


Article Figures & Data
Figures
- FIGURE 1.
18F-FDG PET/CT for initial staging of patient A’s laryngeal cancer. (A) Maximum-intensity projection demonstrates single focus of hypermetabolic activity at location of laryngeal cancer with no evidence of locoregional spread of distal metastases. (B) CT shows abnormal soft-tissue mass (arrow) along anterior aspect of left vocal cord. (C and D) Axial attenuation-corrected PET and PET/CT, respectively, demonstrate that lesion is hypermetabolic, consistent with known diagnosis of squamous cell carcinoma.
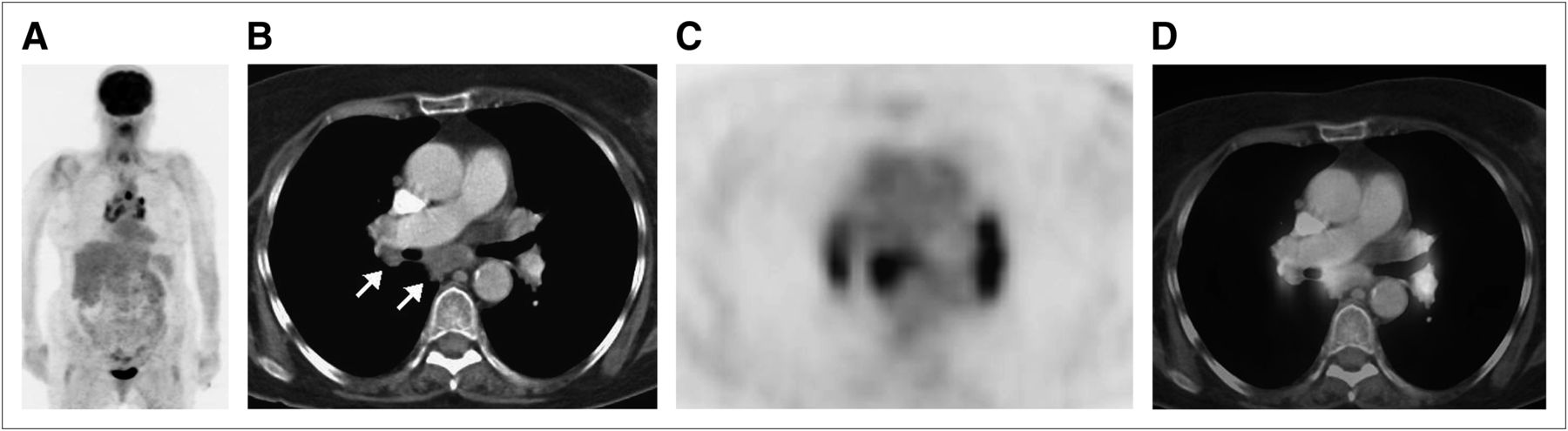
- FIGURE 2.
Follow-up 18F-FDG PET/CT for routine surveillance of patient A’s laryngeal cancer. Clinically, patient had no evidence of disease. (A) Maximum-intensity projection demonstrates bilateral abnormal 18F-FDG avidity in hilar regions and mediastinum. (B–D) Axial CT, PET, and PET/CT through hila and mediastinum show these foci to correspond to hypermetabolic lymph nodes (arrows).
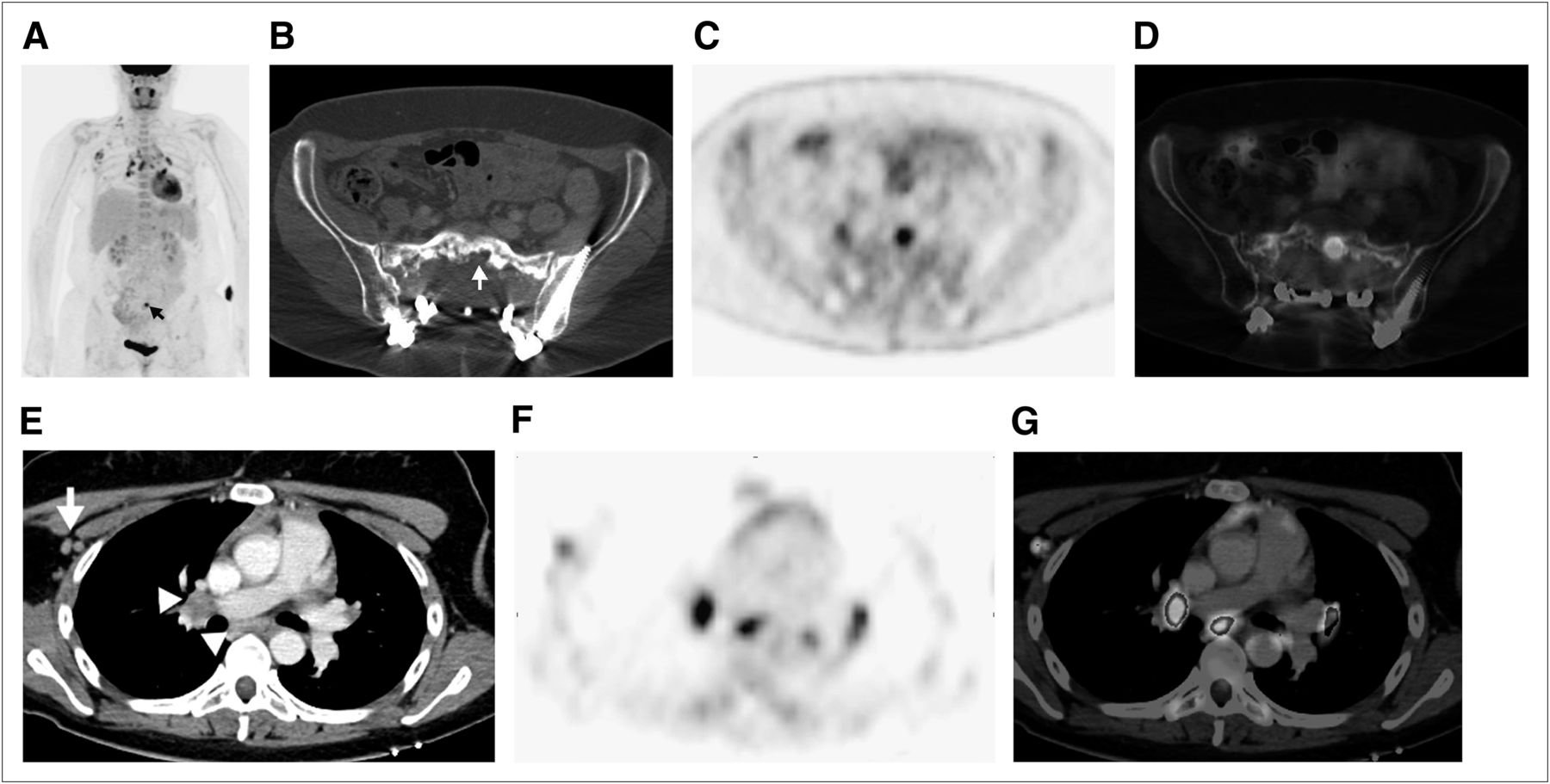
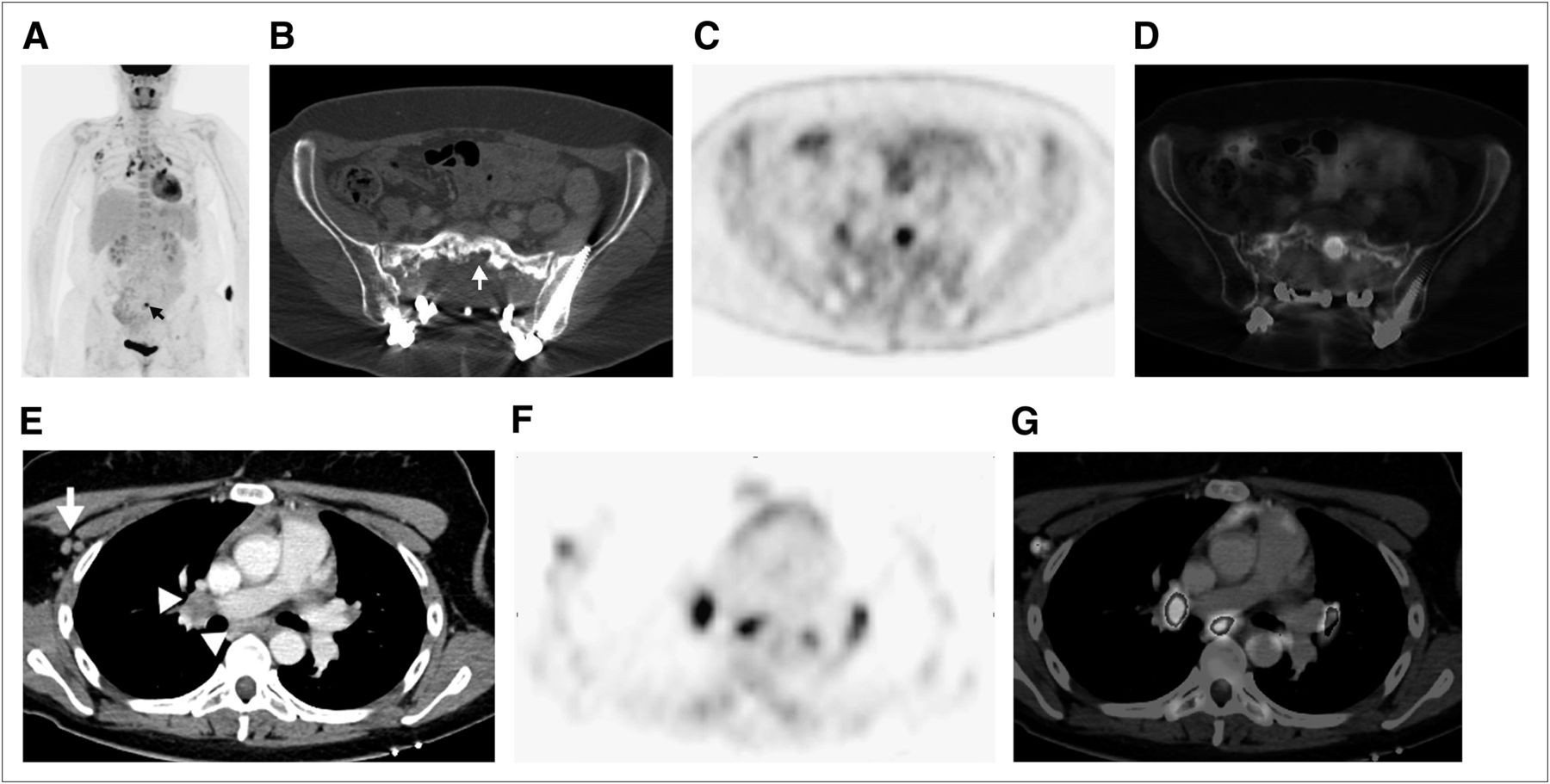
- FIGURE 3.
(A) Maximum-intensity projection from follow-up 18F-FDG PET/CT done for routine surveillance of patient B demonstrates abnormal 18F-FDG avidity in sacrum at site of prior disease (arrow). (B, C, and D) Axial CT, PET, and PET/CT, respectively, show that sacral activity corresponds to new hypermetabolic osteolysis consistent with local recurrence. The combination was believed to represent local recurrent disease. Additional findings on maximum-intensity projection included new, bilateral hypermetabolic foci in hilar regions and mediastinum, as well as in right axilla and right neck base. (E, F, and G) Axial CT, PET, and PET/CT, respectively, show these foci to represent hypermetabolic hilar and mediastinal (arrowheads) and right axillary (arrow) lymph nodes. Foci of uptake in right neck base were also shown to be hypermetabolic lymph nodes.


Tables
Entity Clinical features CT features Sarcoidlike reaction History of prior malignancy; entity may occur at time of initial cancer diagnosis to years later, often with no clinical evidence of disease No pulmonary changes; patient classically shows bilateral mild to moderately enlarged hilar and mediastinal lymph nodes; enlarged or hypermetabolic lymph nodes may be present elsewhere Sarcoid Bias toward young and middle-aged African–American women; clinical complaints often include erythema nodosum, uveitis, and acute polyarthritis, with nonspecific respiratory symptoms, fatigue, weight loss, and fever Pulmonary findings may often be absent though when present show nodular pattern along lymphovascular bundles; patient classically has bilateral lobulated, mild to moderately enlarged hilar and mediastinal lymph nodes; lymph nodes may have peripheral thin egg-shell calcifications Pneumoconiosis History of occupational exposure such as surface mining; patient may be asymptomatic early on and then develop shortness of breath and respiratory symptoms along with pulmonary changes Diffuse reticular or nodular/reticulonodular pattern of pulmonary disease; lung findings can coalesce into massive pulmonary fibrosis; lymph nodes often have egg-shell calcifications Infection No age or sex predilection; signs and symptoms of respiratory infection are present (i.e., fever, productive cough, leukocytosis, and elevated C-reactive protein) Pulmonary features of infection (bronchopulmonary nodules, infiltrate, or consolidation); lymph nodes ipsilateral to pulmonary abnormality are typically at upper limit of normal size to mildly enlarged Radiation-induced inflammation History of prior malignancy with treatment by radiotherapy; patient may be asymptomatic or have dyspnea or nonproductive cough Sharply marginated, localized fibrotic area of lung; lymph nodes ipsilateral to fibrosis are normal to mildly enlarged Lymphoma Age predilection based on type of lymphoma; patient may present with weight loss, night sweats, fever, decreased appetite Rarely has pulmonary findings; marked nodal enlargement is often bilateral though may be asymmetric; conglomerate nodal masses may be present Bronchogenic carcinoma Older individuals, often with history of smoking or pulmonary fibrosis, present with weight loss, decreased appetite, hemoptysis Lung mass or nodule; nodal enlargement is typically ipsilateral to lesion Metastases History of malignancy, possibly with increasing tumor markers suggestive of disease recurrence; is most commonly seen in tumors with predilection for mediastinal or hilar metastases (i.e., esophageal cancer or head and neck cancer) Lymph nodes often asymmetric or unilateral; evidence of metastases may be present in lungs, bones, or elsewhere





{kind=link}
{kind=link}
{kind=link}