


Abstract
99mTc-sestamibi myocardial perfusion imaging is frequently performed in conjunction with exercise or pharmacologic stress testing for evaluation of coronary heart disease. Interpretation of these studies includes systematic review of unprocessed rotating projectional images for evaluation of cardiac size as well as the presence of motion or attenuation artifacts. Occasionally, incidental noncardiac findings are detected on review of the projectional images. We report a case of a patient with a history of autosomal dominant polycystic kidney disease who was found to have a large abdominal photopenic area on the projectional images. The photopenic area corresponded to the location of large intraabdominal cysts on abdominal CT and was consistent with hepatic cysts associated with the patient’s known polycystic kidney disease. We review the differential diagnosis of large abdominal photopenic regions identified on myocardial projectional images and the importance of routinely analyzing these images for incidental noncardiac findings.
Incidental noncardiac findings occasionally are detected on review of projectional 99mTc-sestamibi myocardial perfusion images (1). Here, we report a case in which a large abdominal photopenic area was found on myocardial perfusion imaging in a patient with a history of autosomal dominant polycystic kidney disease.
CASE REPORT
A 69-y-old man was seen in our cardiology specialty office for evaluation of symptoms of shortness of breath with exertion and abnormalities found on a standard exercise test. He had experienced occasional symptoms of dyspnea with exertion during the past 3 mo. He denied symptoms of exertional or rest chest pain. His cardiac risk factors included a history of borderline hypertension and a family history of cardiac disease. The past medical history was significant for known autosomal dominant polycystic kidney disease. He had been found to have large renal and hepatic cysts on an earlier CT scan and was undergoing nephrology evaluation for moderate renal insufficiency.
On physical examination the blood pressure was 121/82 mm Hg, the heart rate 72 beats per minute, and the respiratory rate 16 breaths per minute. The lungs were clear to auscultation. On cardiac examination, there was a regular rhythm with a soft systolic murmur at the left sternal border. On abdominal examination, there was mild diffuse distention without tenderness to palpation.
The electrocardiogram showed sinus rhythm and nonspecific ST-T changes. A recent standard exercise treadmill stress test had demonstrated abnormal electrocardiographic changes at peak exercise in the inferior and lateral precordial leads.
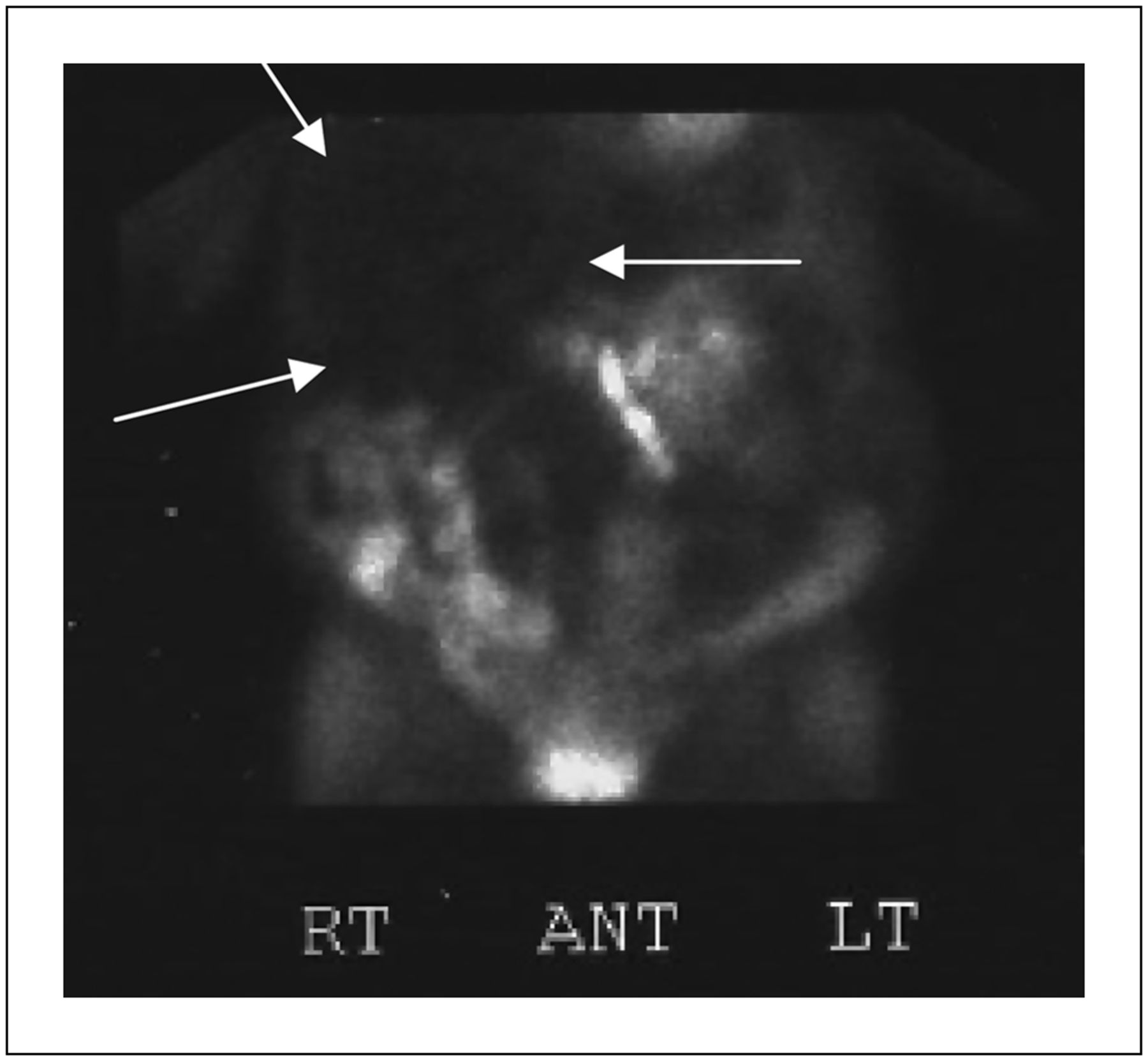
In light of the patient’s symptoms and electrocardiographic abnormalities observed on standard stress testing, repeated treadmill stress testing was performed in conjunction with same-day stress–rest 99mTc-sestamibi myocardial perfusion imaging. The patient reached an exertional level of 10 metabolic equivalents and 100% of maximum predicted heart rate without symptoms of chest pain. Abnormal electrocardiographic changes were again observed in multiple leads at peak heart rate. Gated SPECT myocardial images showed normal left ventricular wall motion with an ejection fraction of 58%. There was normal myocardial perfusion on both stress and rest images, with no evidence of stress-induced ischemia. Review of the unprocessed rotating projectional images, however, demonstrated a large photopenic area within the left and mid abdominal regions (Fig. 1). This was better visualized in an anterior static image acquired at the abdominal and pelvic regions (Fig. 2). Comparison of these findings to an earlier abdominal CT scan demonstrated that the location of the photopenic area corresponded to large hepatic cysts consistent with the patient’s known polycystic kidney disease (Fig. 3).
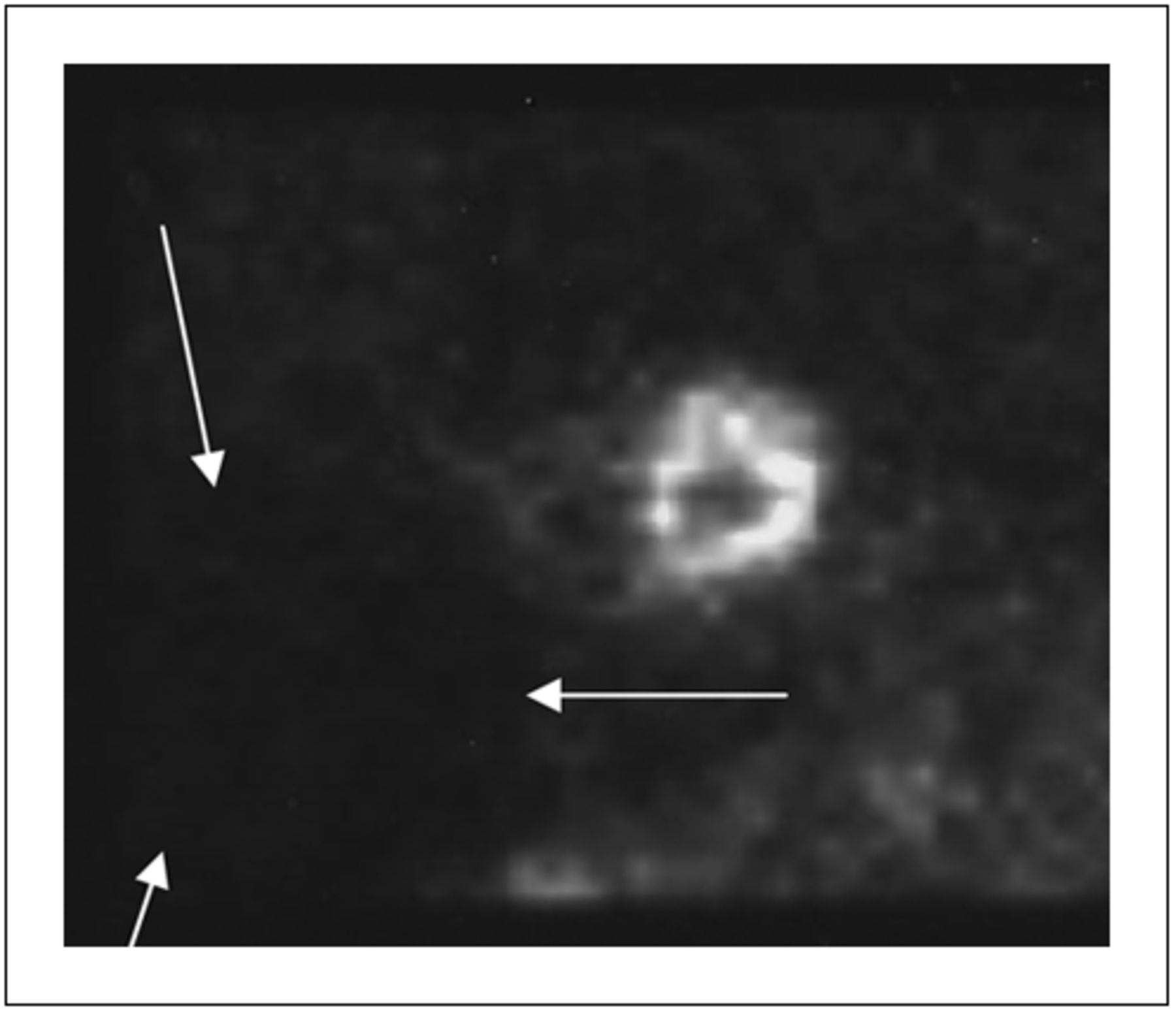
Anterior view of unprocessed projectional images showing large photopenic area within left and mid abdominal regions (arrows).
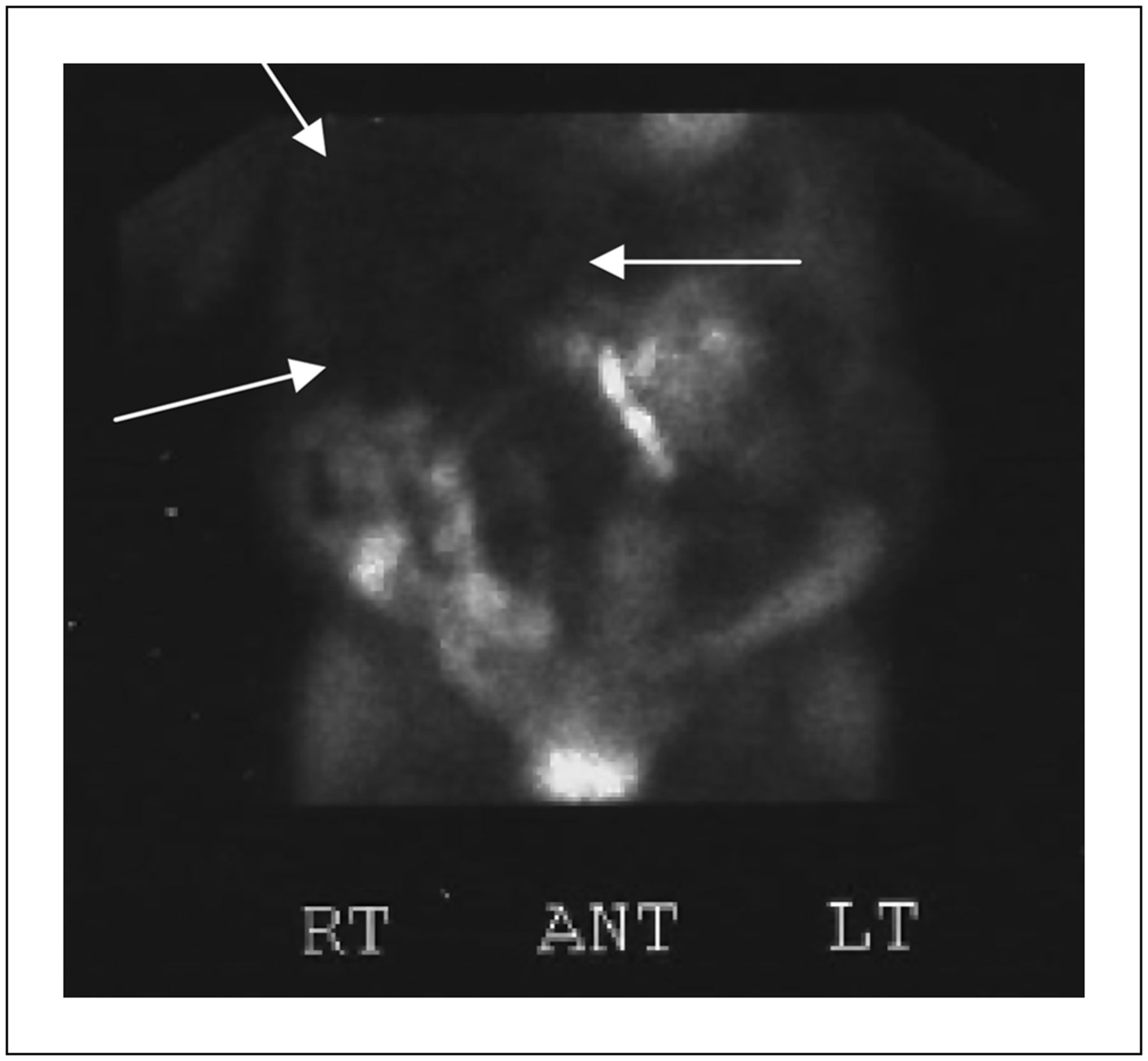
Anterior static image acquired at abdominal and pelvic regions demonstrating large photopenic area (arrows).
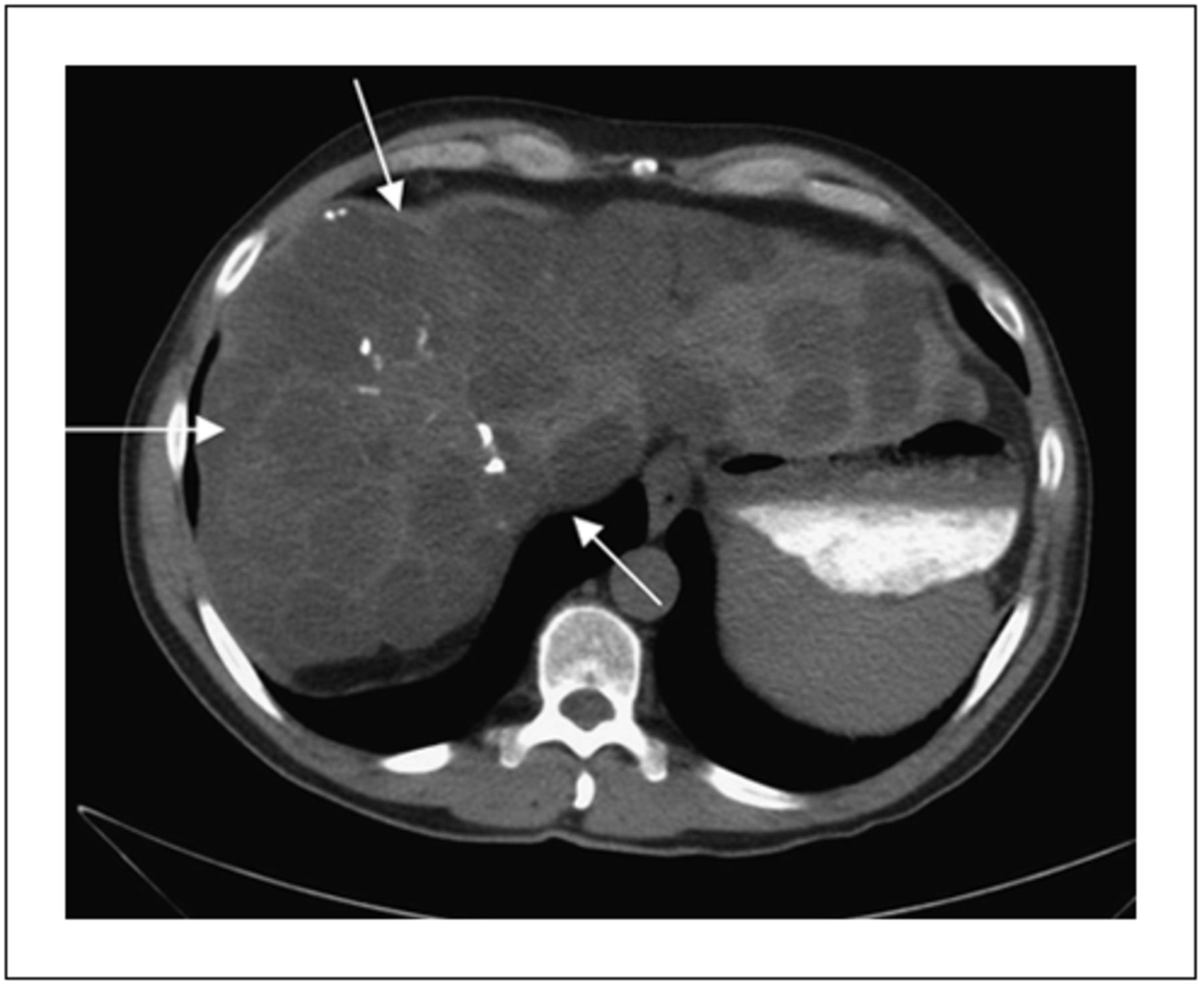
Anterior view of abdominal CT scan demonstrating large hepatic cysts (arrows).
DISCUSSION
Our patient was known to have autosomal dominant polycystic kidney disease, which commonly results in large and multiple renal and hepatic cysts (2). As in our case, these cysts can appear as abdominal photopenic areas on 99mTc-sestamibi imaging (3). Large abdominal photopenic areas are also seen with other types of renal cysts, including acquired cystic renal disease found in patients with end-stage renal disease receiving dialysis and with simple renal cysts (4,5). Other types of hepatic cysts may also result in large abdominal photopenic areas on myocardial perfusion imaging, including simple hepatic cysts and echinococcal cysts (6). Cholecystitis has also been reported to result in an abdominal photopenic area on myocardial perfusion scans (7). When further diagnostic imaging reveals a large solitary cyst, additional investigation may be required to exclude abscess, hematoma, or malignancy (6).
CONCLUSION
This case demonstrates the importance of careful analysis of the rotating unprocessed projectional images in the interpretation of myocardial perfusion imaging. Although the diagnosis of polycystic kidney disease was previously established in our patient, the incidental finding of an extracardiac photopenic area may constitute the first indication of a clinically significant abdominal abnormality.
Acknowledgments
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Sep. 20, 2012.
REFERENCES
- Received for publication December 18, 2011.
- Accepted for publication April 2, 2012.





{kind=link}
{kind=link}
{kind=link}