


Abstract
186Re-1-hydroxyethylidene-1,1-diphosphonate (HEDP) is an attractive radiopharmaceutical for the treatment of bone pain arising from skeletal metastatic lesions. Currently, 186Re-HEDP is most commonly used in European countries. The aim of this study was to investigate the palliative efficacy and adverse effects of 186Re-HEDP in patients with different types of cancers and skeletal bone pain. Methods: Nineteen (8 male, 11 female) patients with various cancers (breast, prostate, renal cell carcinoma, colon, and neuroendocrine tumors) and painful bone metastases were included in the study. A dose of 1,480–3,330 MBq (40–90 mCi) of 186Re-HEDP was administered intravenously. The patients’ level of pain relief was assessed by the Visual Analog Scale for 8 wk after treatment and by a weekly blood cell count to evaluate for hematologic toxicity. Results: The overall response rate was 89.5%, and the mean pain score assessed by the Visual Analog Scale was reduced from 9.1 to 5.3 after 1 wk (P = 0.003). No adverse effects were reported by patients during intravenous administration or for up to 24 h after administration. A flare reaction was seen in 63.2% of patients, mainly during days 1–3, and lasted for 2–4 d. There was no significant correlation between the response to therapy and the flare reactions (P > 0.05). The nadir of platelet reduction occurred at the fourth or fifth week and led to platelet infusion in only 4 patients with a low baseline platelet count and diffuse skeletal metastases. Bone marrow suppression occurred in patients receiving higher doses, but no clinical problems were seen except in 2 patients who required packed cell transfusion similar to their prior transfusions. Conclusion: 186Re-HEDP is an effective radiopharmaceutical for the palliative treatment of metastatic bone pain and has minimal adverse effects.
The skeleton is the most common site of metastatic disease, and tumors arising from the breast, prostate, lung, thyroid, and kidney commonly spread to bone. The frequency of bone metastases has been estimated at 65%–75% in patients with breast and prostate cancer (1,2) and about 30%–40% in those with lung cancer (3). Bone pain, as the main symptom of skeletal metastases and the most common type of cancer-related pain, obviously has a negative impact on quality of life (4). Currently, the factors contributing to cancer pain are not completely understood (5,6), and metastatic bone pain might be poorly localized for external radiation therapy (7). Various modalities have been introduced for the treatment of bone metastases, including analgesics, hormone therapy, cytotoxic drugs, biphosphonates, and surgery; however, they are not effective in all patients with painful refractory skeletal metastases. An alternative approach is systemic administration of radiopharmaceuticals, which is a valuable and effective method for relieving bone pain in patients with multifocal skeletal metastases (4,8).
Various bone-seeking β-emitting radiopharmaceuticals have been developed, including 32P, 89Sr, 153Sm-ethylenediaminetetramethylene phosphoric acid, 186Re-1-hydroxyethylidene-1,1-diphosphonate (HEDP), and 188Re-HEDP. 186Re is a promising radionuclide with a physical half-life of 89.3 h, maximum β-emission of 1.07 MeV, and 9% abundant γ-emission of 137 keV, making it suitable for imaging and dosimetry (9,10). These physical characteristics have led to the development and clinical application of 186Re-HEDP for metastatic bone pain palliation, and this therapy has been available in Iran. The main purpose of this study was to evaluate the benefits of 186Re-HEDP for bone pain palliation and its adverse effects in Iranian patients with different types of advanced cancer.
MATERIALS AND METHODS
Participants and Study Design
Patients with histologically confirmed cancers, skeletal metastases, and marked bone pain were included in the study. The patients were referred to the nuclear medicine department for systemic radionuclide therapy and met the eligibility criteria, including age greater than 18 y, multiple bone metastases seen on a recent 99mTc-methylene diphosphonate whole-body scan, intractable or considerable bone pain compatible with scintigraphically detected hot lesions, life expectancy of at least 3 mo, normal or acceptable renal function (creatinine level < 2 mg/dL), and sufficient bone marrow function (platelet count > 150,000/μµL, white blood cell count > 2,500/μµL, and hemoglobin level > 10 g/dL).
Patients who had any of the following criteria were excluded from the study: impending or pathologic fracture, impending or existing spinal cord compression, hemibody whole-body radiation during the previous 3 mo, or pregnancy.
In accordance with the Helsinki declaration, all patients were comprehensively informed about the procedure and possible adverse effects and all gave written consent. Approval for the study was obtained from the local ethics committee.
Pretherapy Evaluation
99mTc-methylene diphosphonate whole-body scanning, renal function assessment, and hematologic assessment were performed on all patients, as well as conventional radiographic or CT/MR imaging evaluation if indicated. Afterward, the patients’ symptoms were evaluated to determine whether they had simple metastatic bone pain. In addition, a neurologic consultation was requested for patients with suspected nerve root compression or a pathologic fracture.
An interval of at least 1 mo was necessary between the preceding and next session of chemoradiotherapy. Furthermore, the type of therapy had not been changed during the 3 mo of the ongoing study, and other treatment regimens such as hormone therapy or biphosphonate were continued.
Baseline data were taken on registration, including pain score, analgesic score, and the blood cell counts in the previous week. Pain was measured using the Visual Analog Scale (0 = no pain and 10 = intolerable pain) (11). For analgesic evaluation, the dosage and type of drug taken (no medication = grade 0, nonopioid analgesics = grade 1, weak opiates = grade 2, strong opiates = grade 3) were recorded.
The analgesic score was calculated by multiplying the number of mean dosages per week by the conversion factor (12). The bone scan index was defined to evaluate any spread of skeletal metastases in pretreatment bone scintigraphy according to the number and extent of focal lesions. The skeleton was divided into 5 anatomic regions—skull, spine, thoracic cage, pelvis, and extremities—and each region was scored from 0 to 2. The bone scan index was the sum of these scores from 0 to 10.
186Re-HEDP Administration
Patients were admitted to the day care unit of the nuclear medicine or radiation oncology department and received 1,480–3,330 MBq (40−90 mCi) of 186Re-HEDP in 30 mL of saline through a running intravenous line for 10 min. The patients were then observed in an isolated room for 6–8 h. All patients received oral or intravenous hydration (∼500 mL) before and after the tracer infusion, and urinary incontinence was managed by bladder catheterization before administration of the drug. Whole-body scanning was performed after 4–24 h using a single-head camera (e.cam; Siemens) equipped with a low-energy high-resolution collimator and energy window setting of 137 keV ± 20%. External dosimetry was performed at 0, 1, 2, 4–6, and 24 h after injection.
Posttherapy Evaluation
The Visual Analog Scale, analgesic intake, and complete blood count were recorded weekly for 8 wk. In addition, the efficacy of the treatment, duration of pain relief, hematologic toxicity, and flare reactions were evaluated. The treatment efficacy was considered complete if the pain score decreased by at least 80%, partial if by at least 50%, and minimal if by more than 25%. In nonresponders, none of these criteria were fulfilled. Hematologic toxicity was assessed by World Health Organization criteria, and a flare reaction was identified as a transient increase in pain intensity of more than 25% that started within 1 wk of the tracer administration and resolved quickly within a few days.
Statistical Analysis
To compare the variables between groups, we applied the t test or paired t test, Friedman test, Fisher exact test or χ2 test, and Mann–Whitney test. A P value of less than 0.05 was considered to be statistically significant. Linear correlations among the variables were analyzed using the Spearman linear correlation coefficient. The SPSS for Windows software package (release 18; SPSS Inc.) was applied for the statistical analysis.
RESULTS
Among 45 referred patients, 20 fulfilled the eligibility criteria for radionuclide therapy. The 20 patients included in the study (12 female, 8 male) had a mean age of 55 y (range, 30–75 y). They had a pathologic diagnosis of breast cancer (11), prostate cancer (4), colon cancer (2), renal cell carcinoma (1), neuroendocrine tumor (1), or synovial sarcoma (1). One patient with breast cancer died 3 wk after treatment because of a sudden onset of brain metastasis symptoms and was therefore excluded from the study (Table 1). Retreatment was arranged for only 1 patient 6 mo after administration of 177Sm-ethylenediaminetetramethylene phosphoric acid.
Patient Demographics
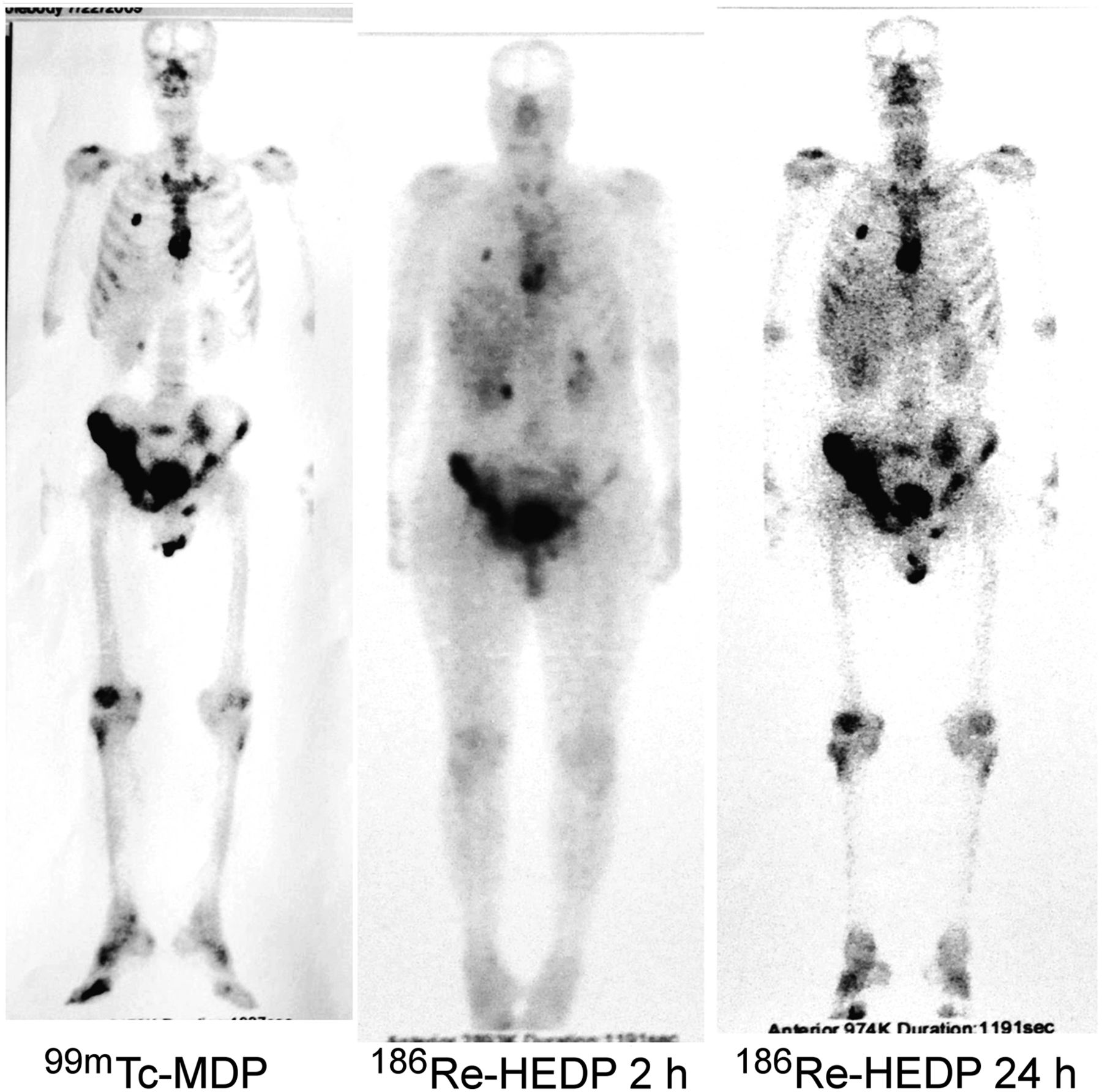
The mean dose administered was 2,882 ± 675 MBq (77.89 ± 18.24 mCi). Only 3 patients received 1,480 MBq, and a dose of more than 2,775 MBq was administered to the other patients. Table 2 summarizes the patient characteristics and treatment results. The distribution of 186Re-HEDP in the body was obtained within 4–24 h and correlated completely with the pretreatment 99mTc-methylene diphosphonate scan (Fig. 1). Pain relief typically began around 7 d after treatment, and a response was observed for at least 1 wk in 15 patients (78.9%) and for 2 wk in 12 patients (63.15%). A complete response was observed in 9 patients (47.3%), a partial response in 4 (21%), and a minimal response in 2 (10.5%). No response was seen in 4 patients (21.1%). The mean duration of pain relief was 5.26 ± 3.58 wk (range, 1–8 wk). It was less than 4 wk in 6 patients (31.5%), 4–8 wk in 2 patients (10.5%), and more than 8 wk in 7 (36.8%) patients. Mean pain scores reduced from 9.10 ± 1.33 before the intravenous injection to 5.31 ± 3.24 during the first week (P = 0.0001) and to 6.63 ± 3.4 at the end of week 8 (P = 0.007). The analgesic score revealed the same trend, and a significant reduction in the mean analgesic score was seen after treatment (P = 0.002). The mean analgesic score was 5.65 ± 3.98 before treatment and 2.73 ± 4.18 at the end of the first week (P = 0.0001), and the mean response duration was 4.15 ± 3.48 wk. Pain palliation was achieved for at least 8 wk in 7 patients (37%), who also had favorable palliation after the study period (Table 3). The duration of response was not significantly different between the groups with and without a flare response (P > 0.05), and no appreciable changes in vital signs or clinically evident adverse reactions were observed within the 24 h after 186Re-HEDP injection.

A 50-y-old man with prostate cancer in whom abnormal foci of increased radiotracer uptake were seen in clavicles, sternum, ribs, spine, sacroiliac joints, and pelvis on 99mTc-methylene diphosphonate (MDP) and 186Re-HEDP scans. In addition, significant uptake resulting from liver involvement is seen on both 99mTc-methylene diphosphonate and 186Re-HEDP scans. Patient showed complete response to therapy and flare reaction after receiving 2,960 MBq of 186Re-HEDP.
Clinical and Hematologic Effects of 186Re-HEDP Before and After Treatment
Efficacy of 186Re-HEDP in Patients with Painful Bone Metastases
A transient decrease in the platelet, white blood cell, and hemoglobin counts was observed. Four patients received 1,480 MBq of 186Re-HEDP at the start of the study, and no considerable complete blood count changes occurred in these patients (Table 4). Although significant bone marrow suppression was detected in patients receiving higher doses of the drug, no clinical problems arose except in 2 patients who required a packed cell transfusion as they had done before treatment. Only 4 patients showed grade 3 platelet toxicity, and 3 of them had a baseline platelet count of lower than 200,000/mL. The other patient had widespread bone metastases and a superscan pattern on the whole-body bone scan. White blood cell toxicity was limited to grade 0 and 1 toxicity, except in 1 patient with grade 2 toxicity. In most patients, the nadir of platelet count reduction was seen at the fourth or fifth week. Declines in peripheral counts returned to the reference range at the end of the eighth week (Table 4).
Side Effects of 186Re-HEDP in Patients with Painful Bone Metastases
Twelve patients (63.2%) experienced a flare response; the majority occurred during days 1–3 and lasted for 2–4 d. A flare reaction occurred in 53.3% (8/15) of responders and 100% (4/4) of nonresponders. As a result, there was no significant correlation between the flare reaction and pain response (P > 0.05). In addition, there was a significant association between the presence of a flare response and dosage (r = 0.47, P = 0.04).
The bone scan index value ranged from 2 to 10 (mean, 6.21 ± 2.4). The mean bone scan index was 6.4 ± 2.55 in the responder group and 5.5 ± 1.73 in the nonresponder group (P > 0.05). The mean alkaline phosphatase serum level was 343 ± 149.84. It was 312 ± 85.5 and 350 ± 162.91 in responders and nonresponders, respectively (P > 0.05).
DISCUSSION
In our study, 78.9% of patients experienced bone pain relief, and a therapeutic efficiency of 50%–92% has been reported with low-dose 186Re-HEDP in different malignancies (13,14). This variation could be related to some heterogeneous factors such as patient selection criteria, tumor type, response criteria, and the method of administration. Comparable results for the efficacy and duration of pain relief have been reported with high-dose 186Re-HEDP (2,590 MBq) (15). Conversely, a dose-escalating study in a small number of prostate cancer patients showed a better response rate when a high therapeutic dose was used (16).
In fact, the intravenous administration of 186Re-HEDP is a challenging subject. The standard dose of 1,295 MBq is recommended as safe, even in heavily pretreated patients (13). However, some data support administering higher doses, which are more likely to reduce tumor markers, ablate micrometastasis, and bring about the disappearance of bony lesions (17). In addition, when there is extensive skeletal involvement, the calculated absorbed dose to specific metastatic deposits has been shown to be significantly reduced (18). This finding could explain why a better response is seen in patients who have received higher doses (19–21). On the other hand, it might be a reasonable justification for a good response in patients with few metastatic lesions treated with a lower administered activity (22–24).
Because 186Re-HEDP delivers a substantial dose to the bone marrow, bone marrow toxicity will be the major adverse effect. In these patients, thrombocytopenia is the dose-limiting factor, whereas leukopenia plays only a minor role (25). A growing number of escalating-dose studies have revealed that the maximum tolerated dose of 186Re-HEDP is 2,960 MBq in prostate cancer (26) and 2,405 MBq in breast cancer (13,27). One report also shows that 2,960 MBq is a threshold for grade 2 toxicity and that grade 3 toxicity was detected in only 1 of 6 prostate cancer patients treated with 4,070 MBq of 186Re-HEDP (25). In fact, bone marrow suppression and the subsequent adverse effects could be affected by various factors other than the dose administered. Suggested factors include the patient’s overall condition, metastatic load, pretreatment blood cell count, and previous therapies (28,29). Our study showed that declines in blood cell count do not depend solely on the dose administered and that baseline complete blood count is important when selecting the best treatment. Thus, we could safely administer higher doses in patients with sufficient blood cell counts. Blood toxicities associated with treatments indicate the importance of pre- and posttreatment monitoring for patients receiving radionuclide therapy, particularly patients with widespread skeletal metastases.
A flare reaction is the other adverse effect of bone-seeking therapeutic radionuclides and is probably related to transient inflammatory reactions that modify intratumoral pressures. Flare reactions can be managed by analgesics or steroid agents (30). An incidence of 10%–30% has been reported with 186Re-HEDP (13,31–34) and up to 50% with 188Re (19). In our study, flare reactions occurred in 63% of patients and could have been due to the patients’ awareness of the probable short-term worsening of bone pain, higher administered dose, or greater fluctuations in the level of pain. The present study, like another reported study (13), suggested that the flare response was not predictive of pain palliation. This suggestion is contradictory to reports that have mentioned the predictive power of flare reactions for treatment response (16,31). Furthermore, we found no significant differences between responders and nonresponders in terms of bone scintigraphy and alkaline phosphatase level—issues that are also controversial in the literature (35). To date, other factors have been evaluated to determine the predictive power of response, such as baseline tumor and bone markers, hemoglobin level, and previous treatments (14,23,24,36), but highly controversial issues remain.
Although several studies have demonstrated that earlier treatment in patients in better clinical condition may improve the response rate (22–24), unfortunately radionuclide therapy is underutilized in Iran. This underutilization could be a result of limited referrals due to specialists’ inadequate knowledge and misconceptions about adverse effects or to the restricted availability and expense of bone pain–palliating radionuclides.
CONCLUSION
186Re-HEDP is an effective radiopharmaceutical for the palliative treatment of metastatic bone pain and has minimal adverse effects.
DISCLOSURE
This paper was adapted from a student thesis at Shahid Beheshti University of Medical Sciences (grant 2345). No other potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank our colleagues in our departments for their productive assistance with data acquisition.
Footnotes
Published online Aug. 5, 2013.
REFERENCES
- Received for publication April 2, 2013.
- Accepted for publication July 12, 2013.





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.