


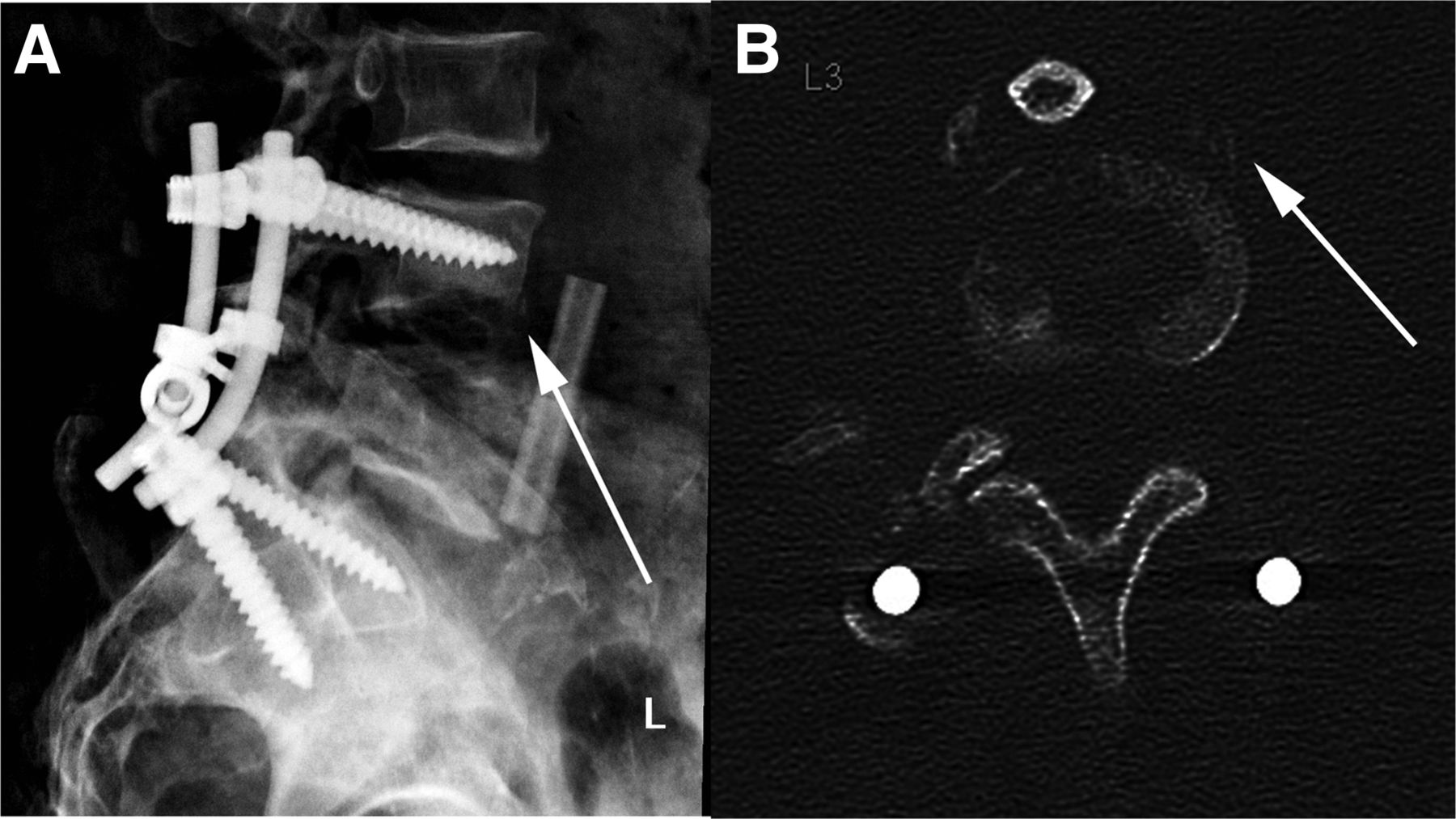
A 62-y-old man presented with chronic, diffuse lower back pain 8 mo after undergoing extensive lumbar spine surgery for osteomyelitis that included an L4 and L5 diskectomy with partial corpectomy, followed by anterior spinal fusion of L4 and L5 with a fibular allograft, and L3 to S1 posterior fusion via spinal instrumentation. Since the surgery, he had multiple admissions due to intractable lower back pain and sepsis. However, multiple bacterial cultures of biopsy samples from the operative site never demonstrated any growth. On the current admission, radiographs (Fig. 1A) and a CT scan of the lumber spine (Fig. 1B) demonstrated erosion of the inferior endplate of L3 and a potential bone fragment anteriorly—findings highly suggestive of osteomyelitis. Bacterial blood cultures were negative. The patient underwent 67Ga scintigraphy, which was compared with an 99mTc-methylene diphosphate (MDP) bone scan performed 2 d prior to the scintigraphy.
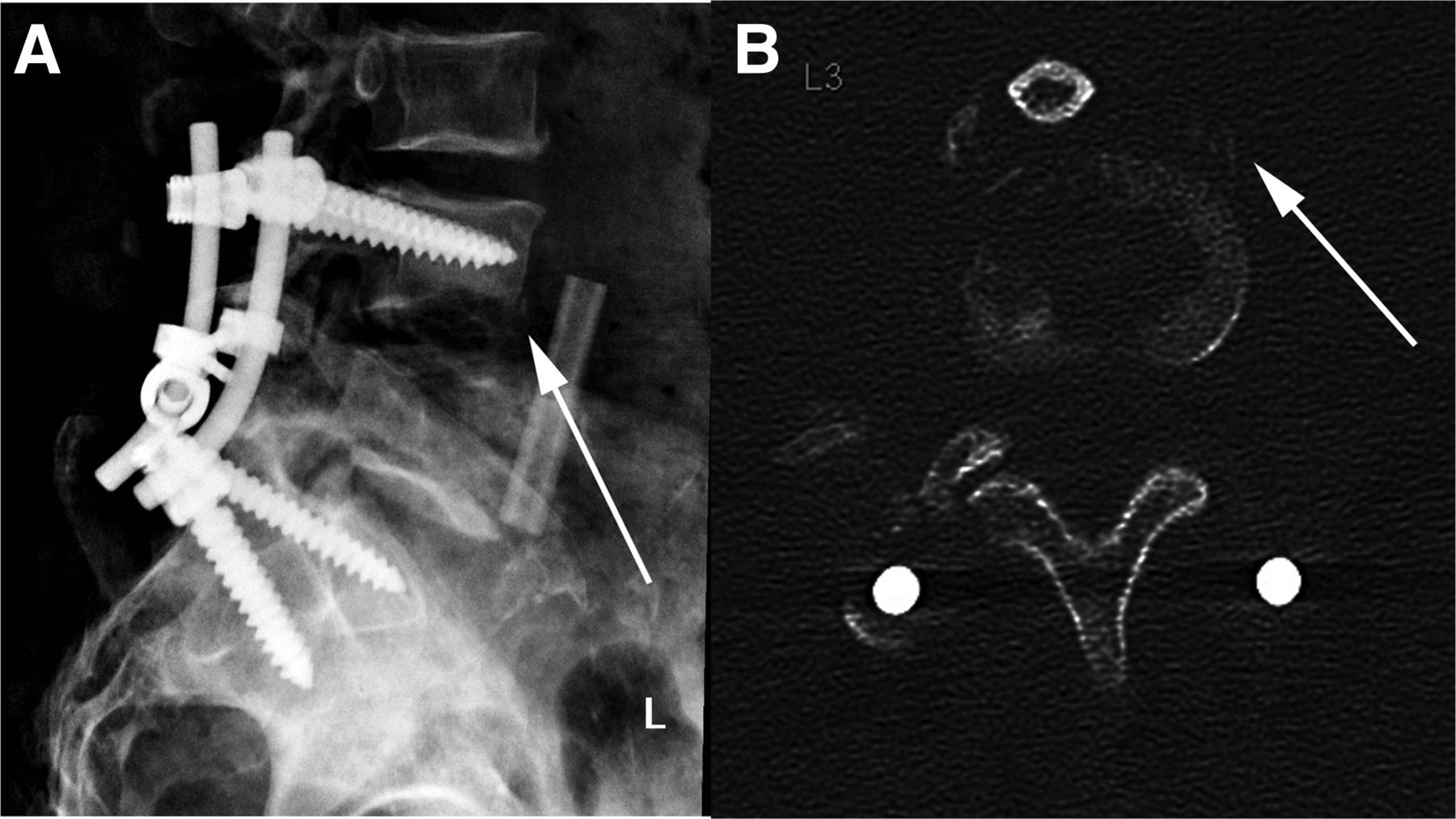
Plain film (A) and axial CT scan of L3 (B) showing inferior endplate erosion and evidence of periostitis (arrows).
The patient was injected with 188.7 MBq (5.1 mCi) of 67Ga-citrate intravenously. A large-field-of-view multipeak camera with a medium-energy parallel-hole collimator was used to obtain scintigrams at 24 and 48 h. Static images of the neck and chest, abdomen and pelvis, and lower extremities were obtained in both the anterior and the posterior projections. SPECT/CT was performed at 48 h for anatomic localization of the abnormal radiotracer uptake and was compared with the previously performed 99mTc-MDP bone scan.
The bone scan demonstrated an area of increased uptake in the body of L3 (Fig. 2A), which was localized to the distal ends of the fixation screws by SPECT/CT (Fig. 3A). Although the location of the activity was suggestive of loosening, the patient had undergone surgery only 8 mo previously; therefore, postsurgical reactive changes could not be excluded. Osteomyelitis involving the hardware remained a possibility, although this location did not correspond to the suggestive findings on correlative imaging. The 67Ga scan was expected to help delineate this differential.
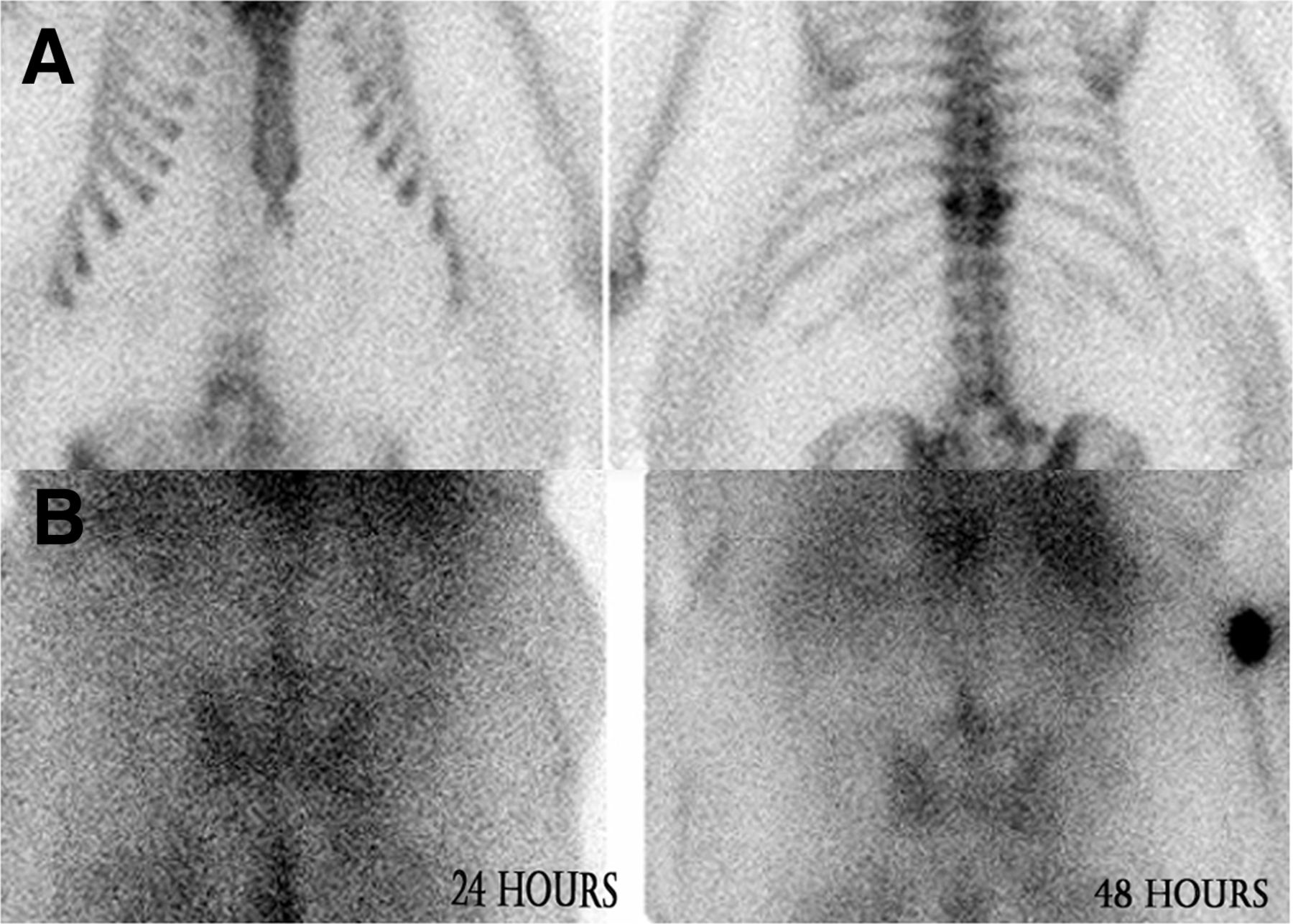
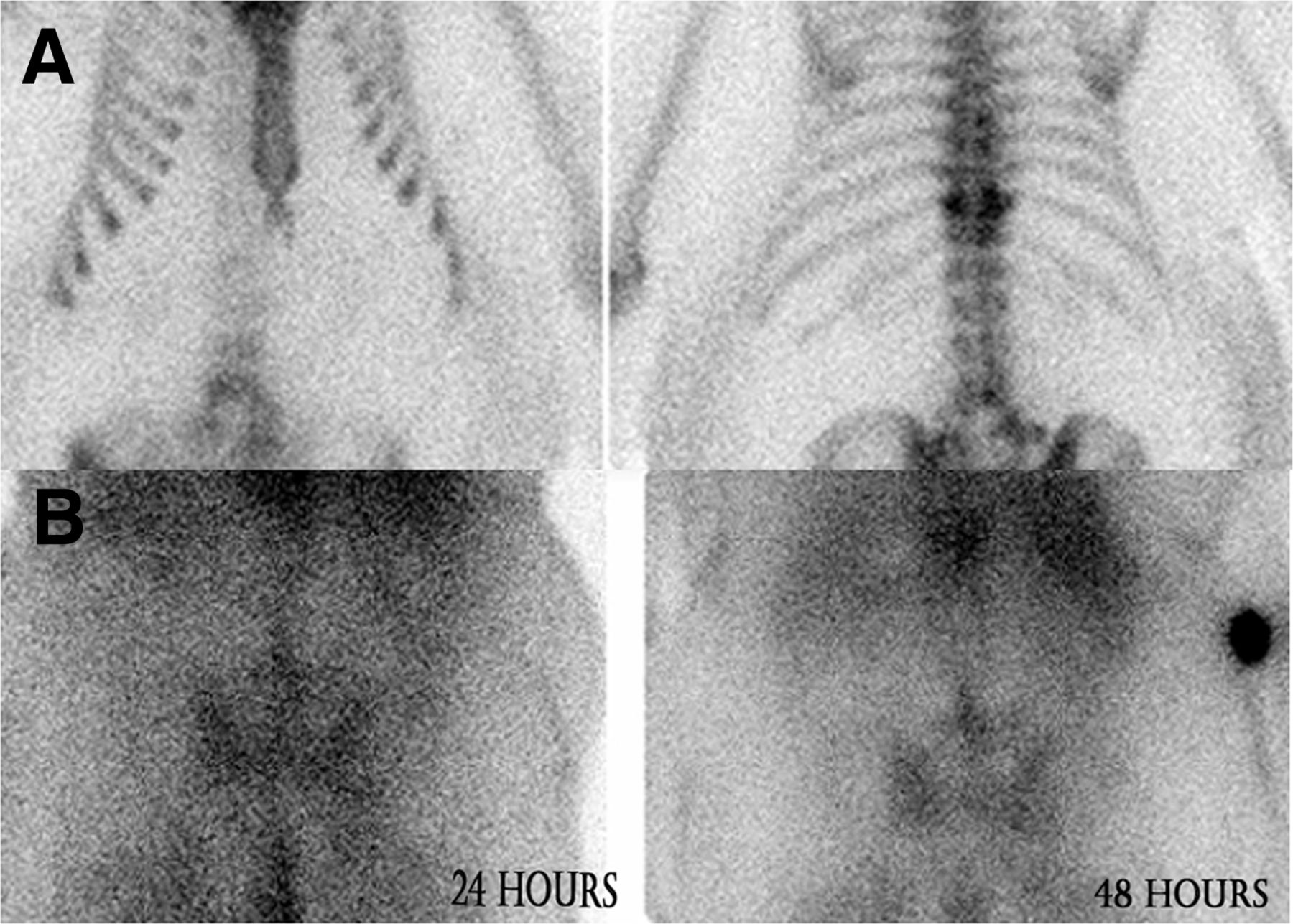
99mTc-MDP bone scan (A) in anterior and posterior projections showing mild activity at L3. More intense uptake is incidentally seen at compression deformity surrounding T11. 67Ga-citrate scan (B) at 24 and 48 h in posterior projection shows progressively increasing uptake in mid lumbar spine.
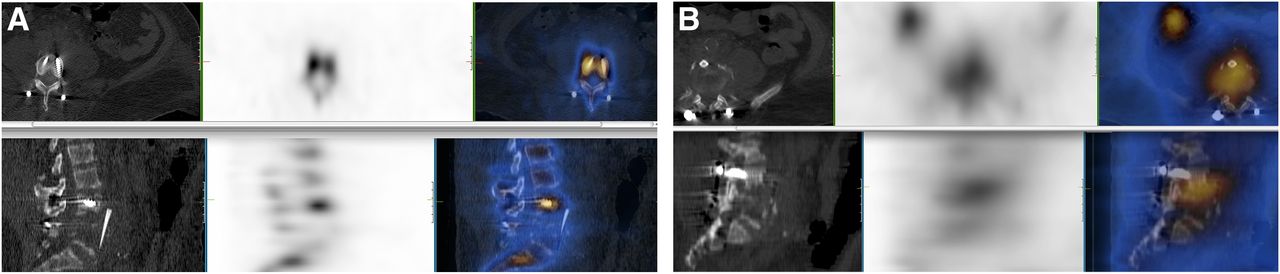
(A) SPECT/CT of 99mTc-MDP bone scan showing that activity is localized to fixation screws and does not involve disk space or bone fragments. (B) SPECT/CT of 67Ga scan showing that spatially discordant uptake involves disk space and inferior endplate of L3 and extends anteriorly to allograft.
On the 67Ga planar images (Fig. 2B), there was progressively increasing uptake in the mid lumbar spine. On SPECT/CT performed 48 h after radiotracer administration (Fig. 3B), there was spatial discordance of the uptake near L3 when compared with the 99mTc-MDP bone scan. The uptake was clearly localized to the inferior endplate of L3 and involved the disk space, allograft site, and anterior bone fragment. These findings were compatible with osteomyelitis or diskitis in this location. The fixation hardware was not involved in the infectious process. Another biopsy sample was taken, guided by the site of activity from the 67Ga scan, and the sample grew Candida.
QUESTION 1
What property of 67Ga makes it a valuable agent in imaging inflammatory processes?
A. Localizes to white blood cells in bone marrow.
B. Binds to transferrin.
C. Localizes to infection sites by binding to leukotaxis.
D. Binds to interleukin-8.
QUESTION 2
What is the target organ with 67Ga administration?
A. Large bowel.
B. Small bowel.
C. Liver.
D. Salivary glands.
QUESTION 3
Which one of the following is not a common cause of false-negative 67Ga findings?
A. Recent gadolinium administration.
B. Blood transfusions.
C. Inadequate bowel preparation.
D. Antibiotic use.
QUESTION 4
In which of the following conditions would 67Ga scintigraphy not be useful?
A. Fever of unknown origin.
B. Inflammatory bowel disease.
C. Sarcoidosis.
D. Lymphoma.
CASE DISCUSSION
67Ga is not an ideal imaging agent because of multiple high-energy photopeaks (93, 185, 288, and 394 keV), low abundance, and a high scatter fraction. However, the physiologic properties of 67Ga still make it an extremely useful agent in appropriate clinical scenarios. It can often uncover an underlying cause of fever or infection that clinicians had not previously considered. It is considered superior to radiolabeled leukocytes in cases of pulmonary inflammatory diseases, drug-induced inflammation, leukopenia, diskitis, vertebral osteomyelitis, and chronic-phase infections. 67Ga may also be the better choice in fever of unknown origin depending on the patient history and suspected sources. Additionally, SPECT/CT can help to mitigate some of the shortfalls of its imaging characteristics.
In our case, the patient had signs, symptoms, and imaging findings suggestive of osteomyelitis in his lumbar spine for several months. However, there was no pathologic evidence, and many courses of antibiotics did not relieve his symptoms. After 67Ga localized an infectious process in the inferior endplate of L3 involving the allograft site, a more targeted biopsy was performed with a subsequent fungal culture, which demonstrated growth of Candida. This was an unexpected finding and an extremely rare case of fungal diskitis in an immunocompetent patient. The patient was started on appropriate long-term antifungal therapy, and his symptoms eventually resolved.
Footnotes
Published online Apr. 17, 2013.
* For the answers, see page 120.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.