


Abstract
Benign unilateral uptake in the diaphragmatic crus is a relatively uncommon finding on 18F-FDG PET/CT that can mimic the appearance of malignancy in patients with known cancer, as illustrated in this patient with neuroendocrine carcinoma. It is important for the PET interpreter to recognize this finding and attribute it to benign uptake based on the patient’s history and symptoms at the time of the scan. Correlation with the findings of other available imaging modalities is also important to characterize focal uptake in unusual locations.
In its ability to stage cancers, evaluate response to treatment, and predict patient prognosis, 18F-FDG PET has proven value. However, interpretation can be made challenging by physiologic, inflammatory, or normal variant activity that can mimic the appearance of malignancy (1). This case demonstrates a relatively uncommon abnormal variant of benign unilateral uptake in the diaphragmatic crus (2). It is important for the PET interpreter to recognize this finding and attribute it to benign uptake based on the patient’s history and symptoms at the time of the scan.
CASE REPORT
A 63-y-old woman diagnosed with neuroendocrine carcinoma of the right lung apex in 2003 presented for a restaging PET/CT examination 1 mo after chemoradiation therapy.
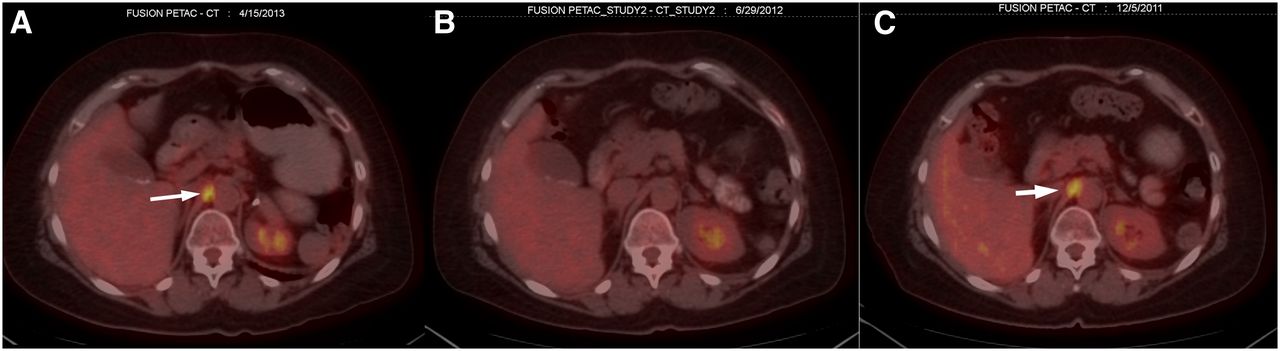
The 18F-FDG PET scan demonstrated focally increased uptake in the right diaphragmatic crus (maximum standardized uptake value, 4.3) that was not present on her PET scan performed 1 y previously but was present on a restaging study performed 2 y previously (Fig. 1). Because the rest of the scan was essentially negative for uptake, this finding needed further investigation. Review of the chart revealed that the patient had not been undergoing radiation therapy at the time of the last study but had received treatment within 3 mo of her previous PET study, which had demonstrated the unilateral diaphragmatic crus uptake. Additionally, the scout view of a recently performed diagnostic CT scan demonstrated right hemidiaphragm elevation (Fig. 2), which is highly suggestive of paralysis secondary to phrenic neuropathy (3).

Three PET/CT fusion images taken approximately 1 y apart. Current study (A) and study acquired 2 y previously (C) were both performed within 3 mo of external-beam radiation therapy, and both demonstrate increased uptake (arrows) at right diaphragmatic crus. Patient had not received any recent radiation therapy at time study acquired 1 y previously (B), which did not show any uptake at right crus.

Scout diagnostic CT image clearly depicts elevated uptake in right hemidiaphragm (arrow), which is typical for paralysis secondary to phrenic nerve damage.
Given the temporal relationship between radiation therapy and the right diaphragmatic crus uptake on 18F-FDG PET and hemidiaphragm elevation, one could surmise that this was benign activity. Because the activity was on the paralyzed side of the diaphragm, radiation-induced phrenic nerve neuropathy was the likely etiology.
Currently, the patient does not demonstrate any evidence of recurrent malignancy by imaging or tumor markers. She is being monitored by serial imaging at a reduced interval and has discontinued radiation therapy.
DISCUSSION
The diaphragmatic crus is an uncommon site of benign physiologic 18F-FDG PET uptake that can be caused by hyperventilation, hiccups, or restrictive pulmonary disease (1). However, in such cases, the uptake is typically bilateral. Unilateral diaphragmatic uptake is most often due to diaphragmatic paralysis (2,4). When the uptake is contralateral to the paralyzed hemidiaphragm, the etiology is a compensatory increase in the work of the functioning side (4). When the uptake is on the ipsilateral side, phrenic nerve neuropathy should be suspected. In the setting of malignancy, secondary effects of external-beam radiation can cause hemidiaphragmatic paralysis via fibrotic changes or induction of phrenic neuropathy (5). Phrenic neuropathy is reversible, but recovery is slow (3).
Because the transient focal unilateral uptake described in this patient demonstrated a temporal relationship with radiation treatments and was ipsilateral to the paralyzed and elevated hemidiaphragm, radiation-induced left phrenic neuropathy could be reasonably suspected.
CONCLUSION
Unilateral diaphragmatic focal uptake is an uncommon abnormal variant on 18F-FDG PET but one that should be recognized as benign activity. Given that the activity was ipsilateral to the elevated hemidiaphragm in this case, radiation-induced phrenic neuropathy could be suspected with reasonable certainty (1,2,4). Radiation treatments can result in ipsilateral diaphragmatic paresis if the phrenic nerve is included in the treatment field, as often is the case in targeted therapy to the axilla in lymphoma (3,5). In this patient, the phrenic nerve was likely irradiated because of the tumor’s location in the right lung apex, making this a rare instance of radiogenic phrenic neuropathy in a primary lung malignancy. This case also demonstrates the importance of correlation with patient history and other available imaging modalities to characterize focal uptake in unusual locations.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Jan. 27, 2014.
REFERENCES
- Received for publication July 29, 2013.
- Accepted for publication September 23, 2013.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.