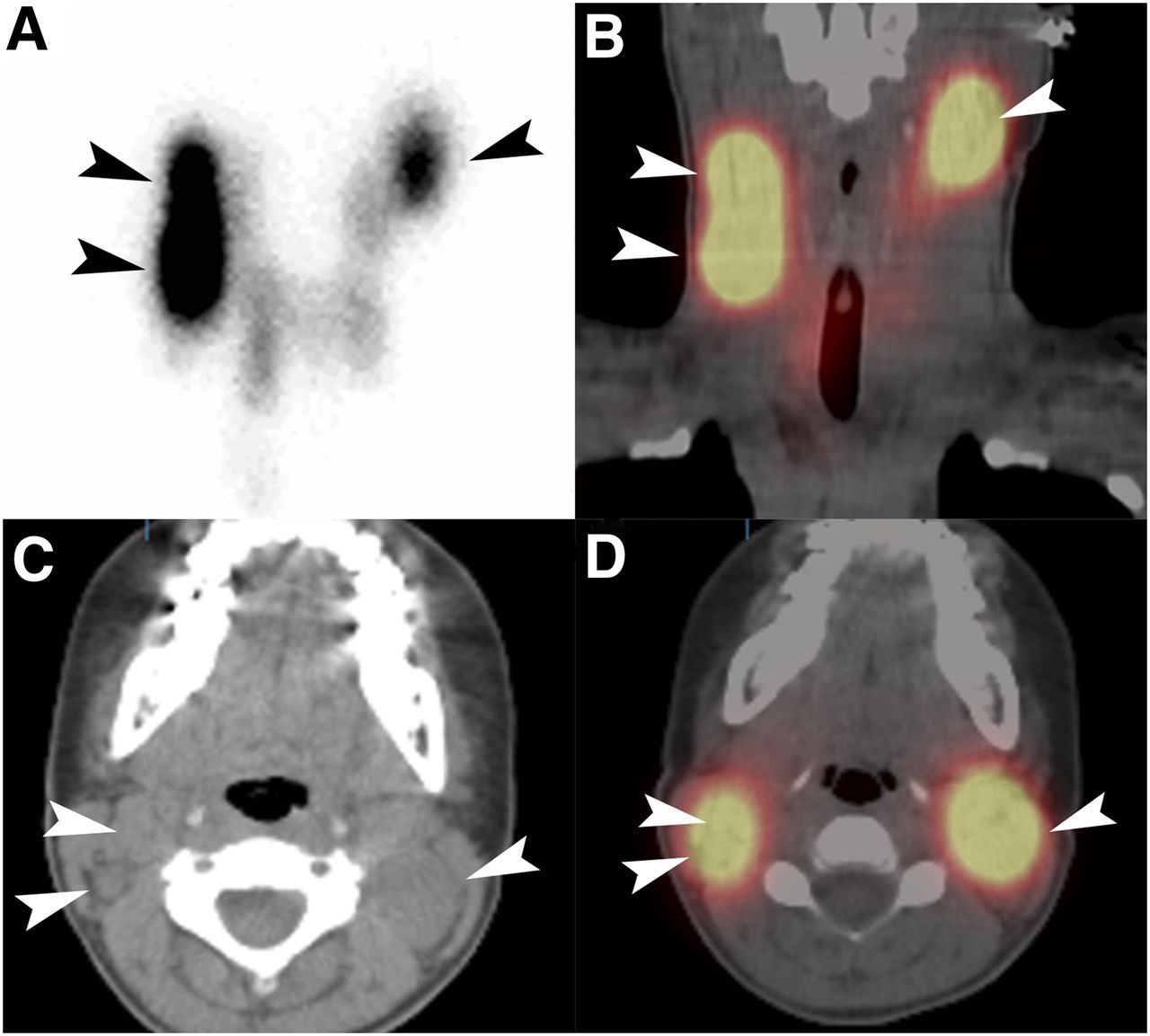
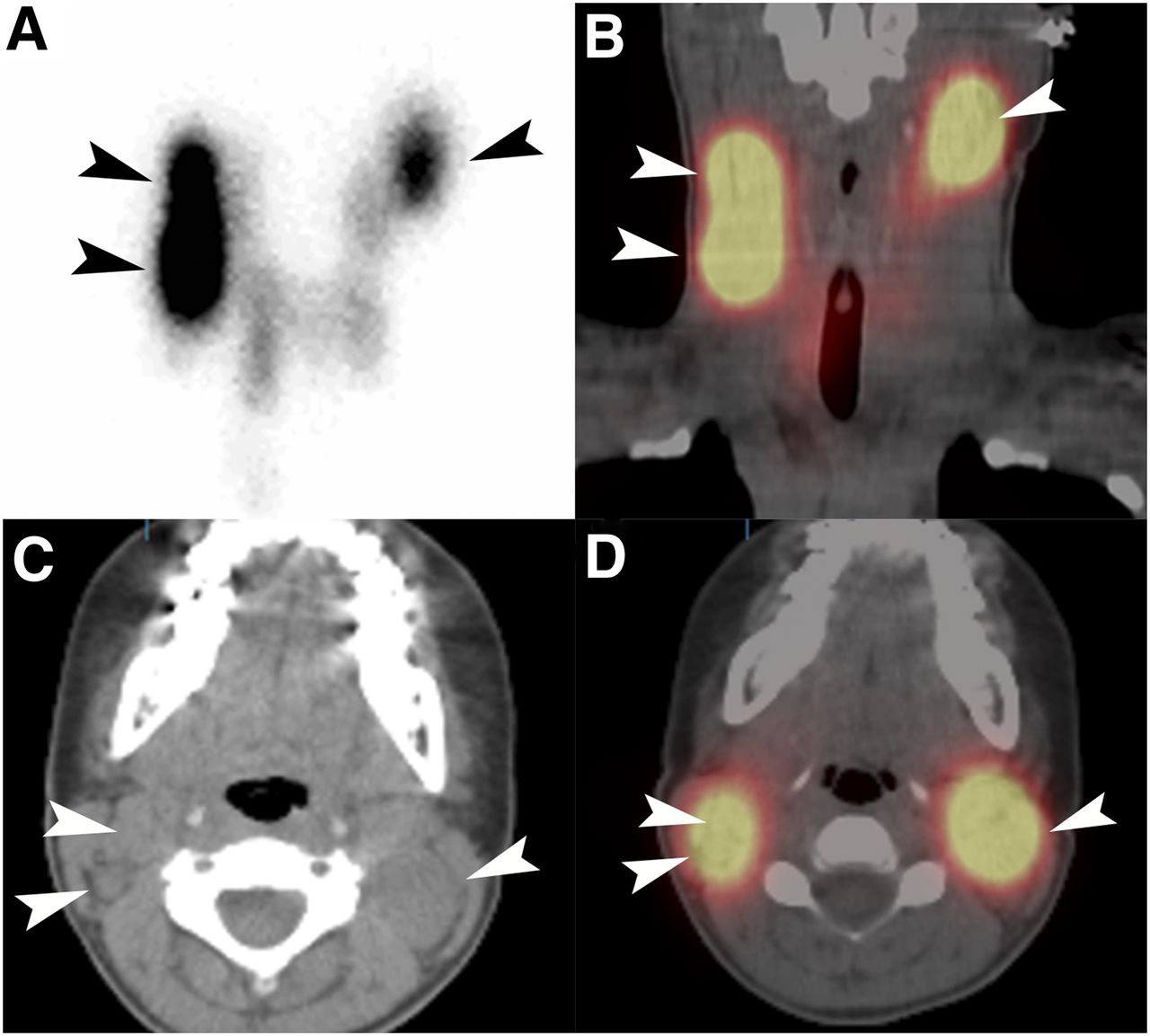
- FIGURE 3.
Diagnostic 131I scan obtained 24 h after oral administration of 37 MBq (1 mCi) of 131I in 14-y-old girl after total thyroidectomy for papillary thyroid cancer extensively involving both lobes and isthmus. Patient’s stimulated thyroglobulin level was 406 ng/mL. (A) Pinhole neck image demonstrates longitudinal intense activity in right neck laterally and focal intense activity in left upper neck; in addition, there are several foci of fainter activity in central neck bilaterally. (C–D) Correlative coronal (B) and axial (D) fused SPECT/CT and axial CT (C) demonstrate conglomerate metastatic lymphadenopathy in right cervical levels IIB and III and left cervical level IIB. Due to residual bulky metastases in bilateral neck as demonstrated on planar diagnostic study and measured on SPECT/CT, the patient was referred for reoperative bilateral neck dissection before proceeding with therapeutic 131I administration.
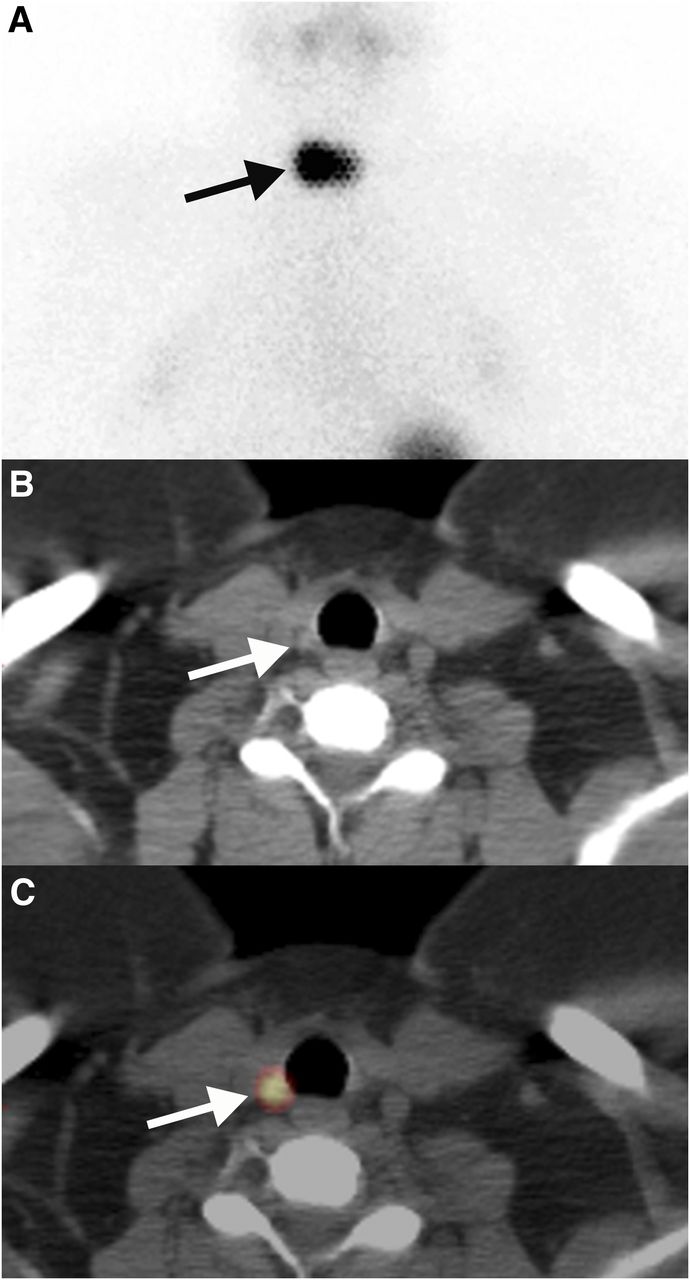
- FIGURE 4.
Diagnostic 131I scan obtained 24 h after oral administration of 37 MBq (1 mCi) of 131I in 37-y-old woman after total thyroidectomy for goiter with incidental papillary thyroid microcarcinoma (1.3-mm tumor; one metastatic of 3 lymph nodes dissected in the central neck compartment). Patient’s stimulated thyroglobulin level was 5.9 ng/mL. (A) Planar static anterior view of chest demonstrates intensely focal central neck activity (arrow). (B and C) Correlative axial CT (B) and axial fused SPECT/CT (C) localizes this activity to 0.4-cm right paratracheal lymph node (arrow) located immediately below cricoid cartilage, consistent with nodal metastasis.
- FIGURE 5.
Diagnostic 131I scan obtained 24 h after oral administration of 37 MBq (1 mCi) of 131I in 54-y-old woman after total thyroidectomy for multifocal papillary thyroid microcarcinoma (5 distinct tumors measuring 0.2–0.4 cm). Patient’s stimulated thyroglobulin level was less than 0.5 ng/mL; however, measurement was unreliable because specimen contained antithyroglobulin antibodies. (A) Planar static posterior view of chest demonstrates multifocal activity within lung fields bilaterally, consistent with pulmonary metastases. (B–D) Correlative axial CT (B) and axial (C) and coronal (D) fused SPECT/CT demonstrate several 0.2- to 0.4-cm iodine-avid pulmonary nodules (arrowheads).
- FIGURE 6.
Axial CT (A and B), fused 131I SPECT/CT (C), and isodose radiation map (D) in 75-year-old man with solitary calvarial metastasis. Total thyroidectomy with resection of multifocal follicular variant papillary thyroid cancer (1.8- and 0.5-cm tumors) and partial parietooccipital resection occurred 10 y previously; however, the patient presented with recurrent metastasis to skull. Whole-body and lesion dosimetry calculations were performed after oral administration of 37 MBq (1 mCi) of 131I. Subsequently, the patient received 7.4 GBq (200 mCi) of 131I therapy; stimulated thyroglobulin was 29,124 ng/mL at time of therapy. (A) Axial CT image demonstrates calvarial metastasis and (B) tumor volumetric measurement of 219 mL obtained with Vitrea2 software, version 4.1.1.0, Vital Images, Inc. (C) Axial fused SPECT/CT image demonstrates focal radioactivity concentration in tumor. (D) CT image with superimposed isodose levels of cGy in tumor (shaded) and brain. Mean radiation dose to tumor was 1,970 cGy, mainly from beta radiation; gamma (photon) radiation emanating from tumor imparted low level radiation to adjacent brain; mean radiation absorbed dose to brain was 35 cGy. (Reprinted with permission of (71).)



Tables
- TABLE 1
AJCC 7th Edition TNM Score for Papillary or Follicular Well-Differentiated Thyroid Cancer (21)
Score Characteristics Primary tumor (T) T1 Tumor ≤ 2 cm, limited to thyroid; T1a: tumor ≤ 1 cm (microcarcinoma);T1b: tumor > 1 cm but ≤ 2 cm T2 Tumor > 2 cm but ≤ 4 cm, limited to thyroid T3 Tumor > 4 cm, limited to thyroid, or any tumor with minimal extrathyroid extension; for example, extension to sternothyroid muscle or perithyroid soft tissues T4 Advanced disease: T4a: tumor of any size extending beyond thyroid capsule to invade subcutaneous soft tissues, larynx, trachea, esophagus, or recurrent laryngeal nerve; T4b: tumor invades prevertebral fascia or encases carotid artery or mediastinal vessels Regional nodes (N) N0 No regional lymph node metastasis N1 Regional lymph node metastasis; N1a: metastasis to central neck compartment (cervical level VI); N1b: metastasis to unilateral, bilateral, or contralateral lateral neck compartments (cervical levels I, II, III, IV, or V) or retropharyngeal or superior mediastinal lymph nodes (cervical level VII) Distant metastases (M) M0 No distant metastasis M1 Distant metastasis Stage T N M Patients < 45 years old Stage I Any T Any N M0 Stage II Any T Any N M1 Patients ≥ 45 years old Stage I T1 N0 M0 Stage II T2 N0 M0 Stage III T3 N0 M0 T1 or T2 or T3 N1a M0 Stage IVA T1 or T2 or T3 N1b M0 T4a Any N M0 Stage IVB T4b Any N M0 Stage IVC Any T Any N M1 T: tumor; N: nodes; M: distant metastases.
ATA Thyroid Cancer Risk Stratification SNM Very low risk Unifocal or multifocal microcarcinomas (< 1cm) √ MACIS score < 6, or TNM score: T1–2, N0, M0 √ In patients < 45 years old: tumors < 4 cm confined to the thyroid √ Excludes tumors with aggressive histology* or vascular invasion √ Low-risk (all criteria must be met) In patients < 45 years old: MACIS < 6, or TNM score: any T any N, M0 √ In patients ≥ 45 years old: MACIS < 6, or TNM score: T2, N0, M0 √ √ No local or distant metastases √ √ All macroscopic tumor has been resected √ √ There is no tumor invasion of locoregional tissues or structures √ √ The tumor does not have aggressive histology* or vascular invasion √ √ If 131I is given, there is no 131I uptake outside the thyroid bed on the first post-therapy scan √ Intermediate/Moderate risk (any criteria) In patients < 45 years old: tumors > 4 cm; macroscopic (> 1cm) N1a or N1b; T1–3, N1b, M0 √ In patients ≥ 45 years old: T3, N0, M0 or T1–3, N1a, M0 √ MACIS score > 6 √ Minimally invasive (microscopic capsular, but not vascular invasion) FTC < 4 cm √ √ Tumor with aggressive histology* or vascular invasion √ √ Microscopic invasion of tumor into the perithyroidal soft tissues at initial surgery √ √ Cervical lymph node metastases, or 131I uptake outside the thyroid bed on the post-therapy scan High-risk (any criteria) In patients < 45 years old: T4a–4b, any N, M0, or any T, any N, M1 √ In patients ≥ 45 years old: any T, N1a–1b, M0, AJCC Stages IVA, IVB, IVC √ FTC > 4 cm, or macroscopic invasive FTC √ √ Distant metastases √ √ Macroscopic tumor invasion √ √ Incomplete tumor resection √ Thyroglobulinemia out of proportion to what is seen on the post-therapy scan *Aggressive histology includes tall cell, insular, columnar, diffuse sclerosing, trabecular solid, poorly differentiated variants of papillary thyroid carcinoma (PTC) and Hürthle cell variant of follicular thyroid carcinoma (FTC); MACIS: Metastases, Age, Completeness of resection, Invasiveness, Size of tumor; staging system developed at Mayo Clinic (16); TNM: Tumor, Nodes, Metastases, staging system developed by AJCC/UICC (21).
Supplemental Data
Files in this Data Supplement:





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
- Article
- Abstract
- ADVANTAGES, DISADVANTAGES, AND LIMITATIONS OF SPECT/CT
- UTILITY OF POST-THERAPY RADIOIODINE SPECT/CT
- UTILITY OF SPECT/CT FOR PROBLEM SOLVING (EVALUATION OF UNUSUAL RADIOACTIVITY DISTRIBUTIONS)
- UTILITY OF DIAGNOSTIC PREABLATION RADIOIODINE SPECT/CT
- UTILITY OF RADIOIODINE SPECT/CT FOR LESIONAL DOSIMETRY
- WHEN TO USE SPECT/CT FOR BEST IMPACT IN THYROID CANCER MANAGEMENT
- CONCLUSION
- Footnotes
- REFERENCES
- Figures & Data
- Supplemental
- Info & Metrics