


Abstract
We describe a case of a 9-y-old girl who on 18F-FDG PET imaging was found to have a highly metabolically active sacral tumor with an average standarized uptake value of 6.2. The tumor was proven to be osteoblastoma by pathologic examination. Osteoblastoma is a relatively rare benign primary bone tumor and occurs predominantly in patients younger than 20 y. The most common area of involvement is the spine. Osteoblastoma has been reported to be metabolically active on 18F-FDG PET imaging, with an average standarized uptake value of 3.2, which renders 18F-FDG PET imaging unable to differentiate benign from malignant primary bone tumors. To our knowledge, only 5 cases of osteoblastoma evaluated by 18F-FDG PET imaging have been reported in the literature; all were metabolically active on 18F-FDG PET imaging. The objective of this case report is to show that a metabolically active primary bone tumor on 18F-FDG PET imaging might be benign and not necessarily malignant.
PET is an important imaging modality for a patient with malignancy. 18F-FDG PET imaging is commonly used for staging and restaging cancer. 18F-FDG accumulates in cancer cells because of their increased glucose metabolism. However, increased glucose metabolism is not specific to malignancy. Some benign bone lesions may accumulate 18F-FDG in amounts similar to those seen for malignant bone tumors (1). Osteoblastoma is an uncommon benign and vascular osteoid-forming bone tumor (2). In the literature, we could find only 5 osteoblastoma cases involving 18F-FDG PET evaluation, all of which revealed increased 18F-FDG uptake (1–4). Here, we present another case of sacral osteoblastoma that revealed increased metabolic activity on 18F-FDG PET imaging. The objective of this case report is to show that a metabolically active primary bone tumor on 18F-FDG PET imaging may be a benign tumor such as osteoblastoma and not necessarily malignant.
CASE REPORT
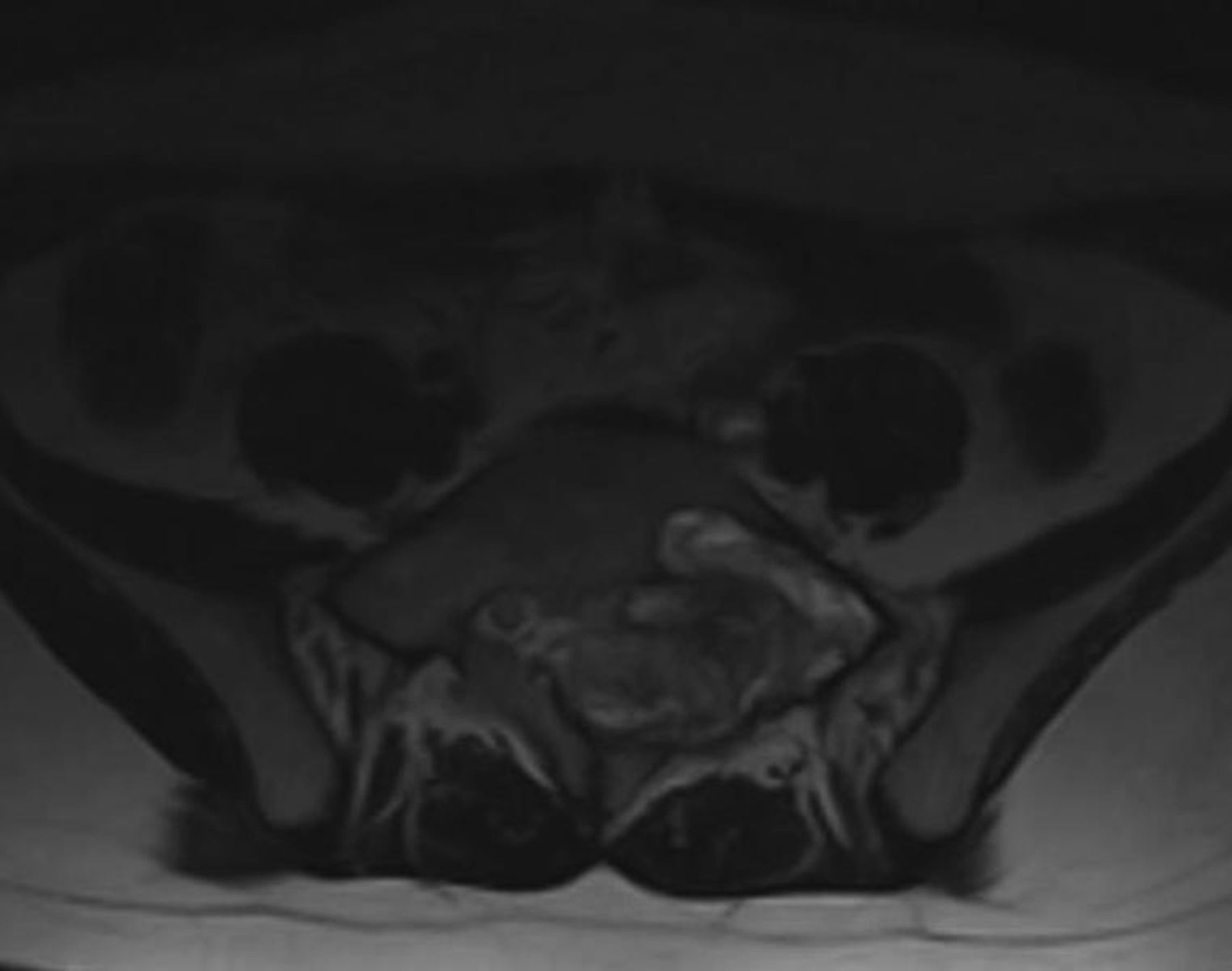
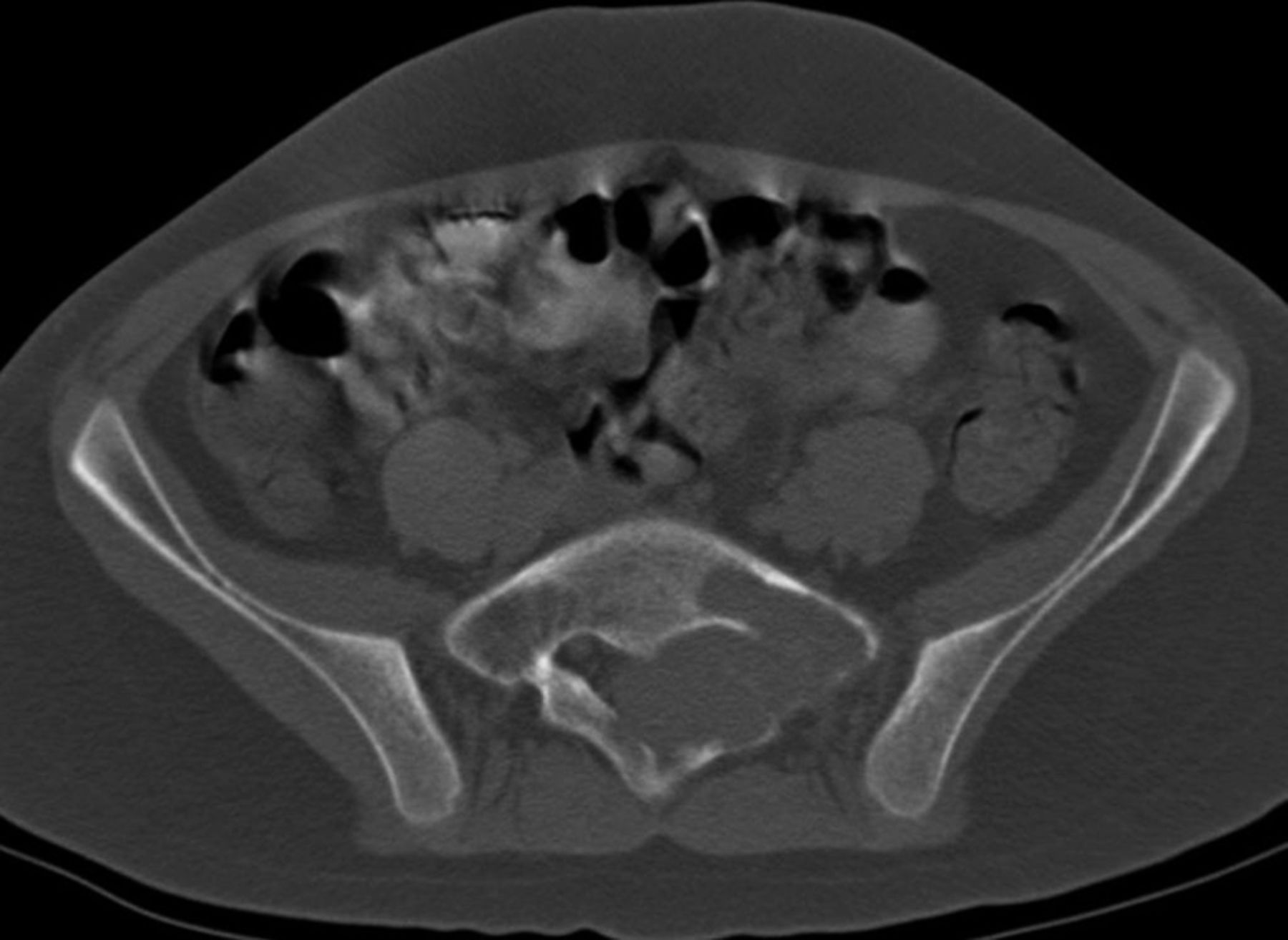
The orthopedic clinic referred a 9-y-old girl to the nuclear medicine department for whole-body bone scanning. She had a 1-mo history of left hip pain radiating to the left thigh. Two weeks before surgery, she started to complain of intermittent abdominal pain, constipation, and occasional difficulty with urination. Initially, she was evaluated by simple radiography of the hip, with normal results. Whole-body bone scanning was performed and found an isolated focal osteoblastic lesion involving the L5 and S1 vertebrae (Fig. 1). Three days later, the patient underwent lumbar spine MR imaging, which demonstrated a large mass (measuring 4 × 2.5 cm) originating from the left sacral ala at the S1 and S2 levels. The mass was invading the spinal canal and the left S1 and S2 foramina and extended upward to the left L5–S1 neural exit canal, causing L5–S1 neural foramina expansion (Fig. 2). Five days later, the patient underwent lumbar spine CT, which demonstrated an enhancing soft-tissue mass causing expansion of the left S1 intervertebral foramen and showing dumb-bell growth inside the spinal canal and outside the left S1 intervertebral foramen (Fig. 3). About 5 wk later, the sacral mass was further evaluated by whole-body 18F-FDG PET/CT imaging, which demonstrated increased 18F-FDG activity, with an average standarized uptake value (SUV) of 6.2 and a maximum SUV of 9.3 (Fig. 4).
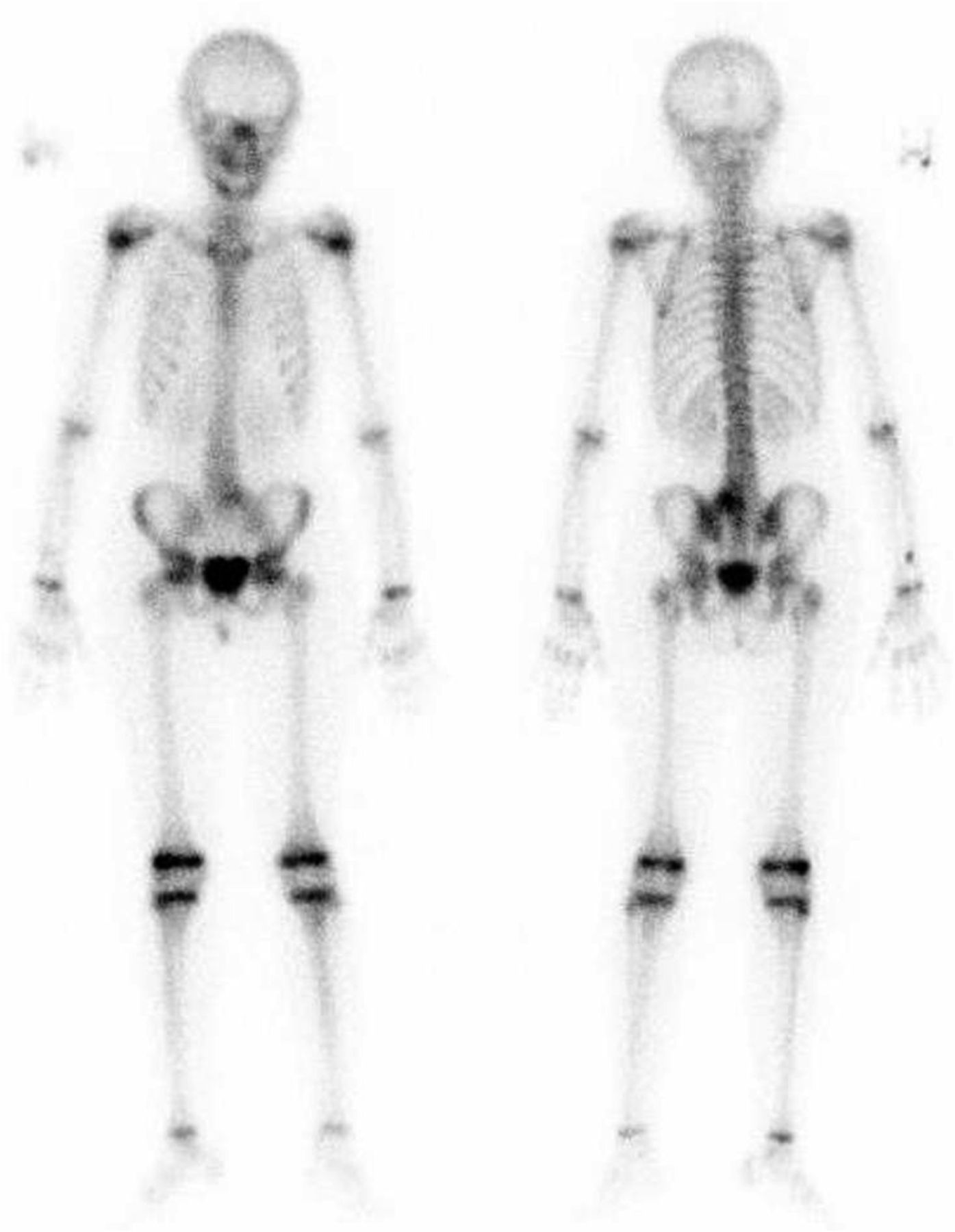
Whole-body bone scan showing focally increased osteoblastic activity in sacrum.
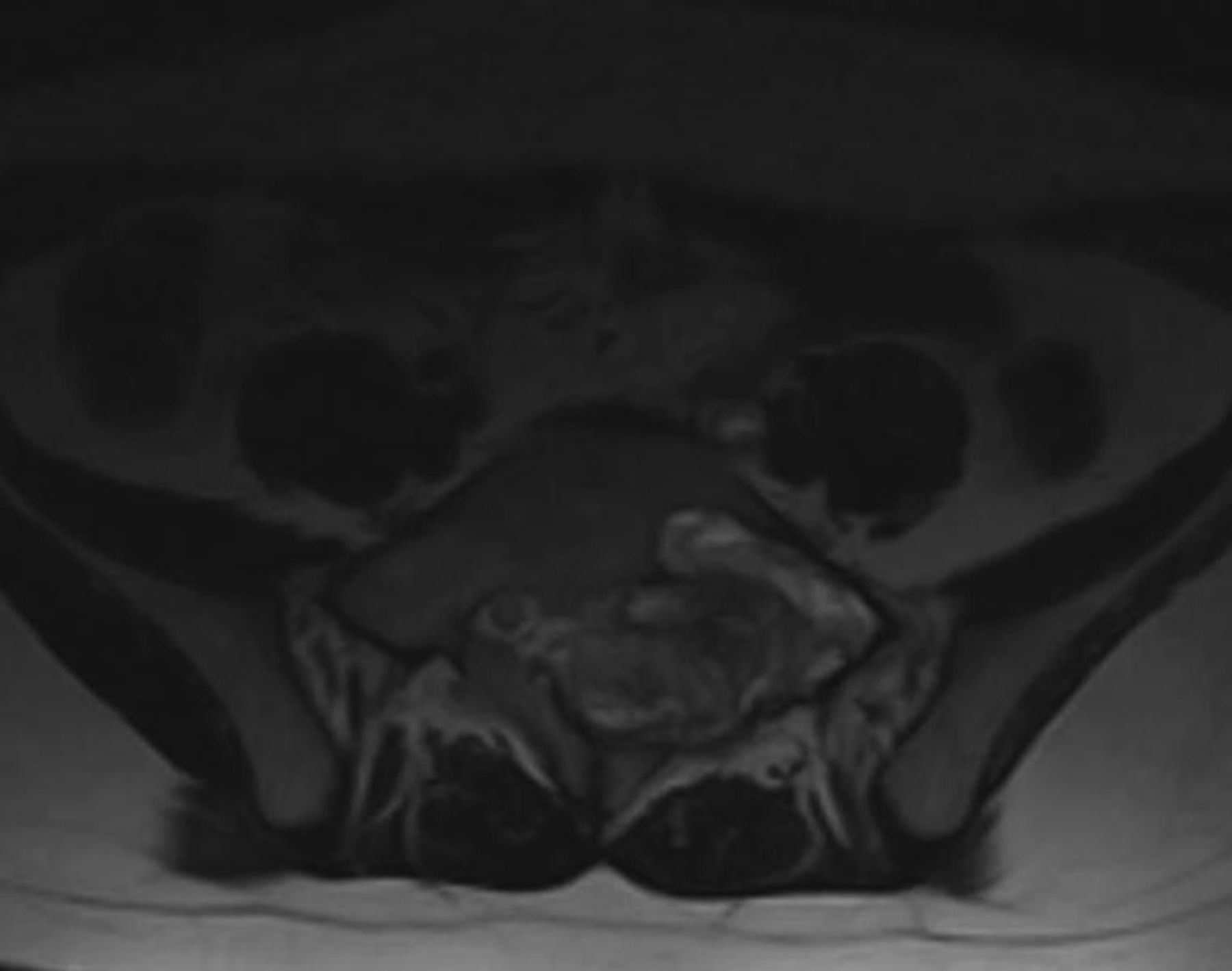
T2-weighted MR image showing heterogeneous soft-tissue mass in left sacrum encasing sacral nerves.
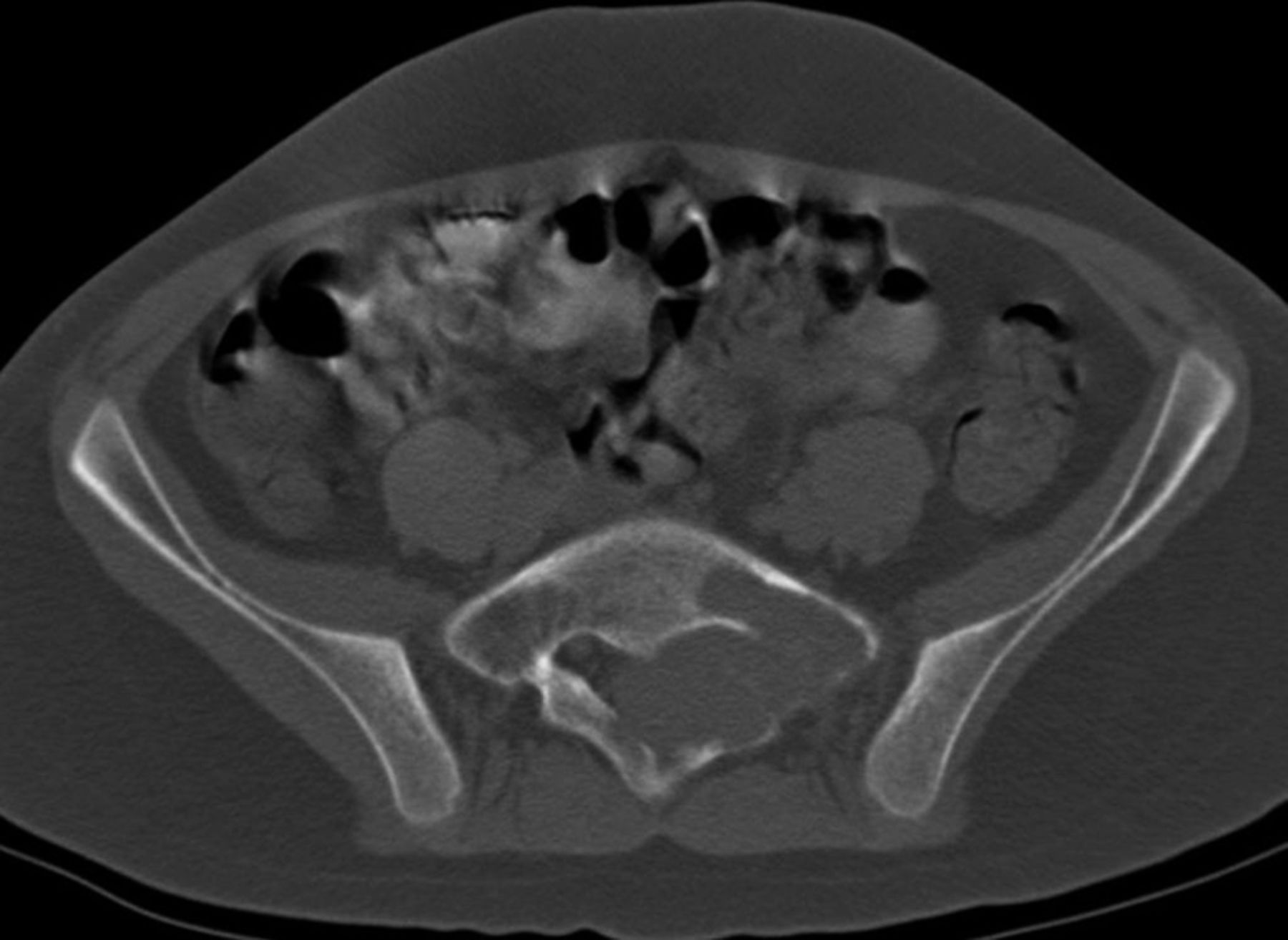
CT image (bone window) showing well-defined soft-tissue mass in left sacrum with marginal bone sclerosis.

18F-FDG PET/CT image showing metabolically active left sacral bone tumor.
Nine days after the PET/CT examination, the patient underwent excisional biopsy followed by posterolateral fusion of L5–S1 and S1–S2. Histologically, the tumor was composed of woven bone spicules and irregular trabeculae lined by benign activated osteoblasts. A cellular vascular stroma containing sheets of large osteoblasts and osteoclast-type giant cells between the bone trabeculae was seen. There was no nuclear pleomorphism or atypical mitotic figures. These features are those of clinically aggressive epithelioid osteoblastoma destroying surrounding normal bone (Fig. 5). Postsurgically, the patient reported gradual improvement, with complete disappearance of her symptoms within 2–3 mo.
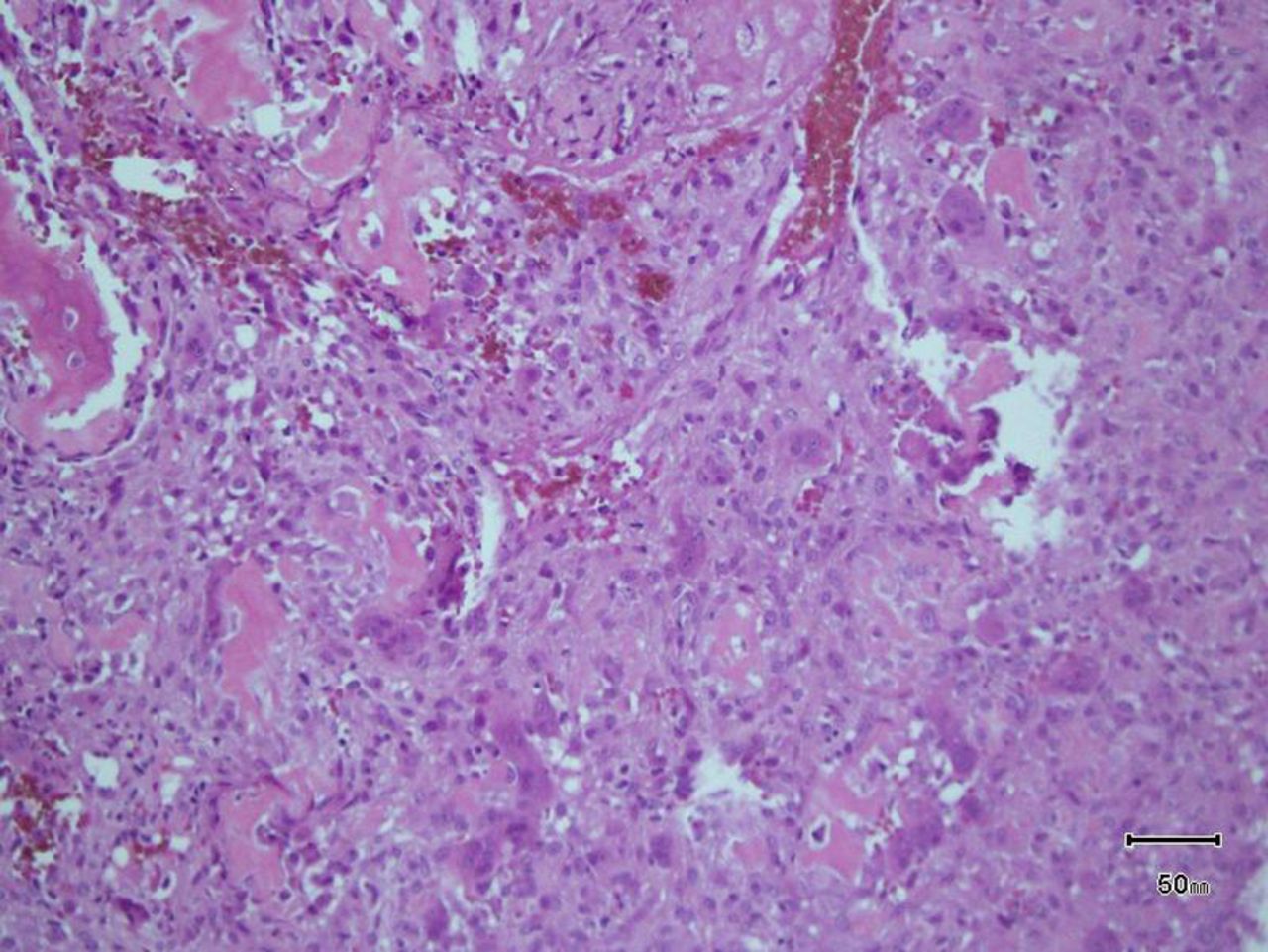
Histopathologic image showing tumor composed of woven bone spicules and irregular trabeculae lined by benign-looking activated osteoblasts (osteoblastoma).
DISCUSSION
In 1956, Jaffe and Lichtenstein independently proposed the term benign osteoblastoma (5,6). Osteoblastoma is a bone-producing lesion accounting for approximately 1% of all primary bone tumors. The most common presenting symptom is pain. The basic microscopic pattern in osteoblastoma is bone-forming tumor containing numerous osteoblasts producing osteoid and woven bone. Although osteoblastoma affects patients within a wide age range (6–75 y), the average age at the time of diagnosis is between 15 and 20 y, and most patients (>80%) are diagnosed before the age of 30 y (7). Osteoblastoma occurs most commonly in males (male-to-female ratio, 2.5:1). About 30%–40% of all cases of osteoblastoma involve the spine. The most common area of involvement is the cervical spine, followed by the lumbar spine and sacrum. In the spine, osteoblastoma is usually confined to the posterior elements (8,9).
The histologic distinction between osteoid osteoma and osteoblastoma may be challenging. A size criterion was widely used in the past: tumors larger than 2–3 cm were classified as osteoblastoma, with a cutoff of 1.5 cm advocated by some authors. The current consensus is that osteoid osteoma and osteoblastoma, rather than being 2 modes of expression of a single tumor, are 2 distinct entities regarding not only their histology but also their clinical and radiologic presentation. Clinically, osteoid osteoma arises in the long bones. The pain predominates at night and responds to aspirin. Osteoblastoma more often affects the axial bones. The pain does not increase at night initially and is less responsive to antiinflammatory medications. Osteoid osteoma has no potential for progression, and the tumor may regress either spontaneously or with nonoperative management. Osteoblastoma, in contrast, has a greater potential for growth, with destruction of bone tissue or even malignant transformation. The sclerotic reaction is often milder in osteoblastoma than in osteoid osteoma. Osteoblastoma may exhibit locally aggressive behavior and is more likely than osteoid osteoma to recur after surgical excision (10).
Kole et al. (1) investigated the glucose metabolism of various bone lesions with 18F-FDG PET imaging. Nineteen malignant bone tumors (including 6 nonosseous metastatic cancers) and 7 benign bone tumors (including a case of osteoblastoma) were included in the study. All bony lesions were clearly visualized with 18F-FDG PET except for a single bone infarction lesion. In addition, the maximum and average SUVs were not higher for malignant than benign lesions. In particular, the osteoblastoma had average and maximum SUVs of 3.2 and 8.7, respectively. Kole et al. concluded that it is not possible to differentiate between benign and malignant bone tumors using 18F-FDG PET scanning and that there is no correlation between glucose metabolic rate and the biologic aggressiveness of bone tumors. Aoki et al. (11) investigated the glucose metabolism of various bone lesions with 18F-FDG PET imaging in 52 patients (19 malignant primary bone tumors and 33 benign bone lesions). Although they found a statistically significant difference in SUV between benign and malignant primary bone tumors, a considerable overlap in SUVs was observed between the 2 groups. In particular, high 18F-FDG uptake was noted in giant cell tumor, chondroblastoma, fibrous dysplasia, sarcoidosis, Langerhans cell histocytosis, and fibroma.
We could find reported in the literature only 5 cases of osteoblastoma evaluated by 18F-FDG PET imaging (1–4). All were metabolically active on 18F-FDG PET imaging. Increased 18F-FDG uptake did not relate to tumor location (temporal bone, nasal cavity, pedicle of L5 vertebra, tibia, and talus). In our case, the osteoblastoma was located in the sacrum and was also metabolically active on 18F-FDG PET imaging. In this context, in a series of 3 patients, Imperiale et al. (4) showed that 18F-FDG PET imaging can be used to monitor the result of treatment of osteoblastoma with percutaneous radiofrequency ablation, as 18F-FDG PET imaging was performed both before and after treatment.
CONCLUSION
Osteoblastoma—usually considered benign bone tumor—is a metabolically active tumor that demonstrates increased 18F-FDG uptake on PET imaging. We add this case to those few cases of osteoblastoma imaged with 18F-FDG PET reported in the literature. 18F-FDG PET imaging has little value in differentiating malignant bone tumors from benign bone tumors.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Oct. 21, 2013.
REFERENCES
- Received for publication June 6, 2013.
- Accepted for publication September 16, 2013.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.