


Abstract
As hospital nuclear medicine departments were established in the 1960s and 1970s, each department developed detailed policies and procedures to meet the specialized and specific handling requirements of radiopharmaceuticals. In many health systems, radiopharmaceuticals are still unique as the only drugs not under the control of the health system pharmacy; however, the clear trend—and now an accreditation requirement—is to merge radiopharmaceutical management with the overall health system medication management system. Accomplishing this can be a challenge for both nuclear medicine and pharmacy because each lacks knowledge of the specifics and needs of the other field. In this paper we will first describe medication management standards, what they cover, and how they are enforced. We will describe how we created a nuclear medicine and pharmacy team to achieve compliance, and we will present the results of their work. We will examine several specific issues raised by incorporating radiopharmaceuticals in the medication management process and describe how our team addressed those issues. Finally, we will look at how the medication management process helps ensure ongoing quality and safety to patients through multiple periodic reviews. The reader will gain an understanding of medication management standards and how they apply to nuclear medicine, learn how a nuclear medicine and pharmacy team can effectively merge nuclear medicine and pharmacy processes, and gain the ability to achieve compliance at the reader's own institution.
Modern nuclear medicine was born about 50 y ago with patenting of the Anger scintillation camera (1961) and introduction of 99mTc as an ideal medical tracer (1960) (1,2). Most of the growth in nuclear medicine over the last half century has been the direct result of the introduction of new radiopharmaceuticals. Many of these agents (hepatobiliary agents, bone tracers, sestamibi, macroaggregated albumin, 18F-FDG, and others) were revolutionary advances in functional imaging, leading to clinical use of multiple radiopharmaceuticals in most nuclear medicine departments. Many nuclear medicine procedures also use a variety of nonradioactive drugs (pharmacologic stress agents, cholecystokinin analog, furosemide, and others). As a result, most health system nuclear medicine departments today routinely dispense dozens of different radiopharmaceuticals and other medications (Fig. 1).

Most modern nuclear medicine departments routinely use many different radioactive and nonradioactive pharmaceuticals. Medication management standards ensure that this use is safe and efficacious.
Historically, radiopharmaceuticals have been managed separately from other medications in many health systems. Because of their radioactivity, radiopharmaceuticals require special handling within the medication use process and their own special procedures and safeguards to ensure safe and effective use. As nuclear medicine departments were established and evolved, many developed their own radiopharmaceutical policies and procedures intended to avoid improper administration and ensure safe use. Concurrently, many health system pharmacy departments, working hard to meet increasingly rigorous and expanding standards, have been slow to tackle the additional issues posed by radioactive agents. Contributing to the lack of pharmacy oversight of radiopharmaceuticals in many health systems has been the perceived safe record of radiopharmaceutical use in most hospitals. As a result of both these factors, radiopharmaceuticals are still routinely managed solely by nuclear medicine in several U.S. health systems. The nuclear medicine section at Christiana Care Health System was a case in point until recently. The section was established in 1952 and operated under its own medication use policies while providing nuclear medicine services at 2 hospitals (1,148 licensed beds) and 2 outpatient facilities.
Over the last several decades, most nuclear medicine departments have compiled good records of safe and effective radiopharmaceutical use (3–5). However, there is a movement toward integrating medication management practices and standardizing approaches for all medications used within health systems. The new measures promise to further improve the safety and quality of imaging procedures, occupational handling, and medication management. One example is the requirement that nuclear medicine hot labs meet U.S. Pharmacopeia 797 standards for pharmaceutical compounding conditions (6). Another is the requirement that radiopharmaceutical use in the health system comply with the Centers for Medicare and Medicaid Services (CMS) conditions of participation (CoPs) for Medicare and the medication management standards as set forth by the Joint Commission (TJC) or other accrediting organizations (6–8). These CoPs and standards call for radiopharmaceuticals to follow the same systems, controls, and oversight by a pharmacist as other medications used in a health system to ensure safety and quality (6,7). Christiana Care Health System maintains accreditation through TJC. Health system medication management systems have met or exceeded TJC standards historically; however, radiopharmaceuticals, managed under a stand-alone system by nuclear medicine, had not been included in previous reviews or gap analyses. When our section learned that radiopharmaceuticals would be required to be under the health system medication management system on the next accreditation cycle, we were concerned. We envisioned a jungle of onerous pharmacy regulations that could compromise the function of a busy nuclear medicine department. We were concerned about what the standards would require, and we worried that pharmacy personnel had no understanding of the unique issues involved with handling radioactive substances. Through a collaborative initiative with our health system pharmacy, we were able to find a path through the jungle—we achieved compliance with all standards in a relatively short time without compromising the function of our department.
In this paper we will give an overview of what medication management standards are, how they are enforced, and what they require. We will show how a collaborative project between nuclear medicine and pharmacy is an effective strategy to achieve compliance with the medication management standards. We will examine some of the particular challenges to standard medication management posed by nuclear medicine and radiopharmaceuticals and share the approaches we took to meet those challenges.
What Are Medication Management Standards?
Government regulations and independent health care quality and accreditation organizations in the United States establish standards for all aspects of operation in health care facilities, including medication use. For example, health care organizations are required to meet specific standards aimed at protecting the health and safety of Medicare and Medicaid beneficiaries to participate in Medicare and Medicaid programs and thereby receive reimbursement (7). Comprehensive CoPs for health care facility operations are promulgated by the CMS, a federal agency under the U.S. Department of Health and Human Services. These CoPs broadly cover all aspects of operation of health care facilities, including how medications are used, and require that all medications used in a health care facility, including radiopharmaceuticals, be controlled by a comprehensive medication management system under the oversight of a pharmacist (7,8). These CoPs are adopted into standards that are surveyed by CMS-recognized organizations such as TJC. The medication management standards of different accrediting organizations show some variation in specifics, but all are designed to meet or exceed the CoPs established by CMS. The accrediting organizations are then responsible for ensuring that health care facilities meet the CMS CoPs. Complete detailed accrediting organization standards along with explanations for their elements of performance are provided to the health system administration and available in printed manuals and Web-based publications (6,7).
A Nuclear Medicine and Pharmacy Team
At the authors’ facilities, preparation and administration of radiopharmaceuticals are the responsibility of certified nuclear medicine technologists (CNMTs) with pharmacist oversight. Before the changes described herein, this was done outside the system's medication management system and without pharmacist involvement. We realized that bringing radiopharmaceutical management and overall medication management approaches into alignment would require expertise in both nuclear medicine and pharmacy practice, so we formed a team including staff from both departments. The team's guiding principle was that any solution considered must require that all medication management functions be performed in accordance with policies and procedures developed with pharmacy oversight and must also comply with the Nuclear Regulatory Commission (NRC) and state regulations.
The team first compiled a list of radioactive and nonradioactive agents already in use in nuclear medicine (Table 1) and initiated a collaborative pharmacist–physician review of all agents while simultaneously working to develop new policies and procedures. To determine what new policies and procedures were needed, the team performed a comprehensive gap analysis of current processes within the nuclear medicine section. This revealed that the section was fully compliant with only 21 of 77 TJC elements of performance for the standards we considered applicable. Thus, system redesign offered an opportunity for improvement. The team's task was to make those improvements without compromising nuclear medicine operations. This required learning on the part of all team members. The pharmacy team member needed to gain an understanding of nuclear medicine procedures and the special requirements of radioactive materials; similarly, nuclear medicine personnel needed to learn about pharmacy operations and the health system's medication management system and its formulary process.
Agents Used in a Typical Health System Nuclear Medicine Department
Contents of Medication Management Systems
Medication management systems may be divided into component processes. These are commonly divided into selection and procurement, storage, ordering and transcribing, preparing and dispensing, administering, and monitoring (8). These processes provide a framework for conceptualizing the medication management system, around which standards have been developed. Meeting or exceeding the standards for each of these processes ensures the safety and quality of the medication system and is now the required responsibility of the institution pharmacy. In the case of radiopharmaceuticals, aligning procedures in nuclear medicine and pharmacy is therefore of paramount importance.
Medication Selection—The Formulary Process
At Christiana Care Health System, as in most health systems, medication use is governed by the formulary process. The formulary is the complete list of medications approved for use at that facility. To be placed on the formulary, each proposed agent must be approved by a supervising body, usually a health system pharmacy and therapeutics committee (P&T), which includes representation from the medical staff, nursing staff, and pharmacy (usually the pharmacy director). The committee's function is to implement and maintain a safe, high-quality medication management system throughout the organization. This includes making sure that all medications proposed for use are safe and will be used in appropriate protocols. Medications must be approved and placed on the formulary before use. At Christiana Care, the criteria for evaluating medications for formulary inclusion include the medication's indications for use; clinical information on effectiveness; risk information such as adverse drug events, drug interactions, and potential for error and abuse; product quality; cost; and TJC sentinel event advisories (9). Addition, deletion, and substitution of medications as well as proposal of new or modified protocols incorporating medications all require committee approval (10). Use of products not on the formulary is strongly discouraged and must be managed under special rules. The formulary process and individuals who oversee it operate under standardized systems to gather information, assess agents and protocols, and thereby ensure safety and quality.
Current standards require that radiopharmaceuticals be rigorously reviewed and approved for the formulary, as is done for other medications. This requires merging the selection process for radiopharmaceuticals into the overall formulary process. The responsibility for radiopharmaceutical selection therefore shifts from solely nuclear medicine staff to the overall medical staff through the P&T committee. We found that the standardized procedures already in place for formulary review of proposed medications facilitated this transition. Most health system pharmacy departments have established systems to gather, present, and assess information on proposed medications. The existing systems can be leveraged to ensure that radiopharmaceutical selection and management meet clinical needs while minimizing safety and quality concerns.
Information on medications proposed for formulary inclusion may come from various sources. Radiopharmaceutical package inserts provide most of the basic data required on each agent. Many health system pharmacies subscribe to services that provide standardized data and reports on medications. The service used through license by our pharmacy, LexiComp Online (a product of Lexi-Comp, Inc.), was able to provide monographs on many common radiopharmaceuticals and continue to update this section of their service. Radiopharmacy texts can also provide additional necessary information (11). Particular concerns arise with radiopharmaceutical uses that are not Food and Drug Administration–approved or are off-label indications. An example is use of 99mTc-sestamibi for parathyroid imaging. In situations such as this, published Society of Nuclear Medicine or European Association of Nuclear Medicine procedure guidelines, nuclear medicine textbooks, and review articles can provide support for particular radiopharmaceutical uses (12,13).
Nuclear medicine physician representation on the medical staff committee addressing medication management should be considered. Whether full membership or ad hoc/consultative membership is pursued will depend on the particular medical staff rules at a given organization. At the very least, a nuclear medicine physician should be present to give input and answer questions when the committee considers radiopharmaceuticals. We addressed this issue by creating an ad hoc position in the P&T committee membership structure for nuclear medicine representation for matters related to radiopharmaceuticals.
Radiopharmaceuticals elevated to formulary status at Christiana Care Health System are listed on the health system Intranet or in printed references making the relevant drug information available to all involved in the medication use process (14). Once a radiopharmaceutical is listed in the formulary, it may be used clinically and follows the institution's medication management policies under the supervision of the pharmacy.
Periodic review of many aspects of the system is a cornerstone of good practice in medication management. Radiopharmaceutical formulary selections, protocols, policies, and procedures should be reviewed at least annually to allow identification of trends or issues with particular agents or protocols that might not be apparent on a day-to-day basis. For formulary selection review, we established a system in which the nuclear medicine manager and a pharmacist with understanding of these medications formally review the radiopharmaceutical list annually and make recommendations to P&T for addition, deletion, and substitution based on internal experience and emerging safety and efficacy literature. In this review, imaging agents are assessed for clinical risks and risk for error. Those identified as presenting significant risks require alert procedures similar to those issued for other medications that cause concern. Consideration is also given to agents that are similar to each other in appearance, labeling, or name so that steps may be taken to minimize risk of errors. The nuclear medicine and pharmacy staff team also routinely reviews the high-alert medication list and list of confused drug names provided by the Institute for Safe Medication Practices and the hazardous medications list provided by the Centers for Disease Control and can intervene anytime throughout the year as warranted (15–17).
Procurement
Pharmacist oversight extends to procurement of selected agents. During our research, we found health system pharmacy departments are often not directly involved in the routine procurement of radiopharmaceuticals. Despite this, processes ensuring secure acquisition and transfer from reputable suppliers must be in place, as with other medications. Even if the procurement process is performed outside the pharmacy, pharmacist oversight of the process is still required. Our team's solution for this was to establish a process of review and audit of product invoices including description, quantity, product number, unit price, and charges from all sites, with feedback and input provided to the nuclear medicine leadership as warranted. Information for this review is obtained from the database of our nuclear medicine radiopharmaceutical management system and provided to the department lead for pharmacy.
Nuclear medicine departmental management systems can greatly facilitate compliance with health system medication management programs. These commercial software systems, often provided by radiopharmaceutical vendors, allow the nuclear medicine department to store and retrieve relevant information about orders, deliveries, and individual patient studies. This information is readily available to the management team in the pharmacy as well as internal or external auditing groups such as TJC, the NRC, and state agencies. Our nuclear medicine section uses a system called SYNtrac (18), which is provided by Cardinal Health, our principal radiopharmaceutical vendor. The system captures information including package receipt and return, patient-specific doses, inventories of doses received and administered, elution of the 99Mo–99mTc generator, quality control, and records of radiopharmaceutical kit preparation. A computerized radiopharmaceutical management system archives the procurement and use information needed for periodic review by pharmacy and helps ensure that all health physics tasks are done on time to meet regulatory compliance from state agencies, accreditation agencies, and the NRC.
Radiopharmaceutical Shortage
Times arise when radiopharmaceuticals may be in short supply or not available for a variety of issues. Planning and communication are key in appropriately managing short supply situations. Most health system pharmacy departments have contingency and communication plans already in place. Merging the procurement and supply monitoring functions of nuclear medicine and the pharmacy can allow use of these existing systems with radiopharmaceutical supply problems, so that anticipated and unanticipated radiopharmaceutical shortages can be quickly identified, alternatives arranged, and appropriate action taken.
At Christiana Care, drug shortages are managed in a scaling manner depending on the nature and timeline of the situation. The pharmacy director, when convinced timely resolution is not evident or that the shortage requires medical staff action, notifies the P&T chair. For radiopharmaceuticals, this review and decision are made collaboratively with the section chief of nuclear medicine. Where appropriate, alternative options are identified and discussed proactively. Affected staffs involved in medication management are then notified through several venues, including memorandum, health system newsletter, notice to nursing leadership, pharmacy Intranet home page announcement, and e-mail to pharmacy and nuclear medicine staff.
Storage
Because of concern about radiation, radiopharmaceutical receipt and storage are controlled primarily by NRC and state regulations and by each facility's radiation safety policies. However, radiopharmaceuticals are also prescription medications and therefore subject to numerous other standards, regulations, and manufacturer recommendations regarding their storage, security, monitoring, and proper disposal. These regulations are embodied in the medication management standards. Therefore, all health system nuclear medicine departments must have policies and procedures in place to meet both radiation safety and medication management standards. Because pharmacy personnel possess great expertise in meeting these standards, it is not difficult for a nuclear medicine and pharmacy team to achieve compliance. Radiopharmaceutical storage policies will require annual review and approval by the P&T committee and a monthly inspection at all locations by a pharmacy designee, as is done for other unit medication inspections (7). Pharmacy oversight brings added emphasis to medication labeling, including expiration dating and warnings (19). Three areas of special concern warrant mention:
Beyond Use Dating
Patients should not receive pharmaceuticals that have expired, been damaged, or are contaminated. Procedures to identify, remove, and dispose of these medications must ensure they are not intermingled with medications ready for use. All medication supplies used in nuclear medicine need to be checked regularly by staff at the point of use; therefore, an approach ensuring this review must be designed and deployed in all locations of medication storage. At Christiana Care, we instituted a monthly review procedure to scour all radiopharmaceutical inventories for medications beyond their expirations to ensure compliance and enhance patient safety. Because radiopharmaceuticals are securely stored in the nuclear medicine hot lab, the medication management inspection is performed by a nuclear medicine technologist along with the pharmacy designee. The monthly inspection report is sent to the pharmacy director. As a practical matter, since most radiopharmaceuticals have short half-lives and expire in hours, nuclear medicine professionals have a high awareness of this issue. Even though the monthly inspection almost never shows any items of noncompliance, it is still required to keep nuclear medicine consistent with other areas in the health system under pharmacy supervision. On the other hand, since some medications are still radioactive even though expired, they may require decay-in-storage handling in the nuclear medicine department before disposal. The monthly inspection verifies that any expired radiopharmaceuticals are effectively separated from doses that might be administered to a patient.
“Look-Alike, Sound-Alike” Storage Concerns
Imaging agents that are similar to each other in labeling but have different doses may lead to selection errors because they look like another product and may even have the same name. Possible look-alike, sound-alike radiopharmaceuticals include 123I metaiodobenzylguanidine vs. 131I metaiodobenzylguanidine vs. 99mTc-methoxyisobutylisonitrile (sestamibi), 99mTc-macroaggregated albumin vs. 99mTc-mercaptoacetyltriglycine, 123I-sodium iodide vs. 131I-sodium iodide vs. potassium iodide, and 123I/131I-sodium iodide vs. 18F-sodium fluoride. Our team instituted an annual review process to identify those radiopharmaceuticals posing the greatest risk of look-alike, sound-alike errors and arranged for those products to be physically separated in the hot lab to avoid mistakes. The team found that the agent of greatest concern was 99mTc-sestamibi doses for rest and stress myocardial perfusion studies, which are received as unit doses from an outside radiopharmacy. On receipt of these doses the nuclear medicine technologist first examines the incoming package for damage and surveys the package for radioactive contamination. The individual doses are categorized by specific product type and dose amount and labeled appropriately. The stress and resting sestamibi doses are then physically separated into marked locations in the hot lab to reduce the chance of error.
Emergency Medication Storage
Storage of emergency medications in nuclear medicine in emergency drug kits and code carts is generally under a health system–wide system authorized by the medical staff through the P&T committee and managed jointly by pharmacy and materials management. Standards require these medications to be stored securely yet remain readily accessible. Handling and security procedures need to be developed in accordance with law and regulation under the direction of the pharmacy director and subject to annual review by the P&T committee (6,7). At our health system, the contents of emergency drug kits are determined using evidence-based guidelines researched by the pharmacy director and approved by the P&T committee of the medical staff. Pharmacy departmental procedure for emergency drug kits is followed for replacement of used or expiring medications and is tracked through the monthly unit inspection process.
Ordering and Transcribing
In a typical nuclear medicine department, most radiopharmaceutical administrations are by protocol rather than by specific prescriber order. Medication management standards allow medication administration under protocol, provided any such protocol ensures appropriate, safe use and is approved by pharmacy and the appropriate medical staff committee such as P&T. Ideally, from the medication management standpoint the protocols should be developed initially in collaboration with the pharmacy. In mature nuclear medicine departments where established protocols are already in practice, review and amendment as needed with the pharmacy director or designee is necessary and can be beneficial. The protocols must be periodically reviewed and amended when new evidence affects protocol safety or efficacy. At Christiana Care, nuclear medicine protocols are reviewed and approved annually by the medical director and department manager of nuclear medicine, a pharmacist, and the P&T committee.
In addition to reviewing and amending all the existing nuclear medicine study protocols, our nuclear medicine and pharmacy team established a medication appropriateness review process to be performed before administering any radiopharmaceutical under protocol for a particular study. The team developed an umbrella policy describing what information must be available and taken into consideration when a radiopharmaceutical study is requested. This information includes age, sex, diagnoses, allergies, sensitivities, current medications, and other information when needed such as height, weight, pregnancy/lactation status, and pertinent lab results. This policy ensures that the nuclear medicine technologist has the information necessary to allow an appropriateness-of-use review, drug interaction and allergy screening, and other steps for each individual case. Incorporating this level of review into nuclear medicine procedures has great potential to improve patient safety (20). Patient history questionnaires, completed for each study, were revised and expanded to capture all required data. For health system inpatients, our technologists obtain this information from patient interviews or from the health system chart. In preparation for outpatient procedures, patients are now asked to bring a copy of their current medications and allergies to their appointments and a technologist will review this information during the patient interview. The technologists also require all female patients of child-bearing age (or legal proxy, where warranted) to complete and sign a pregnancy/breastfeeding questionnaire, as required by standard nuclear medicine practice.
Radiopharmaceutical dosing poses a unique medication management challenge when nuclear medicine protocols are developed. Under standard medication management practice, when a medication is used under a protocol the exact dose must be specified. This is impractical with radiopharmaceuticals, which are dosed on the basis of administered activity, which is a moving target for each dose. To provide the necessary level of specificity, our nuclear medicine and pharmacy team incorporated acceptable dose ranges into each protocol. These dose ranges are approved by the P&T committee as part of the protocol. Occasionally, there may be a technical or clinical reason to use a dose that falls slightly outside the specified range. To accommodate this rare situation, we developed a policy that requires prior approval and written authorization from the nuclear medicine physician as well as direct supervision of administration of all doses that measure beyond the dose range. Fortunately, because the protocol dose ranges were designed to incorporate most routine diagnostic radiopharmaceutical administrations, this is an unusual occurrence.
The potential for other deviations from standard protocols should also be considered. A process to handle order modifications is important because of occasional situations in which deviation from protocol is clinically indicated or a procedure must be modified to address particular clinical circumstances. In this type of situation, medication management standards would require that the deviation be reviewed by a pharmacist before administration except in emergent situations when delay caused by the review might harm the patient. To enhance patient safety in off-protocol situations, our team established a policy requiring that any radiopharmaceutical administration outside standard protocol be specifically approved and personally supervised by a nuclear medicine physician. This additional safeguard ensures accountability, provides additional on-site support for nuclear medicine personnel, and helps to ensure patient safety.
Preparing and Dispensing
Although radiopharmaceutical doses are prepared outside the pharmacy, medication management standards require that preparation protocols incorporate pharmacy expertise and input. This allows radiopharmaceutical preparation instructions within protocols and on hot lab instruction sheets to be developed consistent with good practice, quality, and accreditation standards. A process for review and acceptance of exceptions or revisions to preparation protocols should be built into the process (6,7). The team implemented a policy that exceptions or revisions from protocol require prior P&T committee or director of pharmacy approval supported by evidence-based justification before use. At Christiana Care, some radiopharmaceuticals are received as unit doses from an outside pharmacy and are not prepared on site. Only board-certified and state-licensed CNMTs approved by the section may prepare radiopharmaceuticals; this preparation is performed under indirect supervision of the nuclear medicine manager. Nuclear medicine technologist students may also be permitted to prepare radiopharmaceuticals under the direct supervision of a certified technologist. When nuclear medicine technologist students are approved for preparation or administration, the CNMT trainer is required to be present and actively oversee the entire process.
The team also implemented a policy that the hot lab, where radiopharmaceuticals are prepared, must meet standards established by the United States Pharmacopeia (6). Through their oversight function, health system pharmacy directors are ultimately responsible for ensuring that this standard is met (6,7). Compliance is verified through periodic internal and accrediting organization assessments and inspections. In accordance with medication management standards, staff competency in aseptic technique and dose preparation is assessed through periodic physical demonstration of sterile product preparation by all CNMTs. This is another area in which established pharmacy procedures and guidelines can be easily adapted to ensure the competency of nuclear medicine personnel. The pharmacy director ensures monthly inspections of the hot lab to assess environment, storage, security, and compliance with health system policy and accreditation standards. Cleaning, air quality testing, and microbial swabbing reports are routinely provided to the pharmacy director for review and, as appropriate, action.
Administering and Monitoring
Once the nuclear medicine physician, the authorized user under the institution's NRC license, approves a particular study or procedure for a patient, a certified technologist may then administer radiopharmaceuticals pursuant to the departmental P&T-approved protocol. Our interdepartmental team expanded existing nuclear medicine dose administration procedures to provide additional safeguards required by medication management guidelines. Under the protocol, the technologist must screen for potential drug interactions and contraindications specific to the agent to be used, screen for dosage adjustments such as those dictated by renal or liver function, and provide the patient with education about the medication to be administered. This patient education includes the radiopharmaceutical name, risks and benefits, anticipated side effects, after-procedure instructions, and responses to patient questions. (Under the current scope of practice rules at our institution, a registered nurse is required to administer any nonradioactive agents ordered by protocol or individual prescriber order; the nurse performs the screening and patient education functions for those medications.) The nuclear medicine technologist monitors the patient after radiopharmaceutical administration as appropriate for the agent selected. Medications are available in case of reaction or extravasation. If there is any complication or reaction, the nuclear medicine physician is notified. After the patient is treated if indicated, the technologist, nurse, or physician implements the reporting system for this type of occurrence in the health system's online reporting system used for all medications. This allows investigation of individual cases as well as longitudinal reviews to identify trends or opportunities for system improvement. The reporting process is similar in the event an error in radiopharmaceutical administration occurs.
Documentation of the order for the study, patient history, details of radiopharmaceutical dose administration, patient counseling, and other details needs to be permanently archived for each study. We maintain this documentation in our health system's PACS, Philips iSite (21), together with the images from the study. All patient paperwork and images are transferred to the PACS system when the patient study is completed. The paperwork includes the test request from the referring physician, patient consents, completed nuclear medicine patient questionnaire, and any additional pertinent information used to create the protocol for the study or to complete or interpret the study. The patient questionnaire contains information such as patient medications, allergies, past medical history, and blanks for documentation of patient education as well as the name, amount, dose, and administration route of all radioactive and nonradioactive medications used for the study. This information is kept indefinitely and is available for review by nuclear medicine or pharmacy staff as needed.
Periodic Review and Event Reporting
Two additional tasks in setting up a medication management system for nuclear medicine should be noted. First, in addition to getting nuclear medicine protocols approved by the appropriate medical staff committee and all agents placed on formulary, review and inspection systems for various aspects of the program must be established. Best medication management practices require periodic (minimally annual) review of all important component processes of the system. This provides performance monitoring and allows the system to stay up to date as conditions change or new information becomes available. System processes requiring periodic review include radiopharmaceutical formulary selection; radiopharmaceutical storage policies; look-alike, sound-alike medications and radiopharmaceuticals; handling and security procedures; and radiopharmaceutical administration protocols. Periodic review is fundamental to good medication management practice since this ensures accountability, identifies trends, and keeps the process up to date. Fortunately, health system pharmacists are familiar with the periodic reviews required and often have existing systems that can easily be used to track and document the necessary processes in nuclear medicine.
Also required is a system to identify and follow up on any errors or adverse events that do occur. The comprehensive medication management policy developed for nuclear medicine by our team includes a Medication Administration Error section, which provides a procedure to capture both pharmaceutical and radiopharmaceutical administration errors. This section integrates a hospitalwide Safety First Learning Report, which provides an established pathway for event reporting. The system provides a mechanism for prompt reporting of events, a database for trending, and coordination of intervention and follow-up. Radiopharmaceutical administration errors also require the notification of the chief technologist, nuclear medicine manager, nuclear medicine physician, and radiation safety officer. Any radiopharmaceutical administration error is also discussed at the next quarterly radiation safety committee meeting, and appropriate corrective actions are implemented in a timely manner.
RESULTS
Compliance since implementation of the new procedures has been high. Restructuring the medication use procedures was the key in this team's experience leading to compliance with quality standards. Requiring special focus was the need to achieve this compliance while not disrupting workflows. We found that we began the process with limited knowledge by nuclear medicine personnel about medication management best practices and limited knowledge by pharmacy about nuclear medicine procedures and issues unique to radiopharmaceuticals. The team's efforts were also challenging in the face of limited literature on some commonly accepted off-label uses. To address this, all members of the team committed to sharing their expertise and printed resources. Collaborative exchanges occurred over the course of many meetings simply to understand process, standards, workflows, and best practices. Two-way education between practitioners was collegial throughout the initiative and was instrumental in overcoming the barriers the team faced. After extensive reading and discussions, all team members shared a common platform of knowledge and mutual understanding of objectives and priorities. A common aim to change systems to achieve 100% compliance helped to align all involved to a singular goal.
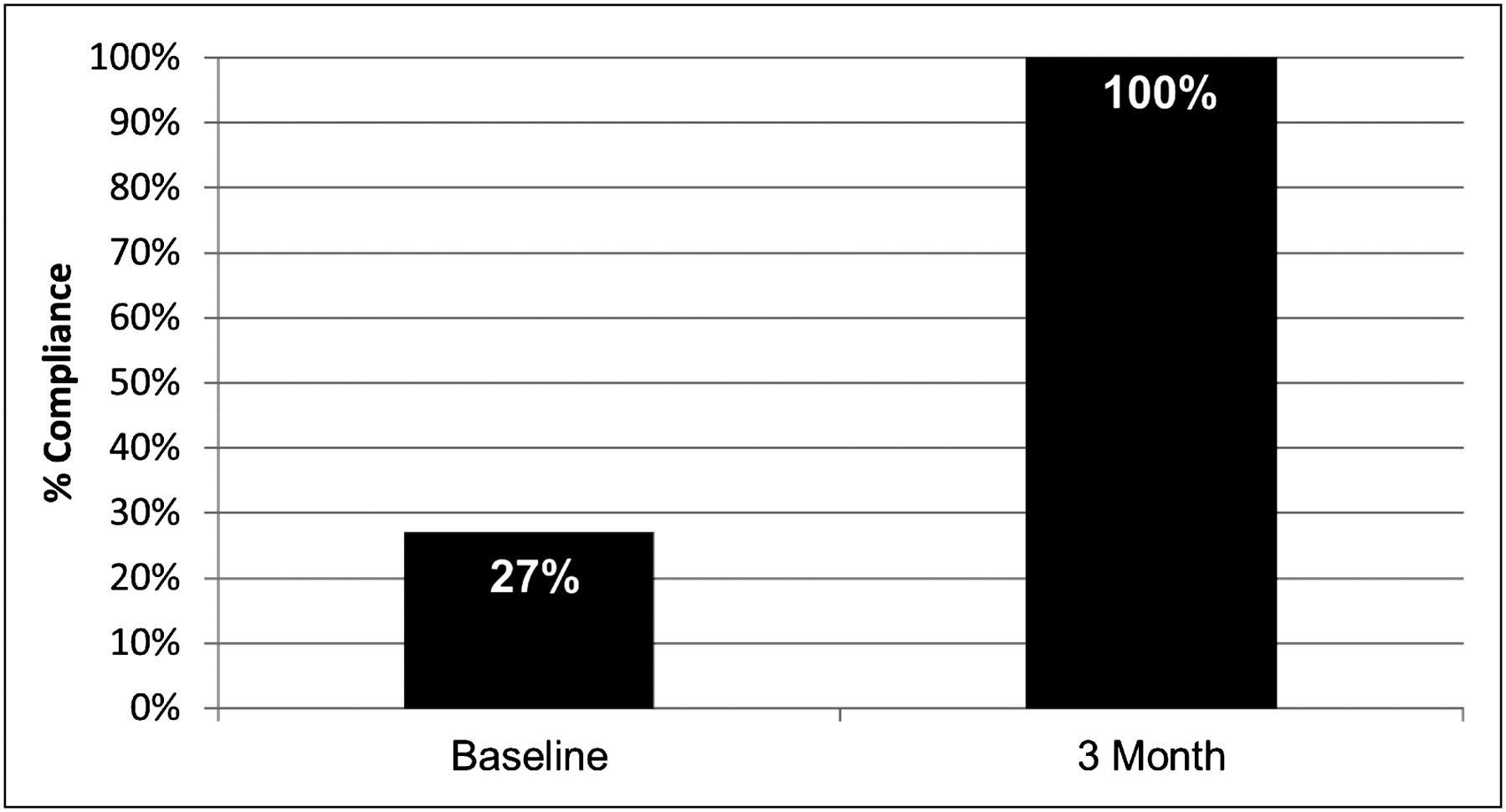
As already noted, our initial gap analysis showed compliance with only 27% of the applicable standards. After 3 mo of intensive effort by the nuclear medicine and pharmacy team, a repeated self-assessment suggested we had achieved 100% compliance (Fig. 2). A subsequent inspection of our institution by TJC confirmed no deficiencies.
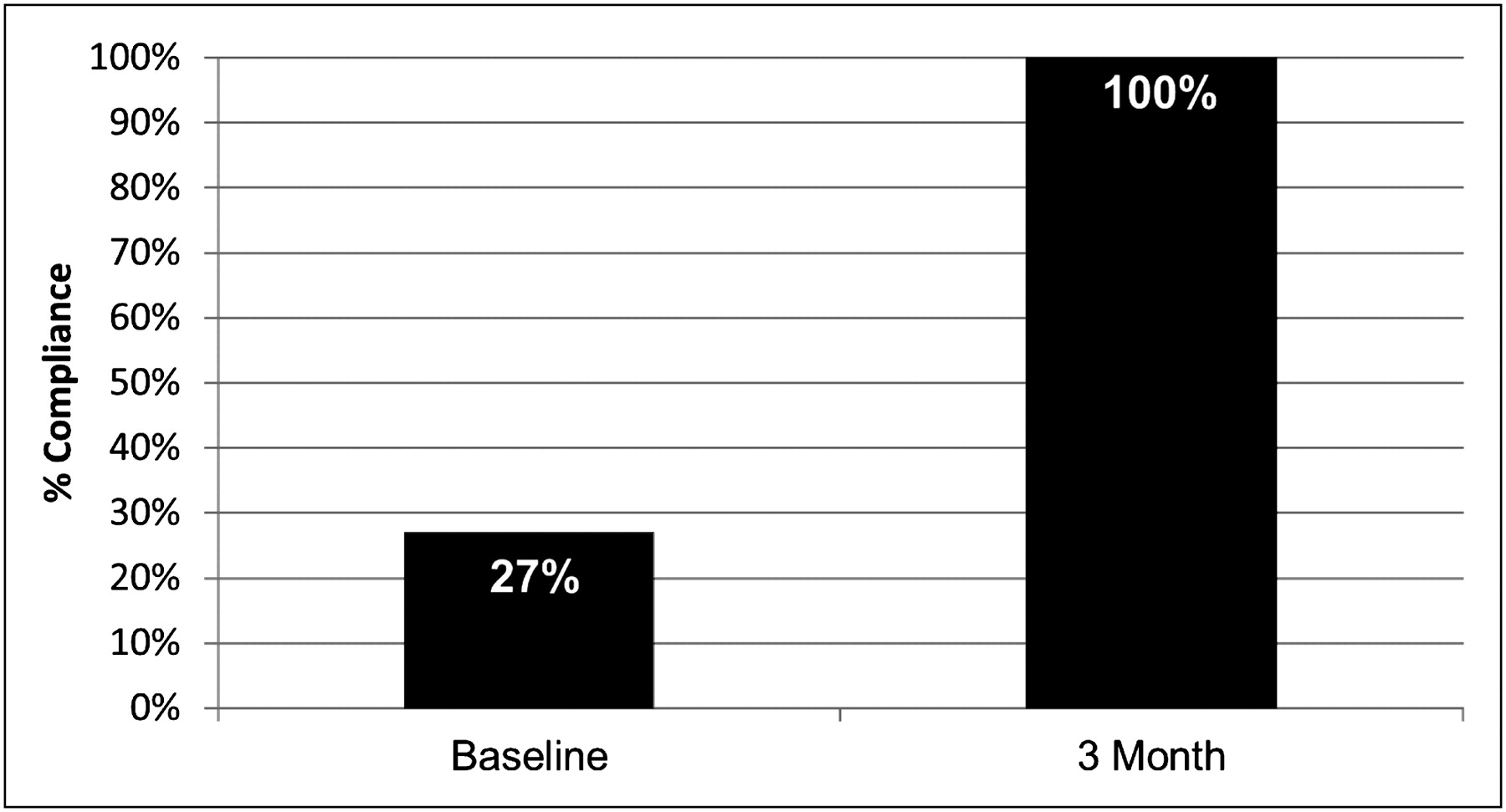
Compliance with TJC medication management standards increased to 100% within 3 mo as a result of intensive intervention by a collaborative nuclear medicine and pharmacy team.
After 1 y of experience with the new policies and procedures, the medication use process remains in compliance with standards and we have not detected that work flow efficiencies in nuclear medicine have been adversely affected by the changes. Technologists’ clock hours and overtime hours have remained the same; likewise, case throughput remains the same as preimplementation rates. An additional benefit of these new medication management policies and procedures was their scalability. The team discovered, with the establishment of new imaging sites, that the policies were easily incorporated or adapted, when appropriate, depending on the circumstances of the facility being established.
Nuclear medicine personnel state they derive added satisfaction from knowing that procedural protocols are strongly designed to protect patient safety. Nuclear medicine staff readily acknowledge the benefits from the resources provided by pharmacy personnel and monitoring systems. Pharmacy expertise applied early in the development of procedural protocols has improved clarity of medication selection, dosing, preparation, and monitoring. Physicians and technologists involved in protocol development have expressed satisfaction with this added input and their sense that instructions are clear and standardized. Since implementation of the program, despite more rigorous standards and heightened vigilance through inspections, reports, and monitoring, no adverse trends have been detected.
CONCLUSION
There is no question that health system nuclear medicine departments are now required to comply with national standards for medication management. This is a daunting prospect for many departments that have long operated independently. Our experience shows that a collaborative team involving nuclear medicine and pharmacy can meld resources from both specialties to achieve compliance and make improvements in safety while taking into account the particular circumstances of the departments involved. Our collaborative team initiative has been presented at a national health systems pharmacist meeting in 2010 and was awarded the Gold Award for Clinical Excellence in our health care system's annual Focus on Excellence performance improvement program. This model may easily be used by other facilities to achieve compliance with accreditation standards and the ultimate goal of enhanced patient care and safety.
Acknowledgments
We recognize the other members of the nuclear medicine and pharmacy team at Christiana Care: Cynthia Knotts, CNMT, Anthony Gialloreto, CNMT, Theresa Riggle, CNMT, and Patricia Robinson. No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Jan. 25, 2012.
↵* NOTE: FOR CE CREDIT, YOU CAN ACCESS THIS ACTIVITY THROUGH THE SNM WEB SITE (http://www.snm.org/ce_online) THROUGH MARCH 2014.
REFERENCES
- Received for publication June 7, 2011.
- Accepted for publication November 8, 2011.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.