


Abstract
Diabetic foot infection is the most common etiology of nontraumatic amputation of the lower extremities, and early diagnosis is of great importance in its management. The aim of this prospective study was to evaluate the strength of 99mTc-IgG scintigraphy in diagnosis of osteomyelitis of the diabetic foot and to compare 99mTc-IgG scintigraphy with 99mTc-methylene diphosphonate (MDP) scintigraphy. Methods: A prospective university hospital–based study was performed over 24 mo. Eighteen patients with type II diabetes and foot ulcers (15 men and 3 women; age range, 45–80 y) were referred for imaging because of clinically suspected osteomyelitis. Early (5-h) and late (24-h) 99mTc-IgG scanning and 3-phase skeletal scintigraphy were completed for all patients at a 3- to 4-d interval. Regions of interest over the involved bony sites and the contralateral normal sites were drawn, and the abnormal-to-normal ratios were acquired for both 99mTc-IgG and 99mTc-MDP studies. Results: From a total of 23 lesions, we observed 10 sites of osteomyelitis, 10 sites of cellulitis, and 3 sites of aseptic inflammation confirmed by MRI, clinical presentation, histopathologic examination, and follow-up evaluation as a gold standard. Both 99mTc-IgG and 99mTc-MDP scanning showed excellent sensitivity for diagnosis of osteomyelitis, but the specificity was significantly lower (69.2% and 53.8%, respectively). Sensitivity, specificity, and accuracy in the diagnosis of osteomyelitis were, respectively, 100%, 53.8%, 73.9% for 99mTc-MDP scanning; 100%, 69.2%, 82.6% for 5-h 99mTc-IgG scanning; and 60%, 76.9%, 69.5% for 24-h 99mTc-IgG scanning. There was no significant difference between the semiquantitative indices of 5-h and 24-h 99mTc-IgG scanning for inflammation, cellulitis, and osteomyelitis. Conclusion: Although both 99mTc-IgG and 99mTc-MDP scintigraphy have high sensitivity for the diagnosis of osteomyelitis, the specificity of these studies is poor. For 99mTc-IgG scintigraphy, 5-h images appear to be adequate, and there is little benefit to performing additional imaging at 24 h.
Peripheral neuropathy and metabolic and vascular disorders are important contributing factors leading to infection of obscured wounds in diabetic patients (1,2). When there is evidence of osteomyelitis, invasive procedures are needed to avoid amputation (3). Radiographic evaluation is not sensitive for the development of osteomyelitis, whereas labeled leukocyte imaging followed by bone marrow scintigraphy, although both sensitive and specific, is labor-intensive and limited by the risks associated with handling blood products (4). 111In-IgG and 99mTc-methylene diphosphonate (MDP) scintigraphy can be helpful for the diagnosis of inflammation and infection (5–11).
The aim of this prospective study was to assess the role of 99mTc-IgG scintigraphy in the diagnosis of osteomyelitis in the diabetic foot and to compare 99mTc-IgG scintigraphy with 99mTc-MDP scintigraphy. In addition to qualitatively assessing the 99mTc-MDP and 99mTc-IgG studies, we have attempted to evaluate the clinical usefulness of quantitative uptake on 99mTc-MDP and 99mTc-IgG scanning in detecting osteomyelitis in peripheral bony lesions.
MATERIALS AND METHODS
Participants
This study was conducted on 18 patients with type II diabetes who were referred to our nuclear medicine department with a clinical suspicion of osteomyelitis. The patients were recruited from a university hospital in Tehran from 2006 to 2008. They underwent 99mTc-IgG scanning first, followed by 3-phase 99mTc-MDP skeletal scanning at a 3- to 4-d interval.
The study complied with the declaration of Helsinki and was approved by the institutional ethics committee of Shaheed Beheshti University of Medical Science, and all patients gave written informed consent.
Imaging Protocols
99mTc-IgG Scintigraphy.
In both studies, the amount of intravenously injected 99mTc was about 740 MBq (20 mCi), and images were acquired by a double-head SPECT scintillation camera (Genesys; ADAC) with a low-energy all-purpose collimator using a matrix of 128 × 128 on a 20% window at a 140-keV peak. The intensity settings of the scintillation camera were carefully monitored so that images of comparable counts and intensities were available for interpretation. Three nuclear medicine consultants unaware of other data evaluated the scintigraphic studies and reached the final impression by consensus.
For 99mTc-IgG scintigraphy, a human nonspecific polyclonal immunoglobulin for intravenous administration was used. An IgG solution with a concentration of about 10 mg/mL in 0.01 M phosphate-buffered saline, pH 7.4, was prepared. 99mTc-IgG was prepared by adding 740 MBq (20 mCi) of 99mTc to an IgG kit provided by the Nuclear Energy Institute of Iran and incubating for 20 min at room temperature. 99mTc-IgG was administered intravenously, and early (5-h) and delayed (24-h) imaging was performed minimally in 2 views, for at least 400,000 counts and 50,000 counts, respectively. Images of the contralateral normal anatomic region were also obtained.
99mTc-MDP Scintigraphy.
Skeletal scans were obtained using 740 MBq of 99mTc-MDP. The first phase of the skeletal scan consisted of the radionuclide angiogram, comprising sequential images at 2–3 s per frame over the involved region of suspected osteomyelitis and the opposite presumed normal anatomic region. The flow phase was performed for 60 s, followed by a blood-pool image at 180 s after intravenous injection of the radiopharmaceutical. Delayed images were obtained 3 h after 99mTc-MDP injection using the same projections for at least 500,000 counts.
Visual Interpretation
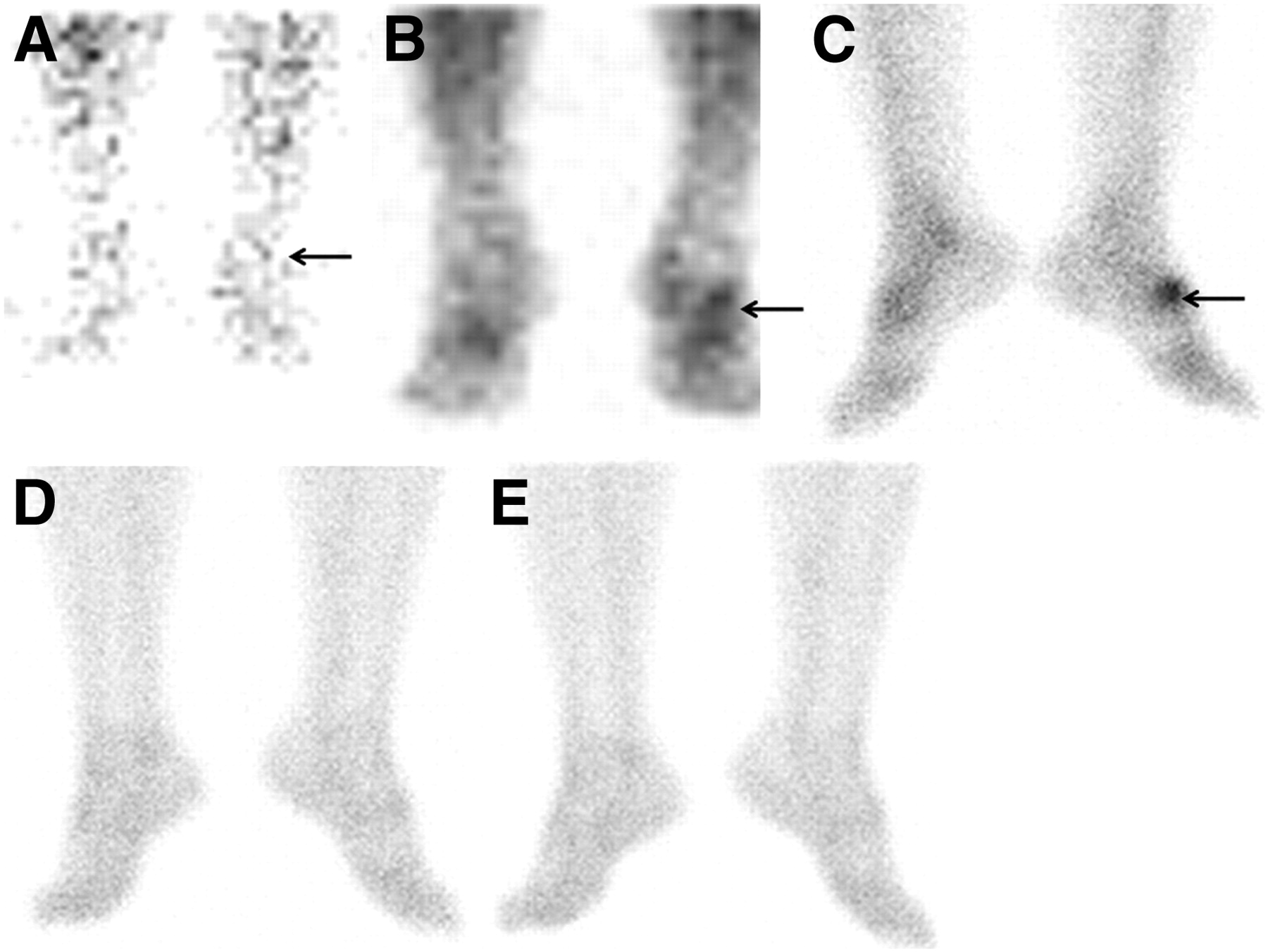
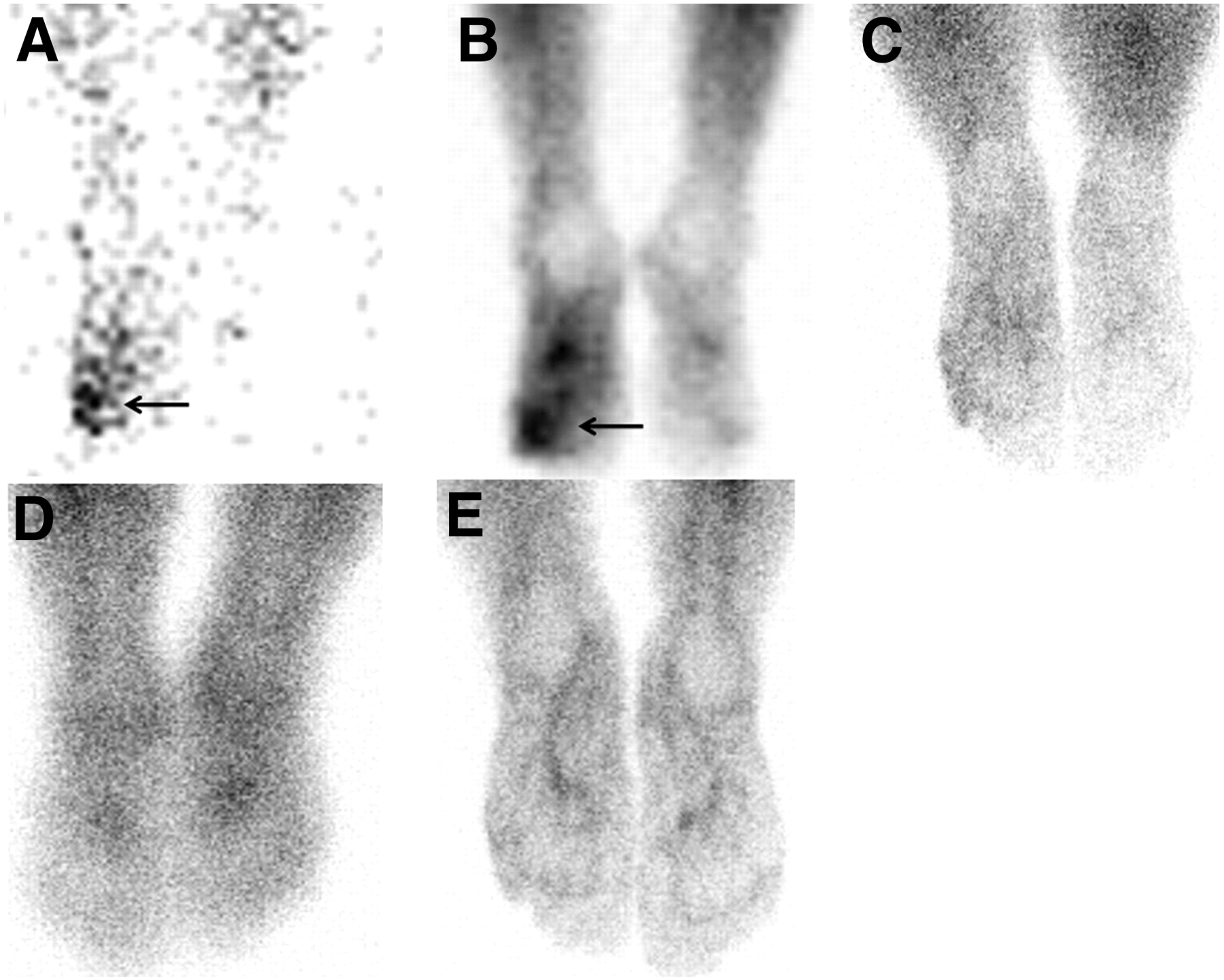
The determination of osteomyelitis was based on significant uptake of radiopharmaceutical in all 3 phases of 99mTc-MDP scanning or an intense accumulation on 99mTc-IgG scanning (Fig. 1). Accumulation of radionuclide in only the first 2 phases of skeletal scanning or a mild to moderate uptake on 99mTc-IgG scanning was characterized as cellulitis (Fig. 2). If there was remarkable radionuclide uptake on 99mTc-MDP scanning without significant uptake on 99mTc-IgG scanning, aseptic inflammation was considered present (Fig. 3). Radionuclide uptake was characterized as absent (−), faint (±), moderate (+), or marked (++).
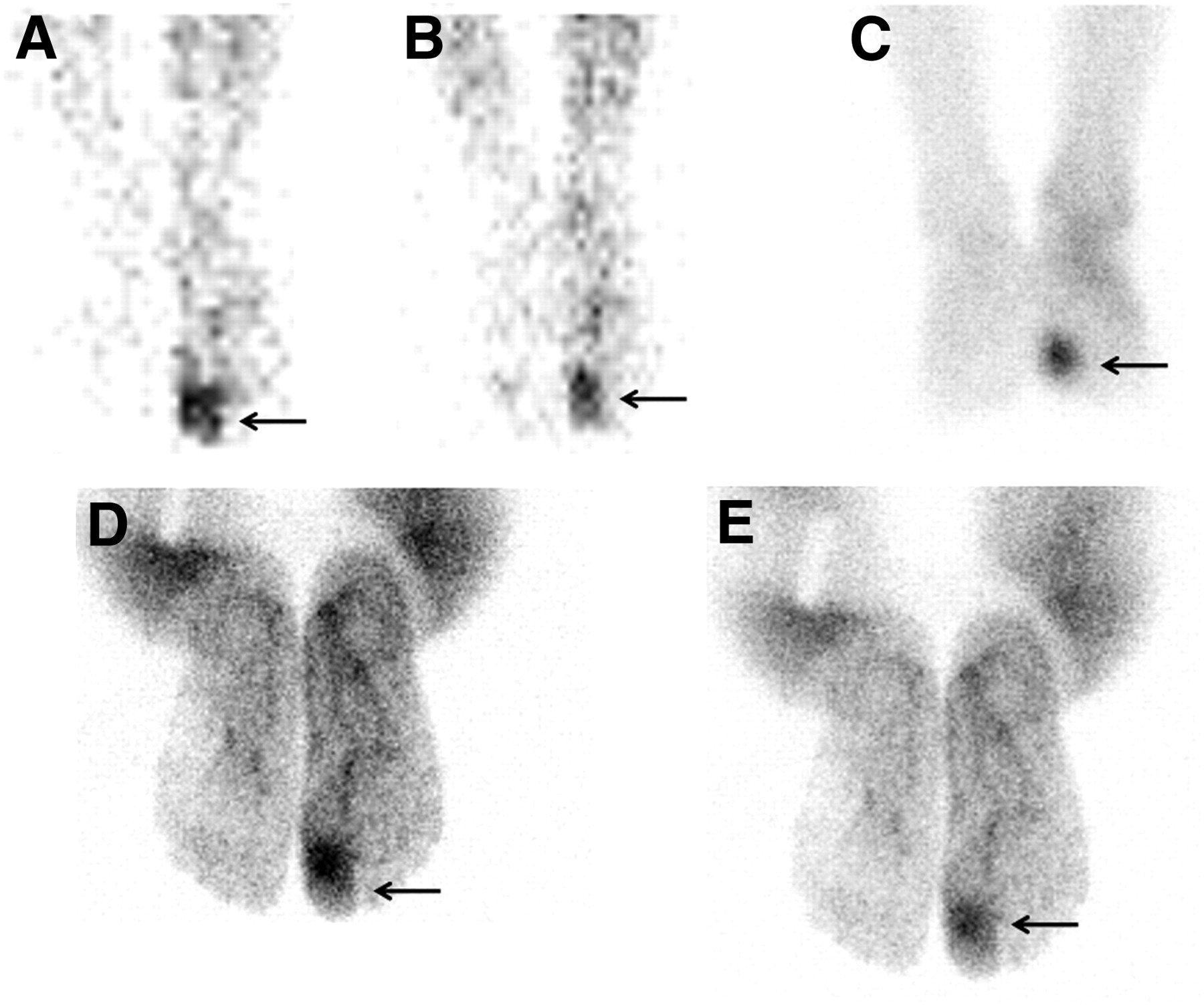
Example images of osteomyelitis (arrows). Significant uptake of 99mTc-MDP is seen in right first toe in all 3 phases of skeletal scintigraphy, accompanied by intense radiotracer uptake indicating osteomyelitis on 99mTc-IgG scan. (A) Flow phase of 99mTc-MDP skeletal scintigraphy. (B) Blood-pool phase of 99mTc-MDP bone scintigraphy. (C) Delayed phase of 99mTc-MDP skeletal scintigraphy. (D) Five-hour 99mTc-IgG scintigraphy. (E) Twenty-four-hour 99mTc-IgG scintigraphy.

Example images of cellulitis (arrows). Significant uptake of 99mTc-MDP is seen in left fifth metatarsi in flow and blood-pool phases of skeletal scintigraphy, but activity is normal in delayed phase and there is no significant uptake in same region on 99mTc-IgG scan. (A) Flow phase of 99mTc-MDP skeletal scintigraphy. (B) Blood-pool phase of 99mTc-MDP bone scintigraphy. (C) Delayed phase of 99mTc-MDP skeletal scintigraphy. (D) Five-hour 99mTc-IgG scintigraphy. (E) Twenty-four-hour 99mTc-IgG scintigraphy.
Example images of aseptic inflammation (arrows). Significant uptake of 99mTc-MDP is seen in dorsal aspect of left foot (talus bone) in all 3 phases of skeletal scintigraphy, but there is no significant uptake on 99mTc-IgG scan. (A) Flow phase of 99mTc-MDP skeletal scintigraphy. (B) Blood-pool phase of 99mTc-MDP bone scintigraphy. (C) Delayed phase of 99mTc-MDP skeletal scintigraphy. (D) Five-hour 99mTc-IgG scintigraphy. (E) Twenty-four-hour 99mTc-IgG scintigraphy.
Semiquantitative Analysis
Both 99mTc-MDP and 99mTc-IgG scans were further analyzed by drawing ellipsoid regions of interest over the suspected abnormal and contralateral normal bony sites. The entire lesion was included in the ellipsoid region, and mean counts per pixel in each region were measured. The mean uptake count ratios between abnormal and contralateral normal sites were also obtained; the ratios were calculated and considered to be indices, and the difference in indices for osteomyelitis, cellulitis, and inflammation in the scans were tested for significance.
The clinicians determined the final diagnosis by consensus, according to the MRI results, clinical presentation, wound culture results, histopathologic results, and follow-up results.
Statistical Analysis
Sensitivity, specificity, negative and positive predictive values, and accuracy were determined for each scan, and the potential differences in osteomyelitis, cellulitis, and aseptic inflammation on 99mTc-MDP scanning and on early and late 99mTc-IgG scanning were analyzed using ANOVA. A P value of less than 0.05 was considered significant. Statistical analysis was performed using an IBM computer and PASW software, version 18.0 (SPSS, Inc.).
RESULTS
The study included 3 women and 15 men (age range, 45–80 y). From a total of 23 lesions, we observed 10 sites of osteomyelitis, 10 sites of cellulitis, and 3 sites of aseptic inflammation, of which 2 were caused by Charcot joint (Table 1).
Scintigraphy Results
Both 99mTc-IgG and 99mTc-MDP scans showed excellent sensitivity for the diagnosis of osteomyelitis, but specificity was significantly compromised (69.2% and 53.8%, respectively). 99mTc-IgG scanning could differentiate osteomyelitis from cellulitis but not Charcot joint from osteomyelitis (Table 2). Sensitivity, specificity, and accuracy in the diagnosis of osteomyelitis were, respectively, 100%, 53.8%, and 73.9% for 99mTc-MDP scanning; 100%, 69.2%, and 82.6% for 5-h 99mTc-IgG scanning; and 60%, 76.9%, and 69.5% for 24-h 99mTc-IgG scanning.
Accuracy of Various Scintigraphy Procedures in Osteomyelitis Diagnosis
The osteomyelitis, cellulitis, and inflammation indices are reported in Table 3. We did not find any significant difference among the indices on 99mTc-MDP scintigraphy or on 5 h-and 24-h 99mTc-IgG scintigraphy (P > 0.5).
Osteomyelitis Indices in Various Scintigraphy Procedures
DISCUSSION
We observed that both 99mTc-MDP and 99mTc-IgG scanning can sensitively detect osteomyelitis; however, they lack the appreciated specificity. Datz et al., investigating 53 patients with assumed infection, reported that the sensitivity and specificity of 111In-IgG scanning was 97.9% and 94%, respectively. They found that this method can detect chronic and acute osteomyelitis with equal sensitivity, and simultaneous administration of antibiotics, steroids, and antiinflammatory agents or concurrent diabetes and renal dysfunction had no influence on scan sensitivity (6).
MRI can efficiently discriminate soft-tissue infection from bone involvement and can effectively detect the development of infection in anterior parts of the bone; however, efficacy is dramatically compromised at the midfoot and hindfoot (12–15). Despite high sensitivity, the application of MRI for the recognition of osteomyelitis in the diabetic foot is compromised by lower specificity regarding Charcot neuropathic osteoarthropathy. In addition, if there is an inflammatory hyperemia, the diagnostic accuracy is further decreased to 40%–50% (8).
Devillers et al., studying 56 diabetic foot ulcers in 40 patients, reported that the accuracy of radiography, 99mTc-MDP scintigraphy, and 99mTc-exametazime–conjugated leukocyte scintigraphy was 69.6%, 62.5%, and 92.9%, respectively. They concluded that leukocyte-labeling scintigraphy can be considered an outstanding technique for the identification of osteomyelitis in the diabetic foot and can be useful in follow-up evaluation because of an ability to predict osteomyelitis remission despite the lack of complete clinical regression of the diabetic ulcers (1). Although both sensitive and specific, leukocyte labeling scintigraphy followed by bone marrow scanning is also limited by inaccessibility, labor intensity, and the risk of infectious blood handling (4). Because of high sensitivity and the frequency of positive outcomes, the usefulness of labeled leukocyte imaging as a screening test is uncertain; supplementation of skeletal imaging by labeled leukocyte imaging has resulted in only marginal improvement of the test (14). Skeletal scanning can sensitively be applied for the determination of osteomyelitis but fails to differentiate diabetic osteomyelitis from other osteoarthropathic conditions because of higher bone turnover in both (16). There have been extensive reports about the usefulness of 99mTc-IgG scintigraphy in detecting a variety of infections, including those of the chest, abdomen, hip, and bone; however, as we also observed, this procedure might not be able to discriminate infection from aseptic inflammation (2,3,17,18). 111In-IgG scintigraphy differentiated infectious from sterile inflammatory processes in 25 adult patients with complicated osteomyelitis or septic arthritis with a sensitivity of 90% and specificity of 95% (19). Oyen et al. have reported that a recent bone trauma or fracture might be misleading in IgG scan interpretation (20–22). Unal et al., examining 20 cases of diabetic foot, reported a 100% versus 94% sensitivity and a 59% versus 100% specificity for 99mTc-IgG and 99mTc-white blood cell labeling, respectively (18). Correspondingly, we observed 4 cases of false-positive osteomyelitis, of which 2 were caused by cellulitis and 2 by aseptic infection, reflecting a lack of specificity of 99mTc-IgG scintigraphy. In a comprehensive study comparing 3 scanning techniques (triphasic skeletal scintigraphy, 99mTc-white blood cell scintigraphy, and 99mTc-IgG scintigraphy) in distinguishing musculoskeletal infection from noninfectious inflammation in 35 orthopedic patients, 2- to 6-h 99mTc-white blood cell scintigraphy and 20- to 24-h 99mTc-IgG scintigraphy had the greatest value (P < 0.01 and P < 0.016, respectively), with a sensitivity of 96.6% and 96.5%, respectively, and a specificity of 71% and 100%, respectively. The authors concluded that 99mTc-IgG scintigraphy might be an alternative to 99mTc-white blood cell scintigraphy because of its simplicity of preparation, similarity of accuracy, and safety, as well as its being better able to show the spread of inflammation into soft tissues (23).
We did not find any differences between the osteomyelitis, cellulitis, and aseptic inflammation indices in 5-h and 24-h 99mTc-IgG scanning. Therefore, it seems there is no need for delayed scintigraphy; one can evaluate the case with only a single scan.
Our study had some shortcomings, the most important of which were the relatively small sample size and the absence of bone biopsy as a gold standard, which may influence the results. However, we consider this problem to have been reduced by the compound use of MRI, clinical presentation, histopathologic examination, and follow-up evaluation. Further well-designed studies would seem useful.
CONCLUSION
Both 99mTc-IgG and 99mTC-MDP scanning can be applied to detect bone involvement in diabetic infection with excellent sensitivity; however, their specificity is compromised, especially in distinguishing between infection and inflammation. In addition, early 5-h images seem to be adequate in 99mTc-IgG scintigraphy, and there is no need for 24-h images.
Acknowledgments
We thank the colleagues at our institutes, especially Soodabeh Ramazani, Hamid Ahmadi, Yahya Nadiri, and Hossein Alizadeh, for technical help and data acquisition. This study was performed under the sponsorship of Shaheed Beheshti University of Medical Sciences (grant 1763). No other potential conflict of interest relevant to this article was reported.
Footnotes
Published online Jul. 27, 2011.
REFERENCES
- Received for publication November 18, 2010.
- Accepted for publication April 21, 2011.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.