


Abstract
Gastrointestinal bleeding can result in significant morbidity. Scintigraphy plays an important role in detecting, localizing, and grading the bleed. Effective scintigraphic evaluation of gastrointestinal bleeding can be complicated by its intermittent nature and the patient’s hemodynamic instability. Dynamic evaluation, delayed imaging, and an understanding of the labeling process are necessary tools to help improve detection rate and localization.
Gastrointestinal bleeding can result in significant morbidity. Scintigraphy plays an important role in detecting, localizing, and grading the bleed. Dynamic evaluation, delayed imaging, and proper red blood cell (RBC) labeling are essential to have an effective impact on patient care.
CASE REPORT
An 83-y-old woman presented with hematochezia. The findings of a recent colonoscopy were negative, and the hemoglobin level was 7.7 g/dL.
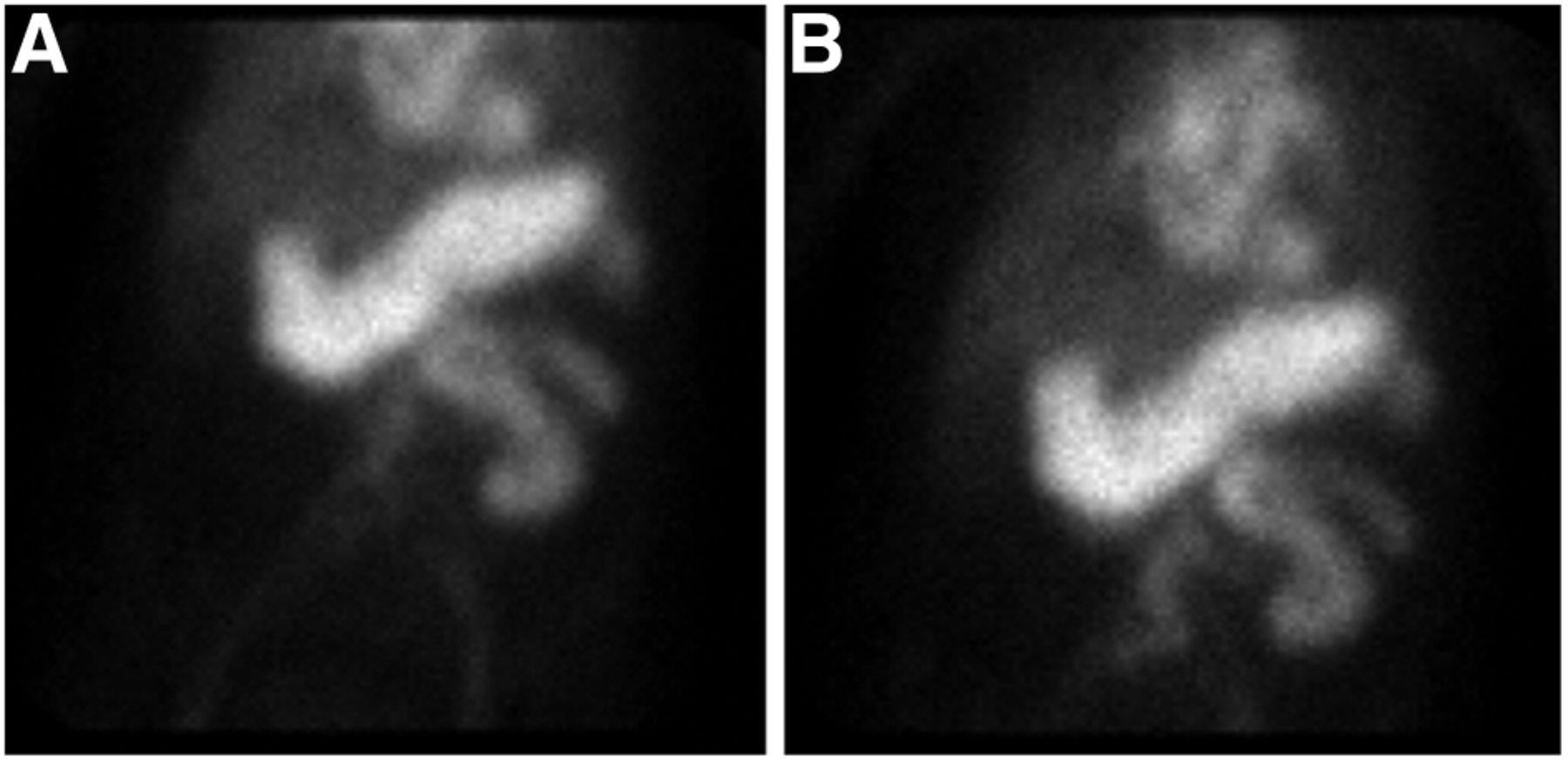
A gastrointestinal bleed scan (777 MBq [21 mCi] of RBCs labeled with 99mTc in vitro) was acquired at 1 min/frame for 60 min (Fig. 1), with static images obtained at 70 and 80 min (Fig. 2).
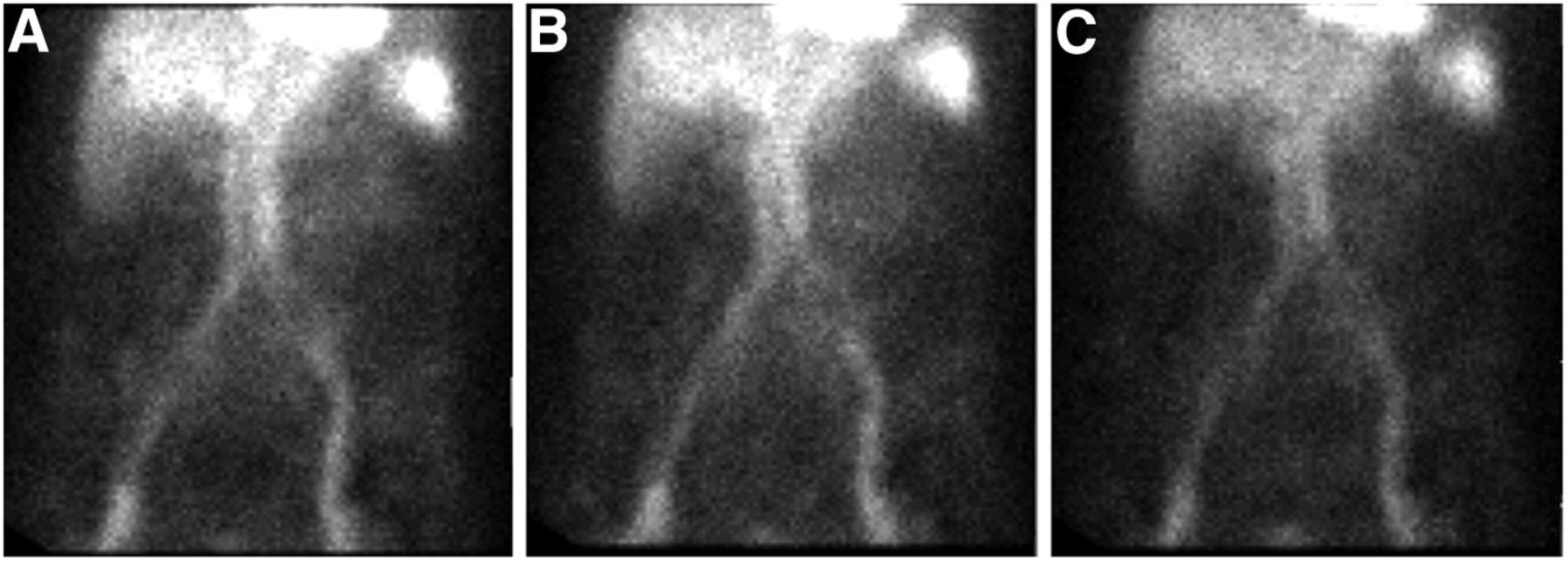
Gastrointestinal bleed scan images acquired at 10 min (A), 30 min (B), and 50 min (C).

Static images acquired at 70 min (A) and 80 min (B).
No abnormal activity was identified during the initial dynamic acquisition (Fig. 1). The additional static imaging revealed radiotracer in the stomach and proximal small bowel (Fig. 2). A brisk prepyloric bleed was reported. Subsequent upper endoscopy revealed a gastric and esophageal ulcer.
DISCUSSION
The intermittent nature of gastrointestinal bleeding can complicate detection. Zettinig et al. reviewed 89 gastrointestinal bleeding scans and reported that 30 of 41 positive scans (73%) were positive on delayed imaging only (1). In another publication, Howarth also supported delayed imaging and added that dynamic imaging helps localize bleeding (2). Dynamic imaging improves the detection of small bleeds and helps differentiate a bleed from areas of hypervascularity or vascular anomalies.
When activity is identified within the stomach on a 99mTc-RBC scan, poor labeling of the RBCs and free pertechnetate accumulating within the gastric mucosa must be considered. Imaging of the thyroid is essential. If the thyroid shows no uptake the bleed can be confirmed, unless the thyroid is surgically absent or was ablated, or the patient is on suppressive doses of thyroxine. Free pertechnetate can be secreted into the stomach lumen and will progress along the small bowel.
Another consideration with suspected gastric activity is radiotracer within superimposed structures, such as the transverse colon. Although each lumen has a distinct morphology, limited activity on initial imaging can make exact localization difficult. Delayed imaging helps in bleed localization by allowing recognition of structures into which antegrade or retrograde progression of activity occurs. In the presented case, imaging could not be continued because of hemodynamic instability.
Treatment of hemodynamic instability in the setting of anemia and suspected bleeding often includes transfusion. Labeling efficiency is affected by the presence of additives in the transfusion. The in-vitro UltraTag (Mallinckrodt Pharmaceuticals) kit labeling process involves adding anticoagulated blood to the kit containing stannous ion (Sn2+). The stannous ion diffuses into the RBCs. After incubation, the extracellular Sn2+ must be oxidized to prevent it from reducing the extracellular 99mTc-pertechnetate, because reduced 99mTc-pertechnetate is unable to enter the RBCs. 99mTc-pertechnetate is then added, and it diffuses into the pretinned RBCs. Once intracellular, pertechnetate is reduced by the intracellular Sn2+ and binds to hemoglobin.
In recently transfused patients, the ethylenediamine tetraacetic acid anticoagulant contained in the transfusion binds the stannous ion before it can enter the RBCs, significantly reducing the labeling efficiency (3,4).
Finally, the amount of bleeding is also an important aspect of clinical decision making. Smith et al. investigated the use of “visual blood loss estimate” on delayed imaging (5). The bleed was graded as strongly versus weakly positive (tracer intensity greater than or less than the liver) and early versus late (time to positivity less than or greater than 1 h). All patients with early or strong positivity required aggressive management, as opposed to only 23% of those with late or weak positivity.
CONCLUSION
Effective scintigraphic evaluation of gastrointestinal bleeding can be complicated by its intermittent nature and the patient’s hemodynamic instability. Dynamic evaluation, delayed imaging, and an understanding of the labeling process are necessary tools to help improve detection rate and localization.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Jan. 27, 2014.
REFERENCES
- Received for publication September 17, 2013.
- Accepted for publication October 23, 2013.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.