


Abstract
Our objective was to evaluate the impact of acquisition time on image quality, lesion detection rate, standardized uptake values, and lesion volume for 18F-FDG PET in cancer patients. Methods: Over 7 mo, 33 cancer patients were included in this study. In these patients, 63 lesions were independently evaluated by 2 nuclear medicine specialists (experienced and beginner). Two consecutive whole-body 18F-FDG PET/CT scans using a 3-min and 1.5-min acquisition time per bed position were obtained for each patient. Lesions were visually identified, and their locations were compared. The lesion volumes and standardized uptake values of the primary tumor, lymph nodes, and metastases were determined and compared. Image quality was scored using a 5-range Likert-type scale. For all parameters, interobserver agreement was assessed. Results: All relevant lesions could be identified at both acquisition times. Image quality was slightly adversely affected by an acquisition time of 1.5 min but was excellent or good in 85% of the scans. In a patient with increased blood sugar levels, the image quality was rated moderate at 3 min and poor at 1.5 min. The quality of lesion visualization was excellent regardless of the acquisition time. Lesion volume and maximum standardized uptake value on PET images showed an excellent correlation between the 2 acquisition times (Pearson correlation coefficient, 0.99 and 0.97, respectively). Interobserver agreement was excellent (κ > 0.83). Conclusion: Although image quality is slightly poorer, reducing the acquisition time to 1.5 min per bed position seems to be clinically feasible without decreasing the lesion detection rate even for less experienced observers.
PET using 18F-FDG has become a well-established and highly sensitive method to provide fast, comprehensive, and reliable information, particularly in oncology, cardiology, and neurology (1–4). However, PET/CT is still a rather time-consuming examination, and obtaining examinations of adequate image quality is commonly challenging, particularly in elderly patients, orthopedic patients, and pediatric patients. Without effective positioning aids, patient motion can cause misalignment (1). When a patient is in pain or anxious, the staff is often forced to enter the examination room to adjust the positioning or to calm the patient and then receives unnecessary radiation exposure. Thus, reducing the scanning time could help to increase patient comfort and the cost-effectiveness of the examination.
In general, higher numbers of coincidental radioactive decays can be registered when acquisition times are longer, and consequently, spatial resolution is better. Phantom studies suggest that even moderate increases in lesion contrast and signal-to-noise ratio considerably increase the lesion detection rate (5).
However, to our knowledge, a systematic study to establish a lower limit for acquisition times in clinical oncology has not been performed. So far, preliminary results from small clinical studies have been contradictory regarding impairment of lesion detection rates and maximum standardized uptake value (SUVmax) if scanning time is reduced below 3 min per bed position (6,7).
One aim of this study, therefore, was to further evaluate image quality with a reduced acquisition time using modern 3-dimensional high-definition PET scanners. Another aim was to verify whether it is feasible to decrease the acquisition time to below 3 min per bed position without substantially reducing the lesion detection rate and diagnostic image quality, even for less experienced observers.
MATERIALS AND METHODS
Patients and Lesions
Over 7 mo, 33 patients with advanced cancer who required a whole-body 18F-FDG PET/CT examination for cancer staging were included in this study. The local ethics committee approved the study, and all participants gave their written informed consent. Patient exclusion criteria were pregnancy, age less than 18 y, diabetes type I, and blood glucose level greater than 180 mg/dL. Patients with a bad general state of health were also excluded because of the prolonged examination time.
18F-FDG PET/CT Protocol
Patients fasted for at least 8 h before 18F-FDG was injected intravenously (body weight–adapted, with 300 MBq for a 70-kg patient). Blood glucose levels were measured before the injection. All patients maintained an uptake phase that allowed tracer to accumulate in relevant lesions (mean, 330 ± 33 MBq). The mean duration of the uptake phase was 80 min (range, 54–132 min) for the 3-min scan and 90 min (range, 50–146 min) for the 1.5-min scan.
Patients were imaged on the Biograph mCT (Siemens Healthcare Sector) with 5.0-mm spatial resolution in 3-dimensional mode. The system consists of 3 detector rings with an axial coverage of 16 cm. For whole-body PET/CT from the skull to the mid thighs, 8 different bed positions were necessary in most cases. First, a low-dose helical CT scan to correct attenuation was acquired during shallow breathing (using CARE Dose4D [Siemens], which automatically adapts radiation dose to the size and shape of the patient: 50 mA, 120 kVp, pitch of 0.8, and collimation of 1.2 mm) with the arms over the head. Immediately thereafter, PET was performed beginning from the mid thigh. The order of the 2 PET scans was randomized. In 18 of 33 patients (55%), scanning at 3 min per bed position was performed first. Patients in whom diagnostic imaging had not been recently performed were subsequently examined using contrast-enhanced diagnostic CT and body weight–adapted iodinated intravenous contrast medium (Imeron 320; Bracco). In patients who had recently undergone diagnostic CT, no further contrast-enhanced CT was performed; instead, the radiation dose of the attenuation-corrected CT was increased to the CARE Dose4D–adapted 80 mA so as to give an adequate image quality for correlating the morphologic results on CT scans and the PET images. We also corrected for the dead time of the PET system and for random and scatter events. In all patients, only 1 attenuation-corrected CT scan was obtained and used for both PET acquisitions. Patients had no additional radiation exposure.
Images were interpreted at a workstation equipped with fusion software that can display CT, PET, and PET/CT images (MMWP, VE31A; Siemens Medical Solutions). All PET/CT images were read by a board-certified nuclear medicine specialist and a first-year nuclear medicine resident, neither of whom knew the acquisition time of the images. The primary tumor, a maximum of 5 lymph node metastases, and a maximum of 2 lesions per organ (maximum of 5 metastases), adapted to the Response Evaluation Criteria in Solid Tumors, 1.1, were assessed (8).
Image quality was scored on a 5-point Likert-type scale as follows: 1, excellent quality; 2, good quality; 3, moderate quality; 4, poor quality; and 5, very poor image quality. Lesions were visually identified. The quality scoring was based on individual subjective image perception. Objective criteria were image blurring (background uptake) and, in terms of the quality of lesion visualization, the relation of lesion uptake to background uptake. Other criteria were the sharpness of angles of anatomic structures other than the lesions for determination of overall image quality.
For the quantitative outcome, tumor uptake was measured using SUVmax, and lesion volumes were determined. Volumes of interest were placed around the lesions to estimate volume with an SUV threshold of 2.5. SUVmax was computed after tissue radioactivity had been normalized to the decay-corrected injected dose and body weight.
Statistics
κ-statistics were obtained to evaluate overall image quality and the quality of lesion visualization at both acquisition times. Pearson correlation coefficients were measured and t tests performed to compare the lesion volumes and SUVmax. Statistical evaluation of the image quality and lesion detection rate was based solely on the results of the board-certified nuclear medicine specialist. Interpretation data from the first-year nuclear medicine resident were used to assess interobserver agreement only. κ-statistics were obtained to evaluate interobserver variability.
For comparison of acquisition times, the results of the 3-min scan served as the reference.
RESULTS
Patients and Lesions
In all, 33 patients were included in this study (18 men and 15 women; mean age, 61 y; range, 36–83 y). In these patients, a total of 63 lesions were assessed. Primary tumors were bronchial carcinomas (n = 13); ear, nose, and throat tumors (n = 8); anal cancers (n = 3); breast cancers (n = 2); gastrointestinal stromal tumors (n = 2); esophageal cancers (n = 2); cervical cancer (n = 1); pleural mesothelioma (n = 1); and colorectal cancer (n = 1).
Image Quality and Lesion Detection Rate
All relevant lesions could be identified at both acquisition times (Table 1; Fig. 1). Image quality was slightly lower in the scans with an acquisition time of 1.5 min (κ = 0.16); nevertheless, the image quality was rated as excellent or good in 85% of those scans. In an obese patient with an increased blood sugar level of 148 mg/dL, image quality was rated as moderate at 3 min and poor at 1.5 min (Fig. 2). The quality of lesion visualization was excellent regardless of the acquisition time (κ = 0.59) (Table 2; Fig. 1).
Comparison of Overall Image Quality for All 33 Patients
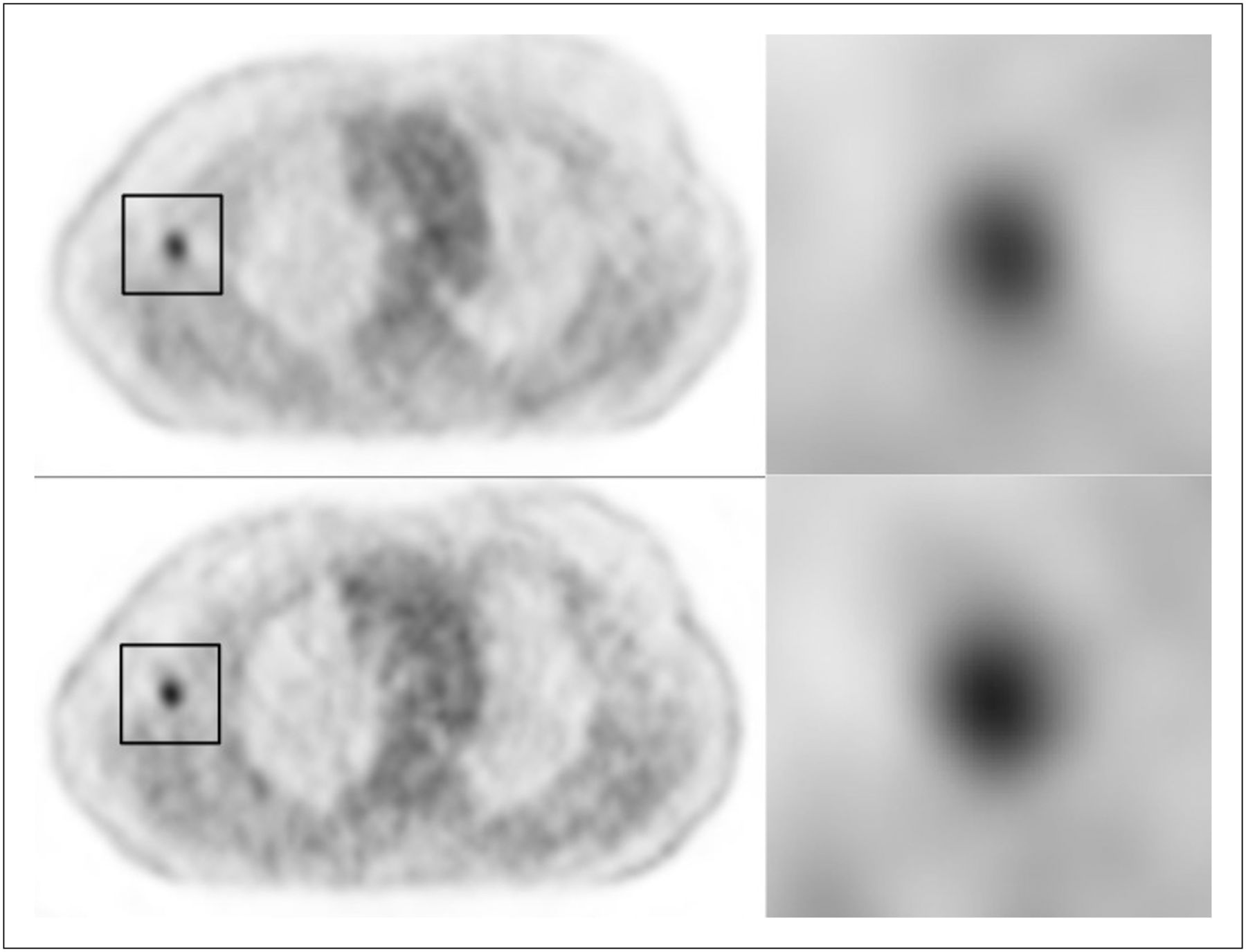
18F-FDG PET/CT images of 75-y-old woman with advanced lung cancer and lymph node metastases. Metastatic lymph node in right axilla (box) is clearly identifiable on 3-min scan (top) and 1.5-min scan (bottom). Image quality of 1.5-min scan is slightly reduced as result of more pronounced blurring.
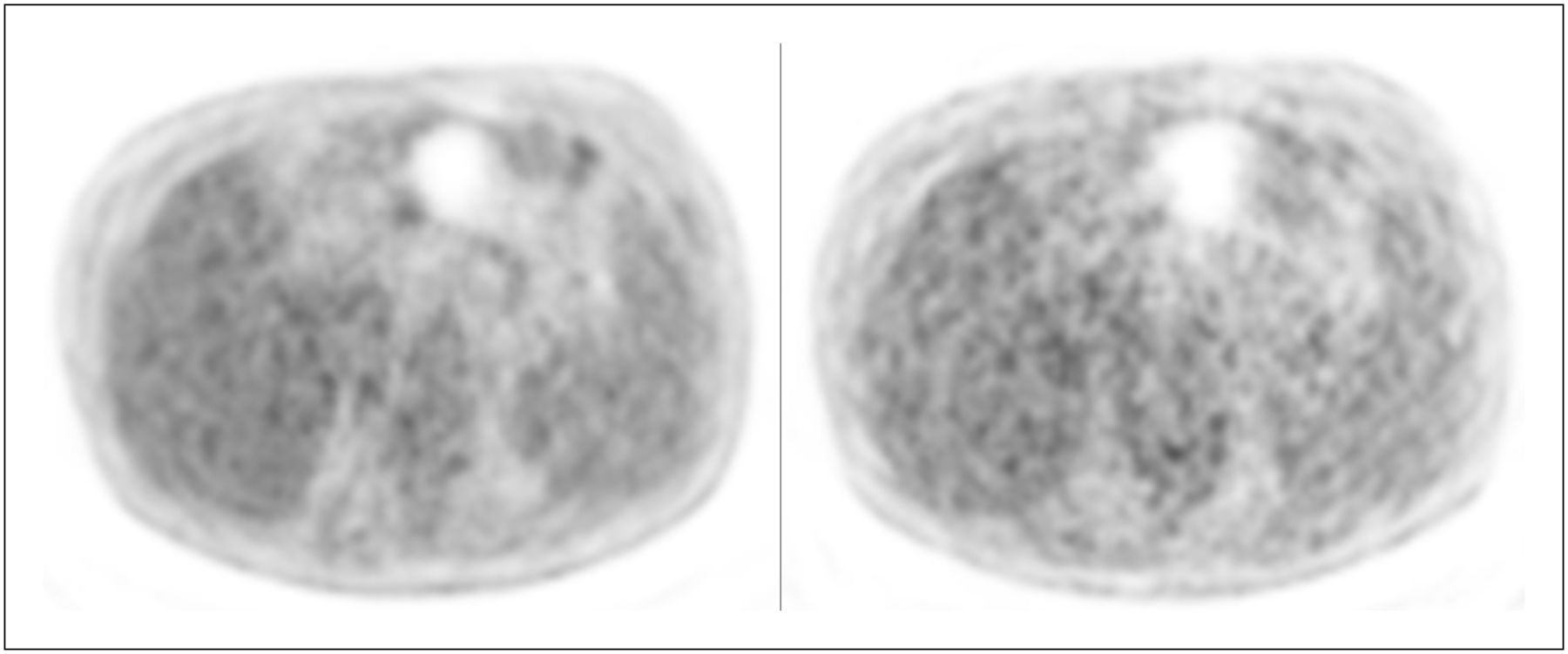
Axial PET images of obese patient with increased blood sugar (148 mg/dL). Left image was acquired at 3 min per bed position; right image, at 1.5 min per bed position. Image quality was considerably reduced for both acquisition times and was rated poor for 1.5-min scan, which could be relevant in critical regions such as upper abdomen.
Comparison of Quality of Lesion Visualization for All 63 Lesions
Lesion Volume
Correlation of lesion volumes on PET images between the 2 acquisition times was excellent (Pearson correlation coefficient, 0.99). The mean lesion volume was 38.6 cm3 (SD, 82.7; range, 0.05–503.2 cm3) for the 3-min scan and 39.4 cm3 (SD, 83.8; range, 0.01–496.9 cm3) for the 1.5-min scan. The t test did not show a significant difference between the 2 scan times (P = 0.13).
SUVmax
SUVmax correlated well between the 2 acquisition times (Pearson correlation coefficient, 0.97). The mean SUVmax was 13.5 (SD, 8.2; range, 2.3–46.3) for the 3-min scan and 13.5 (SD, 7.7; range, 2.2–40.0) for the 1.5 min scan (Fig. 2). The t test did not show a significant difference between the 2 scan times (P = 0.91).
Interobserver Correlation
The lesion detection rates did not differ between the board-certified nuclear medicine specialist and the first-year nuclear medicine resident. Image quality was scored exactly the same for the 3-min scans. Image quality was rated slightly worse by the less experienced observer on the 1.5-min scans (κ = 0.83).
DISCUSSION
This study shows that it is clinically feasible to reduce acquisition times from 3 to 1.5 min per bed position by using modern 3-dimensional high-definition PET/CT scanners. Image quality was only slightly adversely affected by the shorter acquisition time, and lesion detection rates were not lower, even for less experienced observers.
Although phantom studies suggest that lesion detection rates can be increased considerably with only moderate increases in objective imaging parameters, the clinical impact of these findings has not been evaluated yet. For example, in vitro data of Farquhar et al. (5) showed that scan duration was the most significant predictor of contrast-to-noise ratio variance. They showed that increasing the scan time from 1 to 4 min per bed position was most effective for obtaining higher contrast-to-noise ratios. Imaging a thorax phantom using 3 sizes of spheres to simulate lesions (0.45, 1.0, and 1.9 mL), the authors found that less than a 2-fold increase in contrast was required to improve detection performance from poor to excellent.
In vitro and in vivo data from Brown et al. (7) are in line with these findings. They performed a quantitative and qualitative analysis based on 3-dimensional 18F-FDG phantom and patient PET images and detected a trend toward fewer lesions being detected under decreased acquisition time conditions. Phantom images were acquired for 1-, 2-, 3-, 4-, and 5-min time frames with different lesion-to-background contrast ratios. Patient data were investigated using list-mode acquisition to obtain comparable 2-, 3-, and 4-min frames. In both phantom and patient images, qualitative and quantitative analysis showed that image quality was poorer below the 4-min acquisition frames. In patient images, 1 lesion detected during a 4-min acquisition could not be detected in a 3-min acquisition and another 4 lesions were missed on images acquired in a 2-min period. The authors concluded that the acquisition time frame should not be reduced to below 3 min for standard 3-dimensional-mode 18F-FDG imaging. However, the number of patient PET images was small (n = 10) and the clinical impact of the finding needs to be further investigated.
Our results suggest that these in vitro findings are less significant for diagnostic imaging in oncology than previously assumed. To the best of our knowledge, our clinical study on PET/CT image quality and acquisition times is the largest patient cohort published so far. In our study, low contrast-to-noise ratios, because of a shorter acquisition time of at least 1.5 min, did not seem to significantly influence lesion detection rates. We also found that SUVmax did not vary significantly within the scan times of 1.5 and 3 min. Our results were also confirmed in a recent clinical study by Goethals et al. (6) and an earlier study by Farquhar et al. (5). Assessing 17 head-and-neck cancer patients with acquisition times ranging from 10 to 0.5 min, the investigators demonstrated that a reduced image quality did not adversely affect the visual identification of malignant lesions in the head-and-neck region.
Our PET scanner is equipped with high-definition PET technology using advanced iterative reconstruction algorithms that have been commercially available since 2007. This technologic advance and the substantially higher tracer uptake in malignant lesions (9) may have contributed to our results.
Our results suggest, in accordance with the study of Goethals et al. (6), that 18F-FDG uptake can be semiquantitatively compared for the 2 scan times. This is important because SUVs are used to distinguish between benign and malignant lesions and changes in SUVs serve to monitor response to therapy.
Moreover, size may be of particular interest if PET images are used in radiation oncology treatment planning (6). Accurate delineation of target volumes is important to maximize radiation dose to the tumor and minimize it to nontumor tissue (10). Our data demonstrate that the PET/CT volumes measured were not significantly influenced by the duration of the acquisition. Nevertheless, the lesion size was slightly altered with respect to the acquisition time, with a slight increase in size at 1.5 min. This finding can be explained by a more relevant blurring at 1.5 min caused by a reduced number of coincidental radioactive decays registered at shorter acquisitions.
Another important aspect that supports the immense value of PET/CT in tumor staging is the low interobserver variability. Indeed, observer variability can be high in a CT-based definition of the gross tumor volume. A more consistent definition of the gross tumor volume can often be obtained if coregistered 18F-FDG PET images are used (11). A survey on the interobserver variability of SUVmax and SUVmean measurements on 18F-FDG PET/CT scans in patients with focal pulmonary lesions showed that the SUVmax of lung nodules can be calculated without any interobserver variation (12).
Our study had several limitations. First, we did not obtain histopathologic proof of our findings. Moreover, even though the results of the objective data (SUVmax and lesion volume) indicated an excellent correlation between the 2 scan times on statistical evaluation, the group size of 33 patients is still relatively small.
Further technical improvements will most certainly help to further reduce scanning time. New technologic developments such as a larger field of view, the use of a 4-row full-ring detector system, and the use of time-of-flight (13) technology could dramatically reduce whole-body examination time. The time-of-flight projections that are organized in time bins along each line of response achieve a better estimate of the actual image with much less blurring. Future studies will be needed to assess the effectiveness of these technical developments.
CONCLUSION
In addition to the findings of Goethals et al. (6), Caldwell et al. (11), and Huang et al. (12), our results demonstrate that acquisition times can likely be lowered without reducing the lesion detection rate in different tumor entities even for less experienced observers, although image quality was rated slightly worse at 1.5 min by the less experienced observer.
On the basis of our experience, we would rather be careful in reducing acquisition time in obese patients or patients with increased blood sugar levels, particularly in critical regions such as the upper abdomen.
Acknowledgments
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Oct. 15, 2012.
REFERENCES
- Received for publication January 17, 2012.
- Accepted for publication April 2, 2012.





{kind=link}
{kind=link}