


A 56-y-old woman with a history of non–small cell lung cancer presented with a persistent left pneumothorax and a left bronchopleural fistula after bronchial balloon occlusion. A ventilation–perfusion scan using 133Xe and 99mTc-macroaggregated albumin (MAA) was requested to evaluate for possible lung reduction surgery.
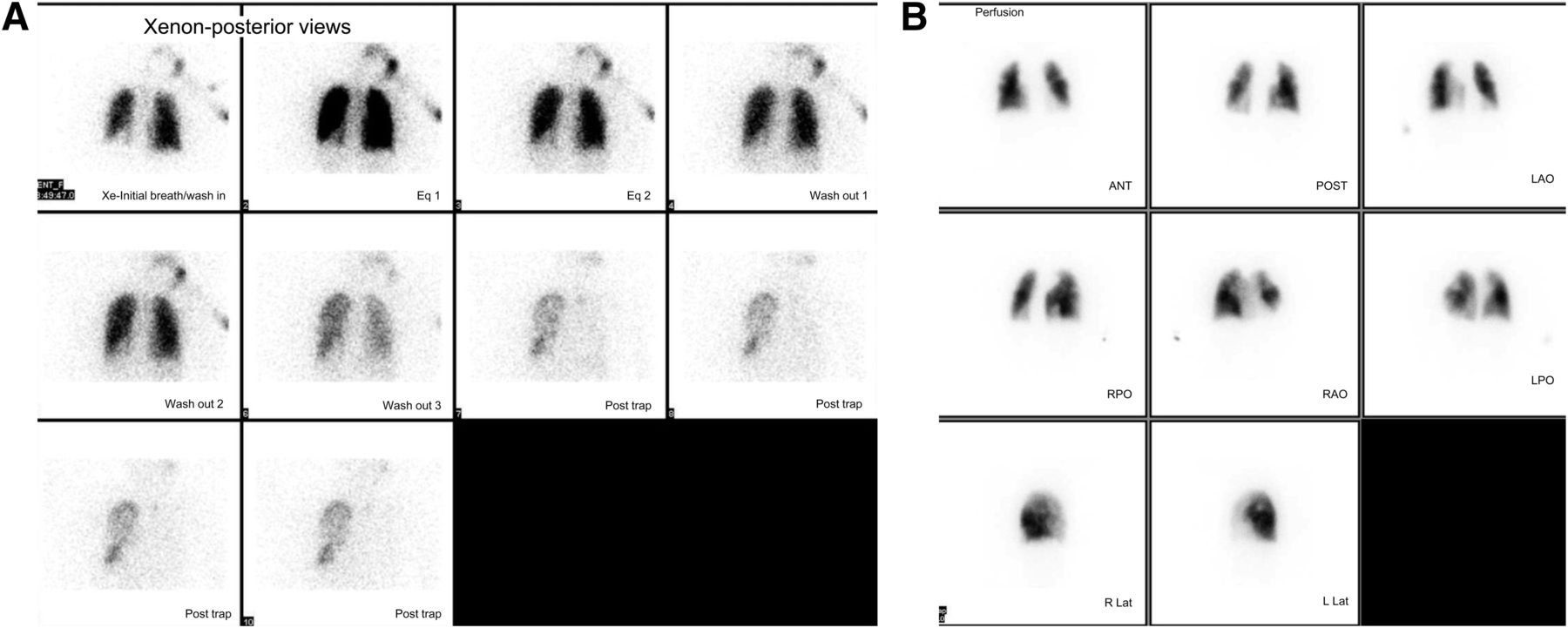
With 428.46 MBq (11.58 mCi) of 133Xe gas, ventilation images were acquired in the posterior projection during a single breath-hold in the equilibrium and washout phases. Regions of interest were drawn around the lungs to generate ventilation time–activity curves. Then, 162.06 MBq (4.38 mCi) of 99mTc-MAA were injected intravenously and 8 standard projections of the lungs were acquired. Regions of interest were drawn around the lungs to calculate differential perfusion.
QUESTION 1
Based on the 133Xe ventilation and 99mTc-MAA perfusion images shown (Fig. 1), what is the best interpretation of this study?
Chronic obstructive pulmonary disease.
Bronchopleural fistula.
Normal scan findings.
A or B.
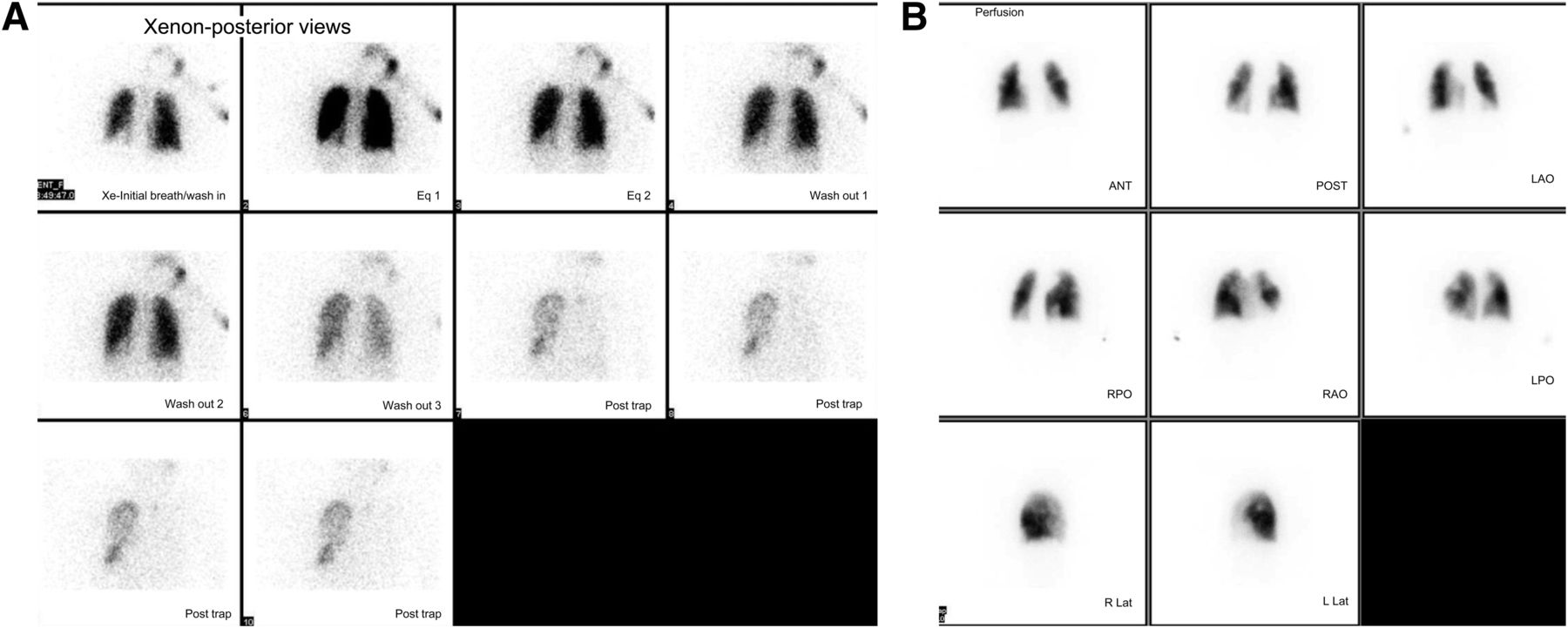
133Xe ventilation images (A) and 99mTc-MAA perfusion images (B).
QUESTION 2
What are the physical half-life and biologic half-life of 133Xe, respectively?
30 min and 20 s.
2 d and 50 s.
5.3 d and 30 s.
7 d and 60 s.
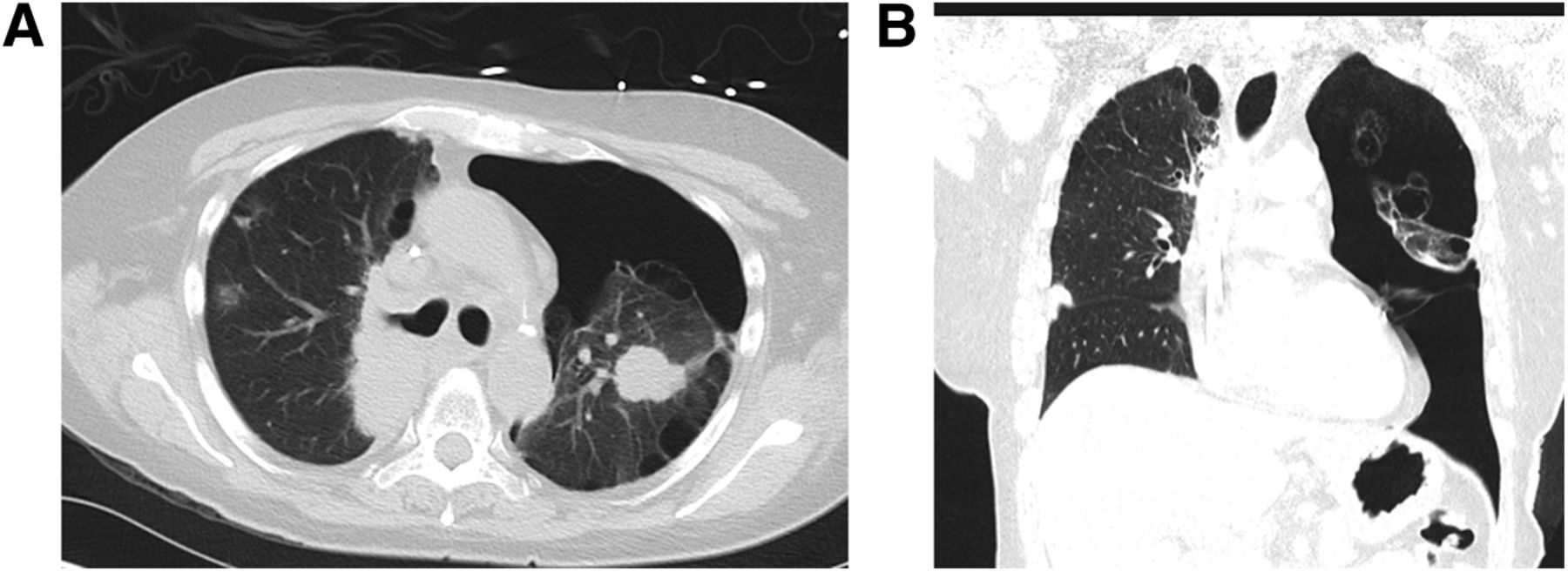
Correlative CT images of the chest are shown (Fig. 2).

Correlative CT images of chest in cross-sectional (A) and coronal (B) views showing mild bilateral emphysema and large left-sided pneumothorax.
QUESTION 3
What are the CT imaging features of a bronchopleural fistula?
Pneumothorax or air trapping on the side of the fistula.
No abnormality on CT images.
Return to midline of a previously shifted mediastinum or a drop in the fluid level by more than 2 cm in patients after pneumonectomy.
A and C.
DISCUSSION
Bronchopleural fistula is a process that can be caused by several lung diseases or by injury. The most common causes are pulmonary infections, trauma, surgical complications, malignancy, and therapy of malignancy. Among various imaging techniques such as plain radiography, CT, 133Xe scanning, and ultrasound, CT and 133Xe scans are the most promising. CT is the anatomic imaging technique of choice for visualization and characterization of a bronchopleural fistula. Most authors recommend CT as the first diagnostic examination. 133Xe ventilation scanning is a simple and accurate method for diagnosis and follow-up of bronchopleural fistula. 133Xe images will show trapping of the tracer on the affected side during the washout phase. A study by Raja et al. in 1999 showed the sensitivity of 133Xe to be 83% and that of 99mTc-DTPA to be 0% in the diagnosis of bronchopleural fistula. In this case, the 133Xe scan findings can be seen in bronchopleural fistula as well as in chronic obstructive pulmonary disease. The distinction could be made by correlating with the history and CT imaging. According to the present literature, CT should be the first modality for the diagnosis and characterization of bronchopleural fistula, and 133Xe scanning can be used as an inexpensive and simple follow-up imaging modality.
Footnotes
Published online Jul. 18, 2013.
↵* For the answers, see page 241.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.