


Article Figures & Data
Figures
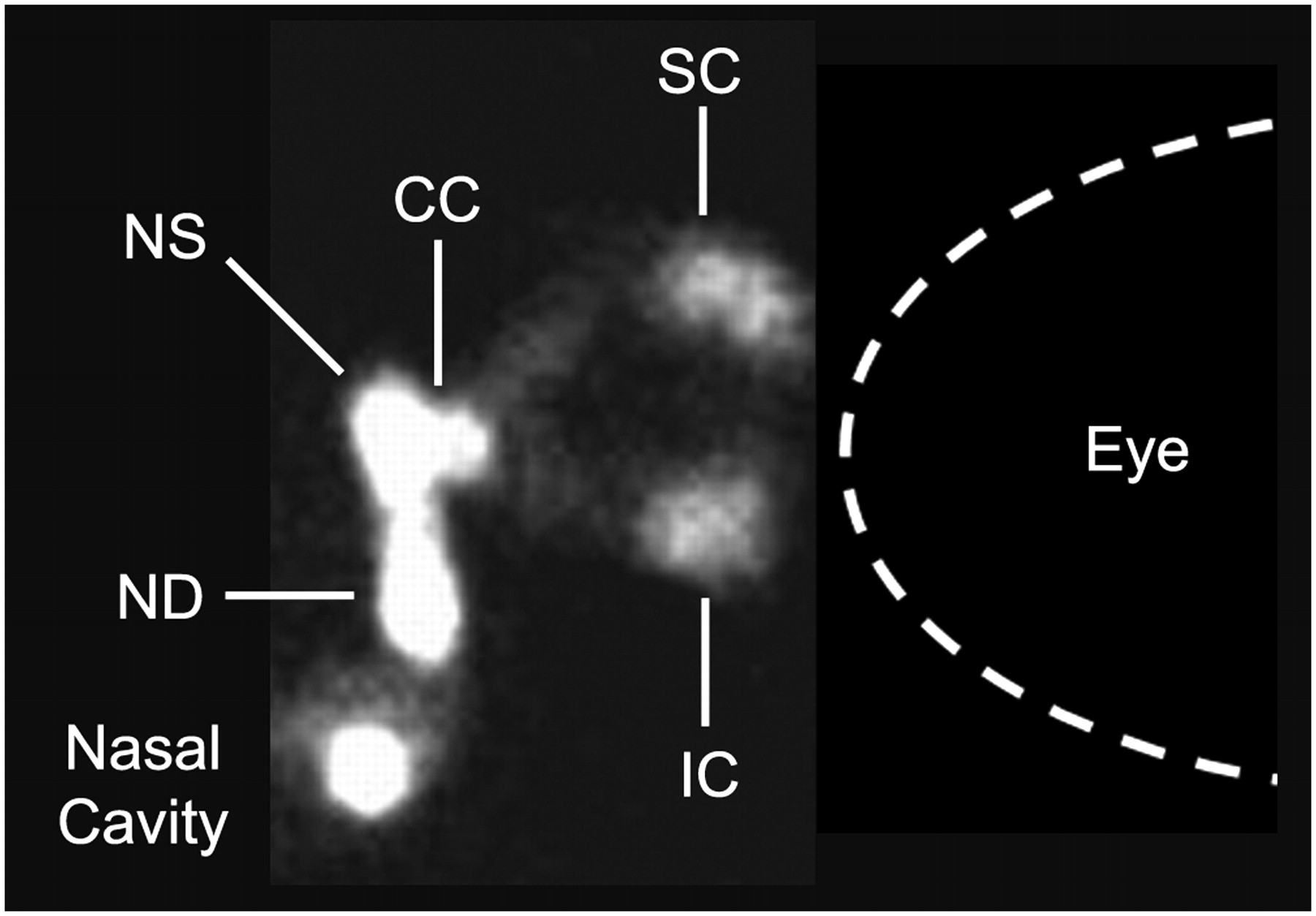
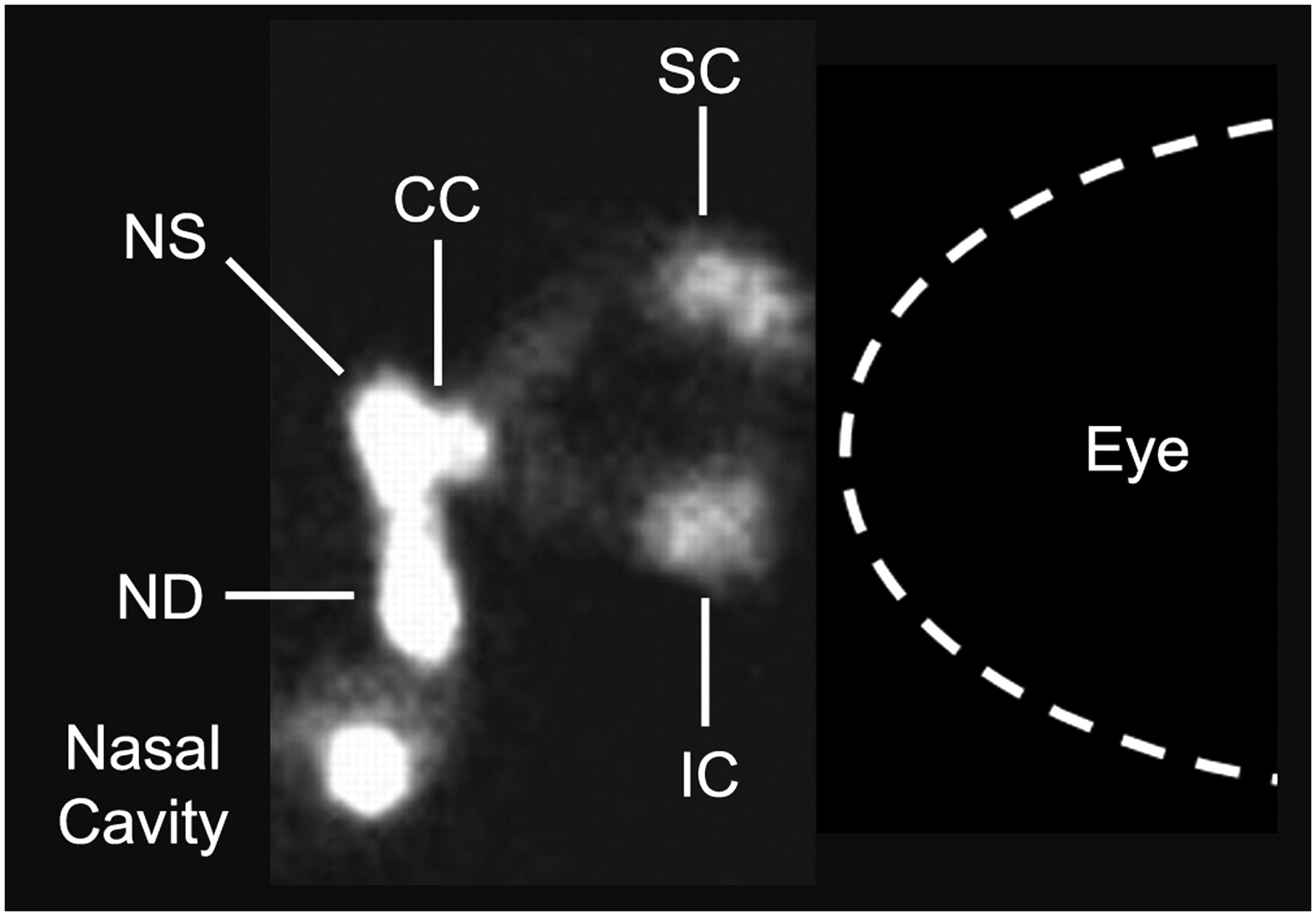
- FIGURE 1.
Nasolacrimal apparatus as seen on dacroscintigraphy. Nasolacrimal apparatus is situated medial to eye and consists of superior canaliculus (SC) and inferior canaliculus (IC), common canaliculus (CC), nasolacrimal sac (NS), and nasolacrimal duct (ND).
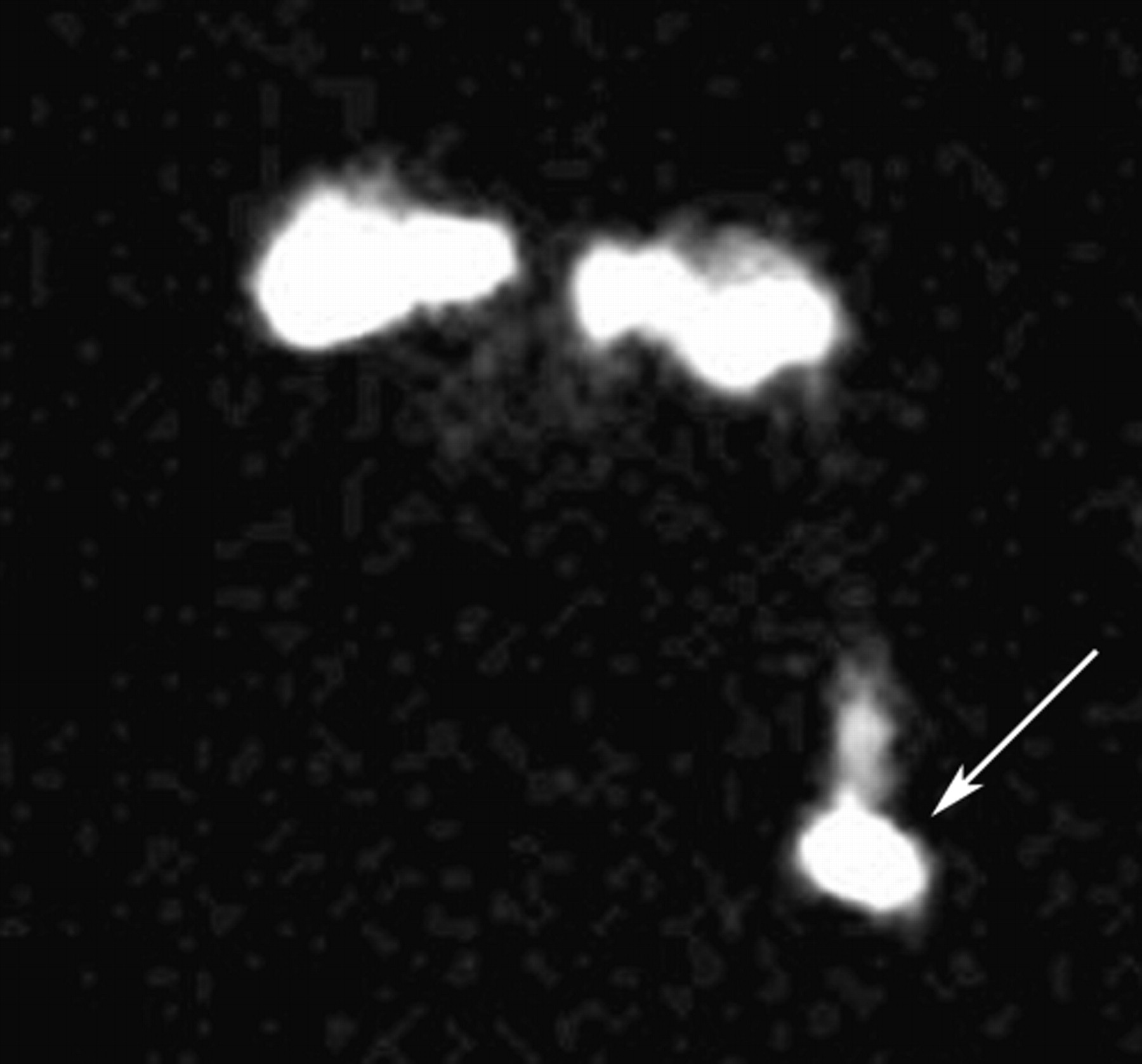
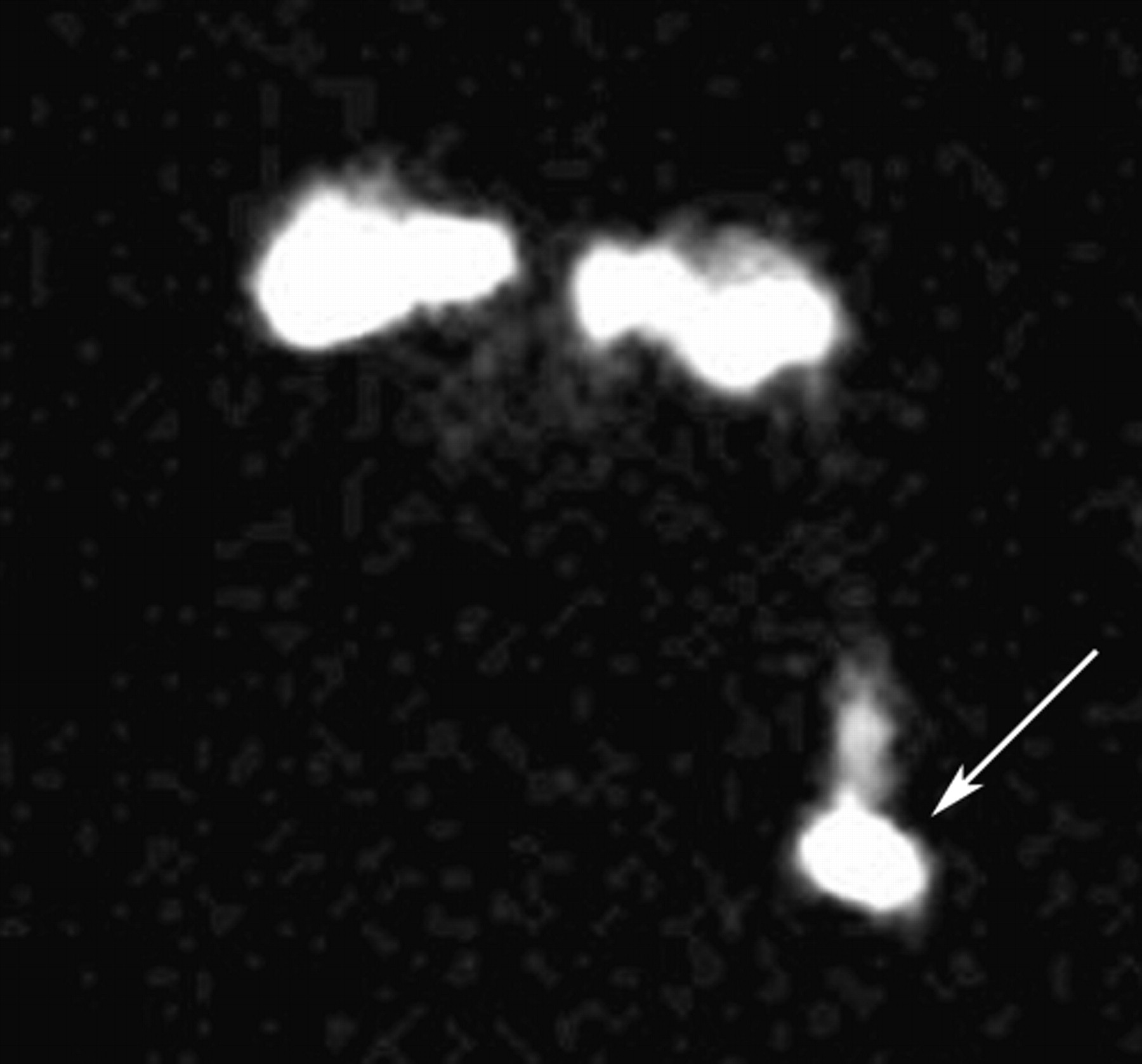
- FIGURE 2.
Tears usually deviate laterally, whereas true drainage pattern will reveal activity to deviate medially into nasal cavity. This case demonstrates patient with contamination from radioactive tears from left eye falling anteriorly down face (arrow).
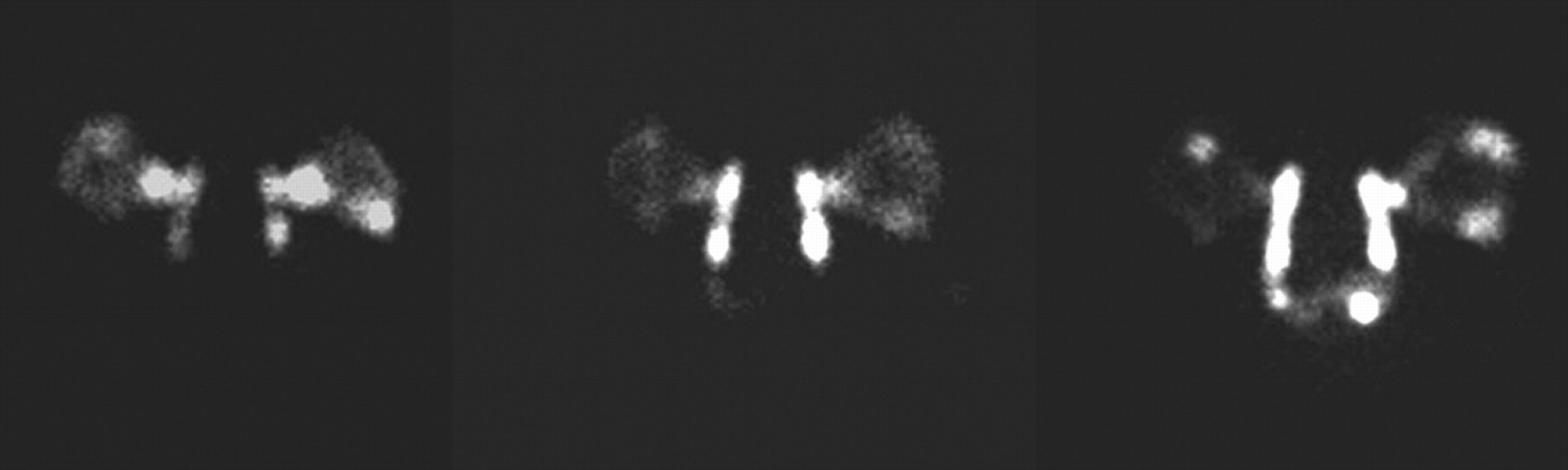
- FIGURE 3.
Normal lacrimal gland study at 3 time points demonstrating bilateral drainage from eyes into nasal cavity.
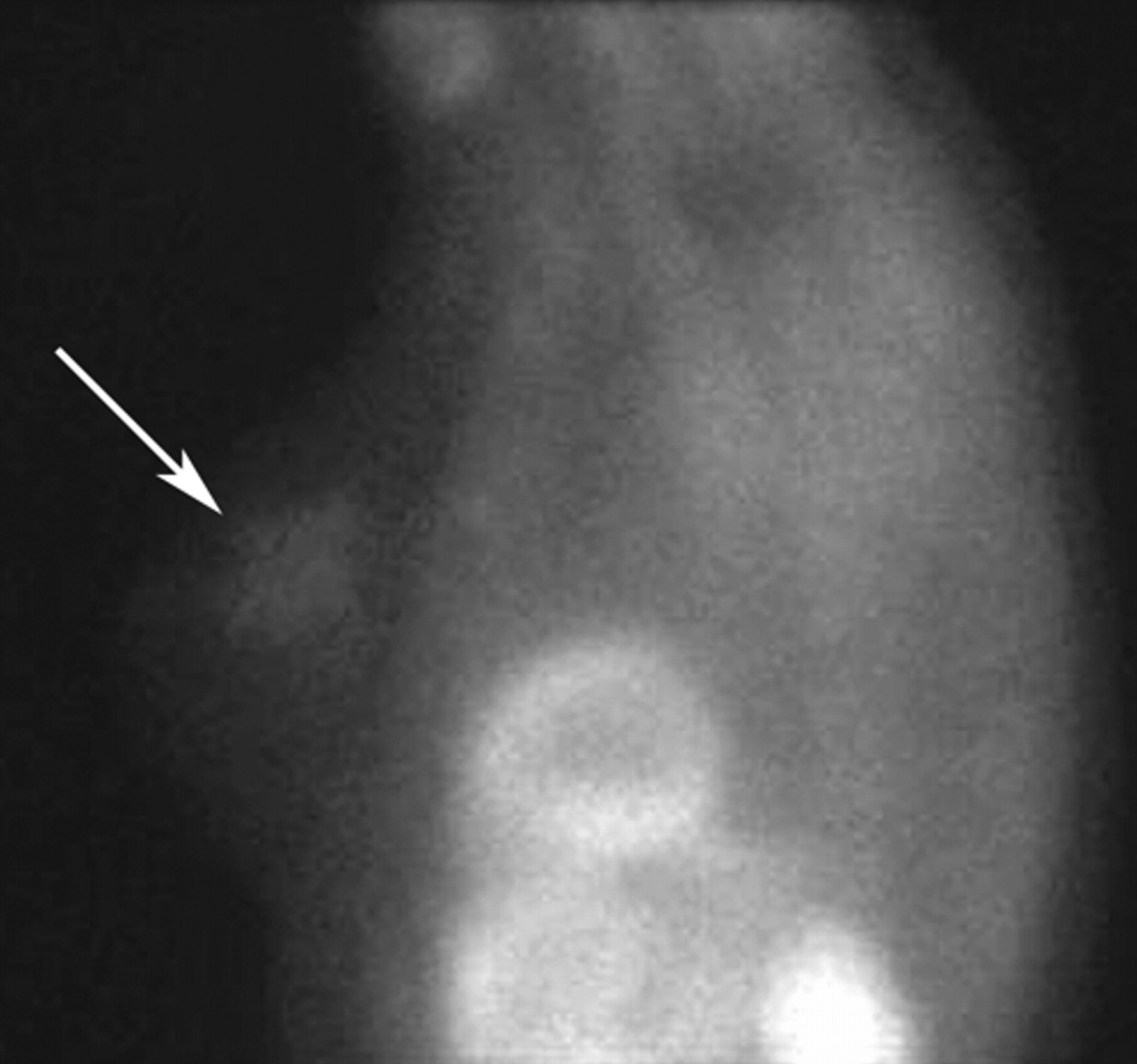
- FIGURE 4.
Dacroscintigraphy study demonstrating bilateral obstruction. Images at 3 time points reveal bilateral obstruction within nasolacrimal ducts (arrows).
- FIGURE 5.
Normal LeVeen shunt study. Images at 10, 20, and 30 min demonstrate rapid arrival of 99mTc-MAA in lungs with increasing activity over time, confirming patency of shunt. Activity inferior to lungs represents injected activity in peritoneal cavity.
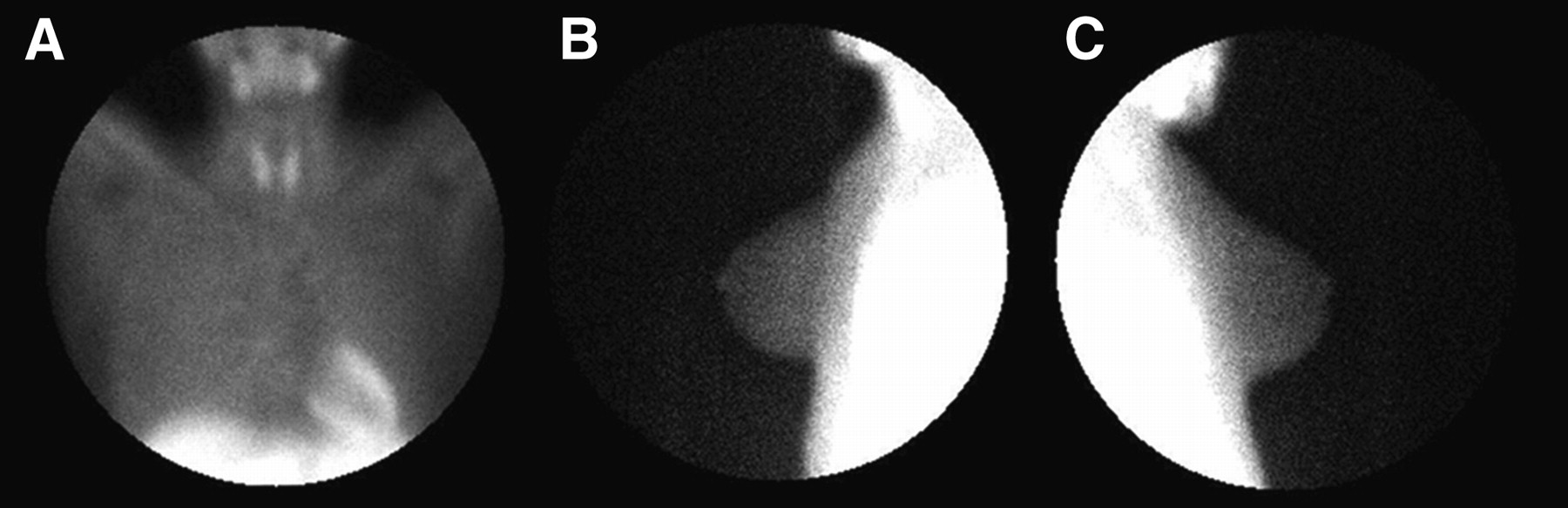
- FIGURE 6.
Anterior (A), left lateral (B), and right lateral (C) views of normal scintimammogram.
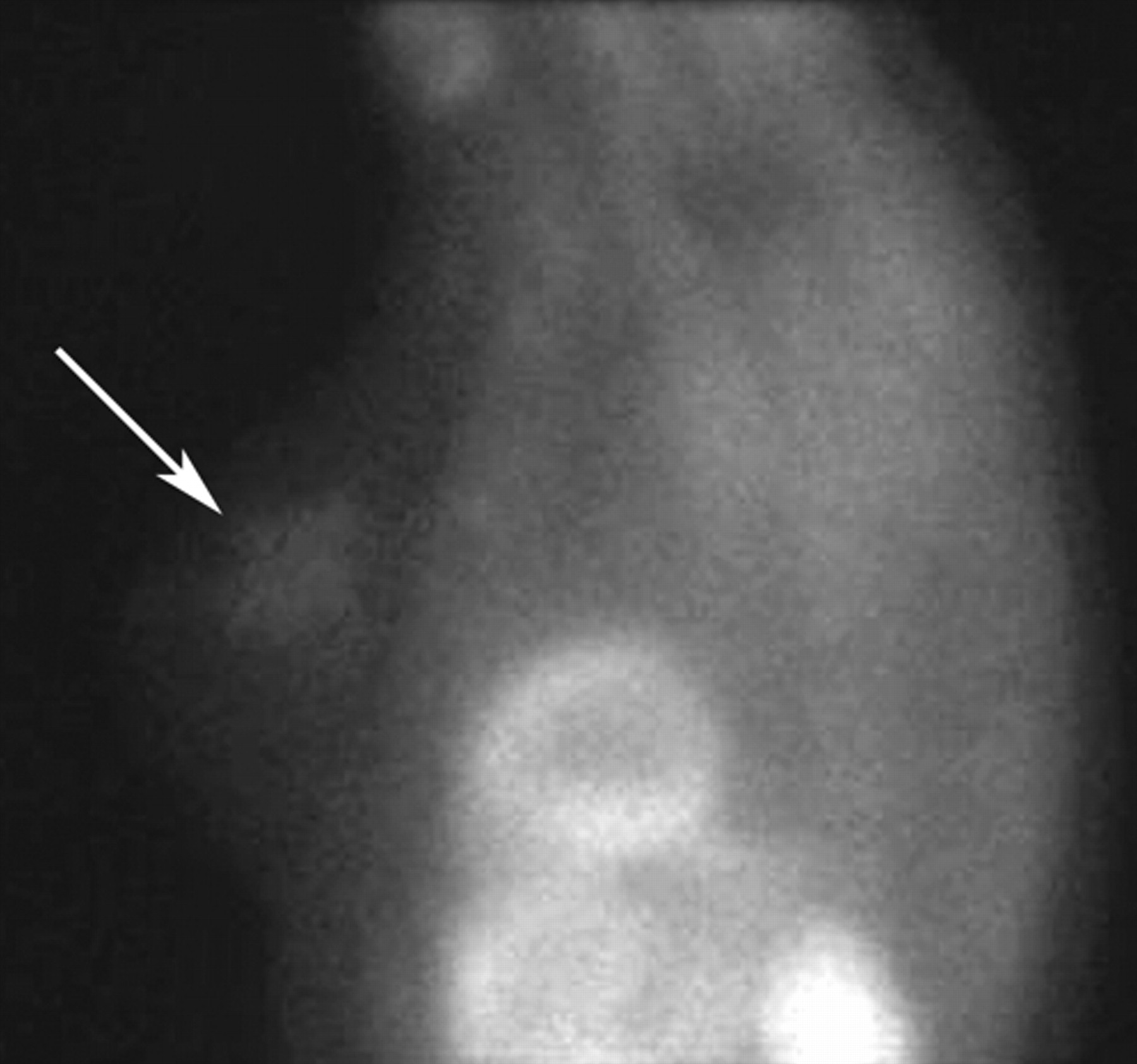
- FIGURE 7.
Abnormal accumulation of 99mTc-sestamibi (arrow) in left breast consistent with malignancy. Biopsy confirmed infiltrating lobular carcinoma.
- FIGURE 8.
(A) Right lateral static view of scintimammogram. Small abnormal accumulation of activity is seen close to chest wall. (B) 30° posterior oblique view significantly increases visualization of lesion.
- FIGURE 9.
Relatively normal whole-body 99mTc-MAA study. Note little activity outside lungs.
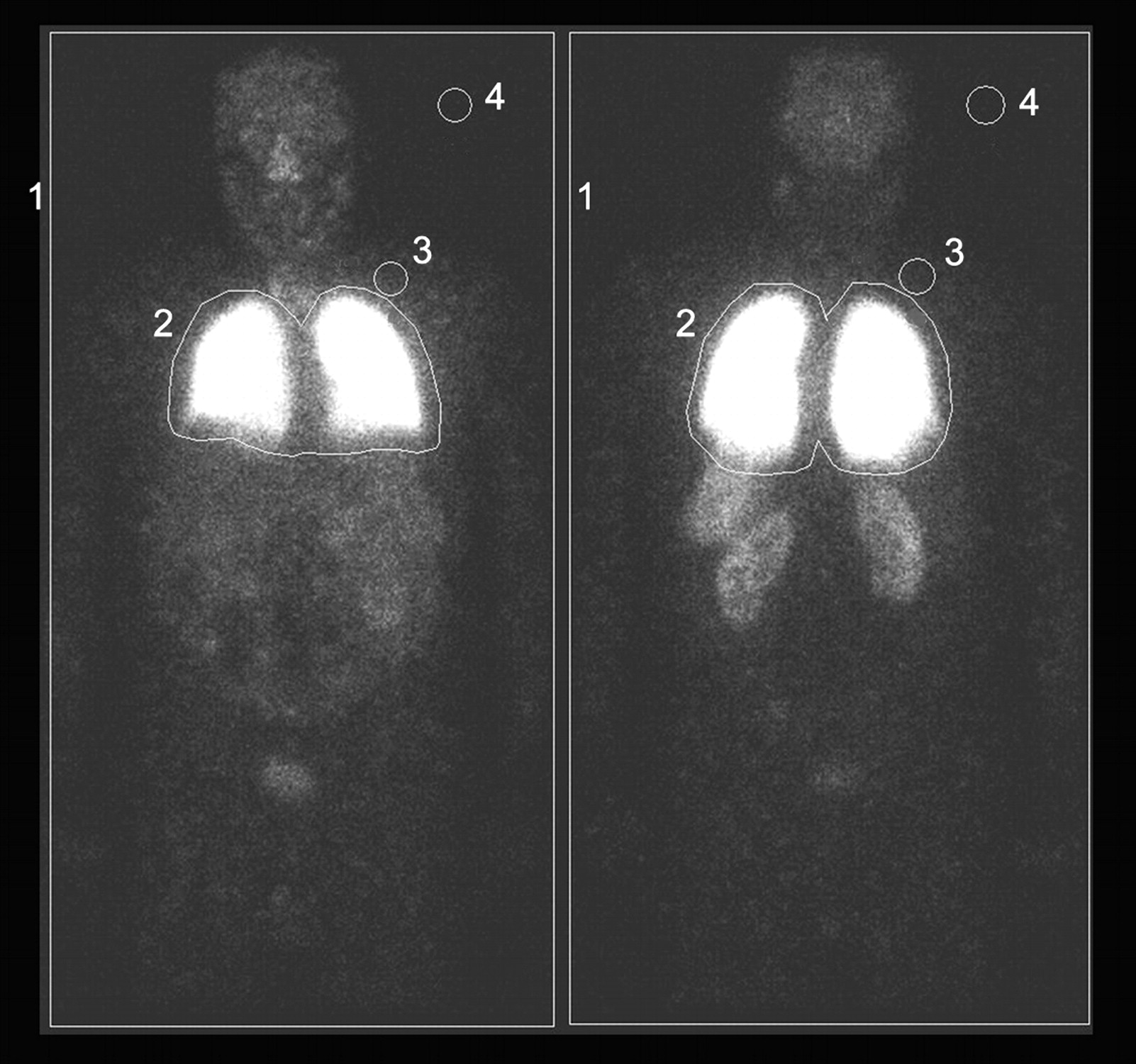
- FIGURE 10.
Whole-body 99mTc-MAA study in patient with R-L shunting resulting from hepatopulmonary syndrome. Abnormal uptake, indicative of shunting, in several organs including brain, thyroid, spleen, kidneys, and bowel is shown. ROIs around whole body (1), lungs (2), background soft tissue adjacent to lungs (3), and room background (4) are used in calculation of shunt (as discussed in text).
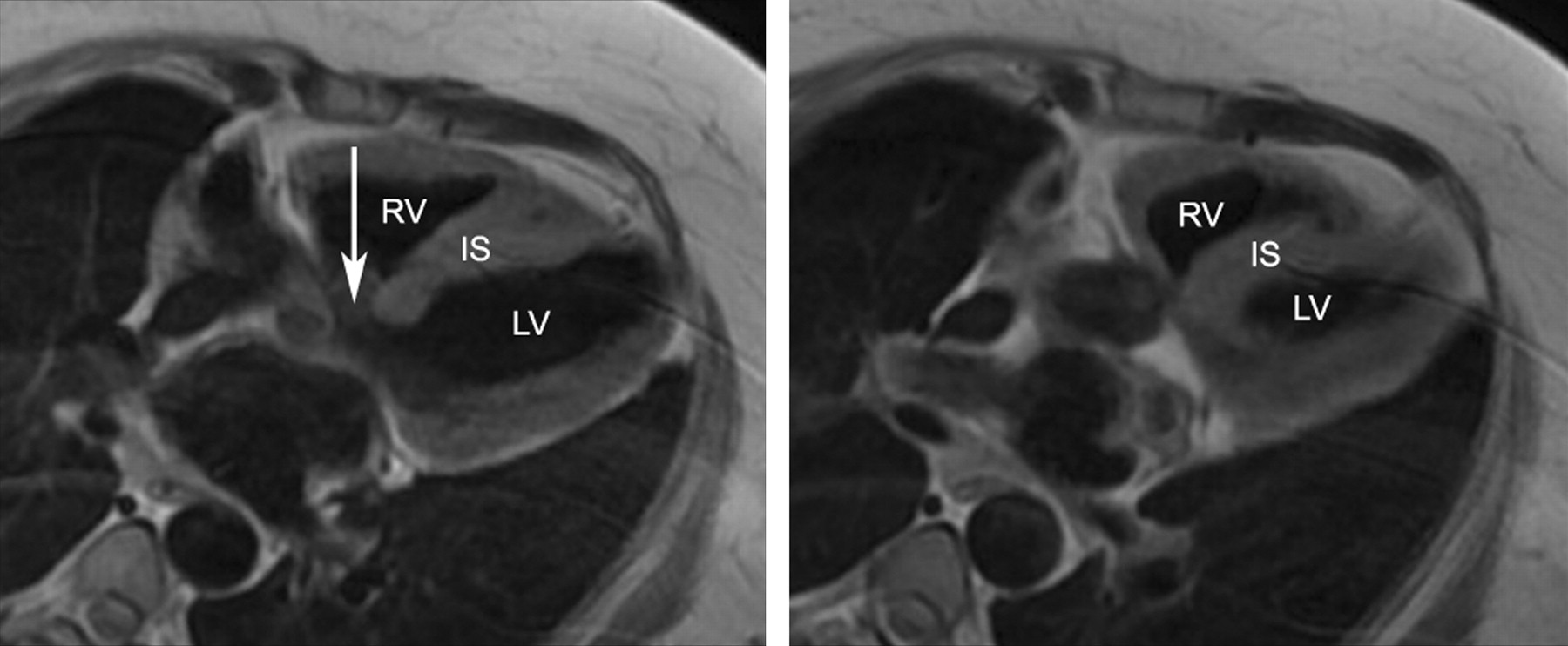
- FIGURE 11.
Two horizontal long-axis images from cardiac MRI in patient with VSD resulting in L-R shunt. Left image demonstrates defect (arrow) in IS. Right image is more inferior and demonstrates normal complete septum at this level. RV = right ventricle; IS = intraventricular septem; LV = left ventricle.
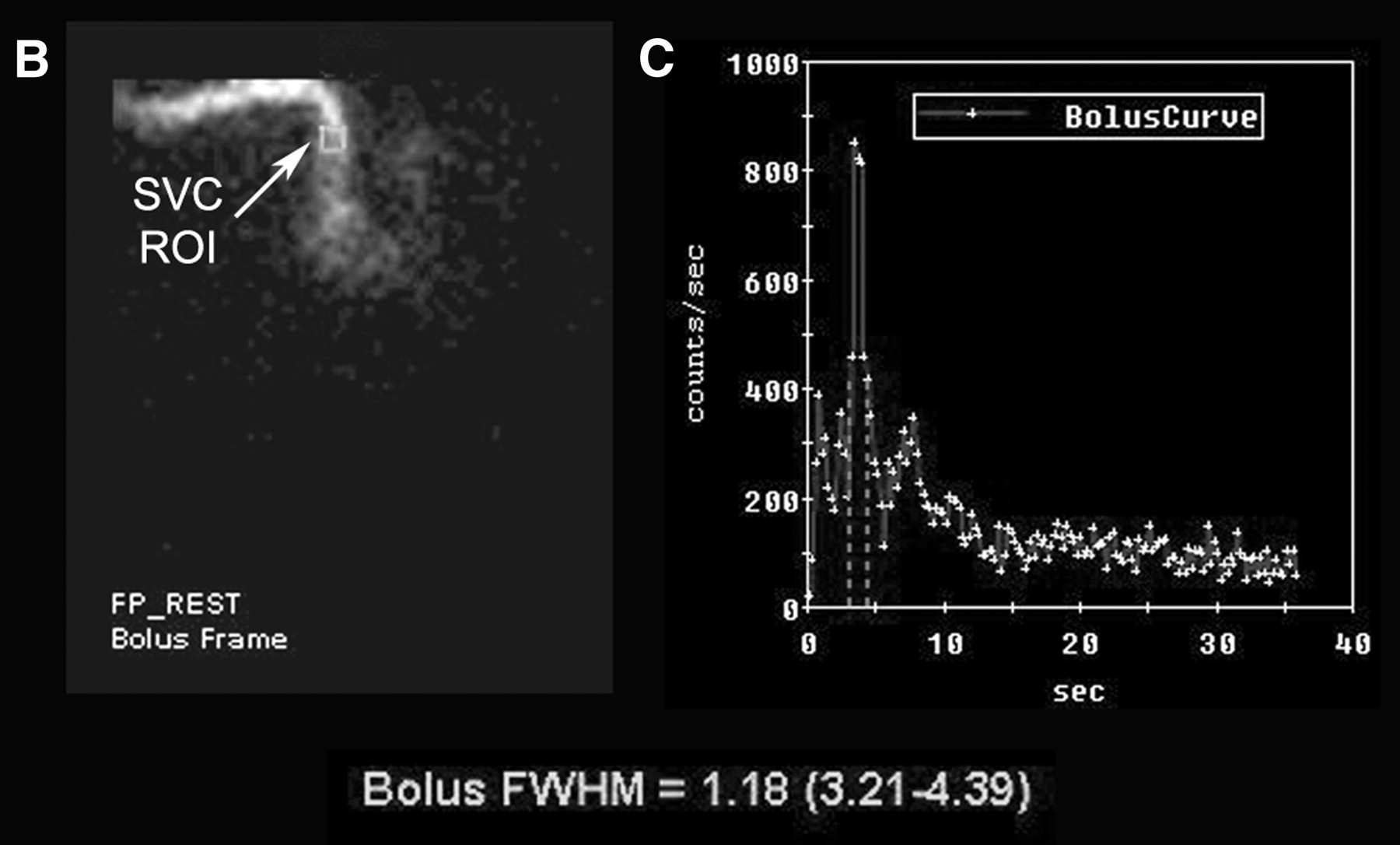
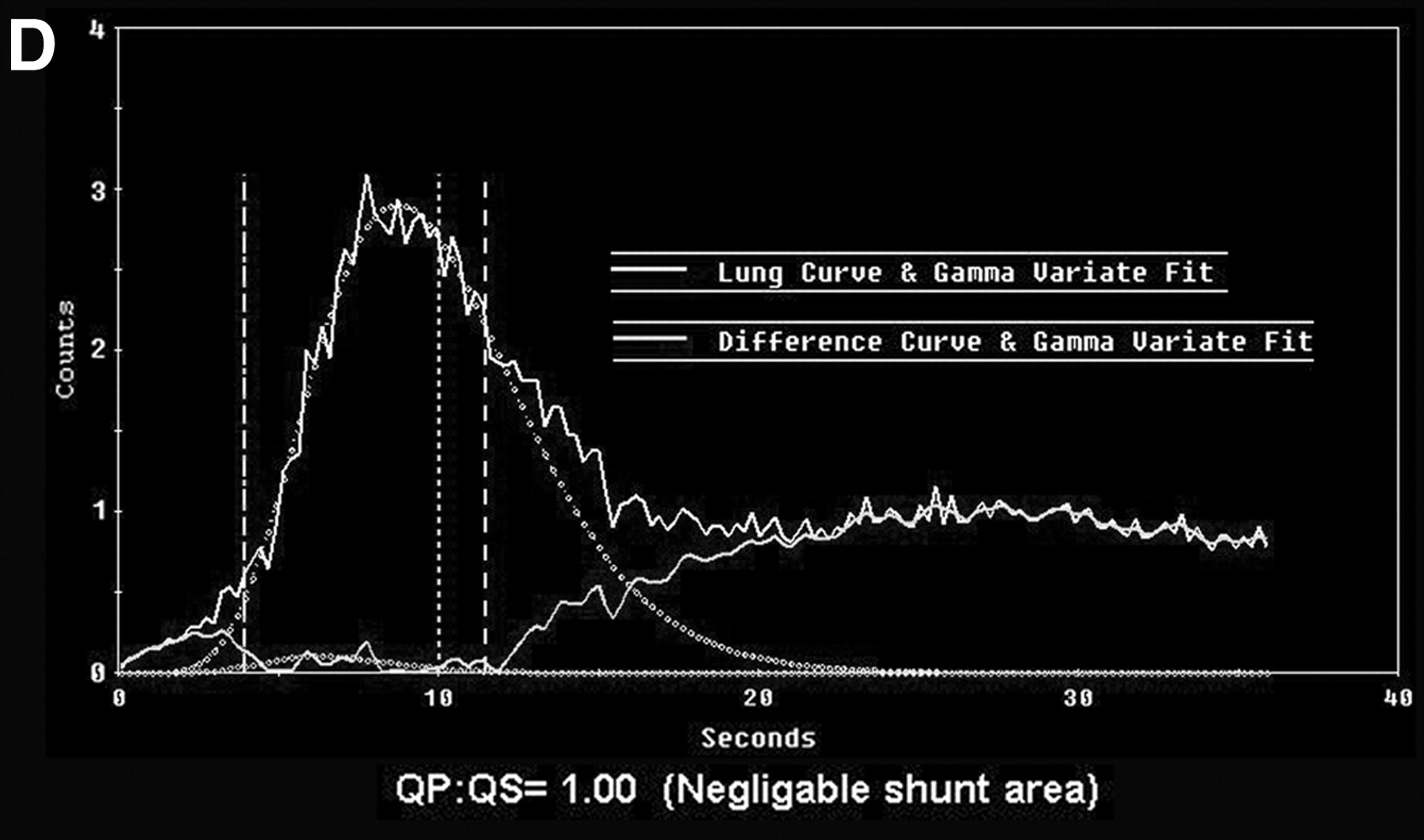
- FIGURE 12.
Normal first-pass L-R shunt study in same patient as in Figure 11. (A) Dynamic images demonstrate sequential arrival of activity in SVC, right side of heart, pulmonary arteries, lungs, pulmonary veins, and left side of heart. (B) Assessment of adequacy of bolus. ROI has been placed over SVC (square), allowing input activity to be plotted (C). FWHM is 1.18, indicating good tight bolus has been attained. (D) Time–activity curve over lungs. Total activity is demonstrated by solid line. γ-variate analysis has separated out lung curve (broken curve). Difference (curve) between total activity curve and lung curve is consistent with recirculation after first pass through body. There is no additional curve early after lung curve to suggest premature recirculation from L-R shunt. This is reflected in analysis, which indicates normal Qp/Qs of 1.00. Consequently VSD is currently not physiologically significant.
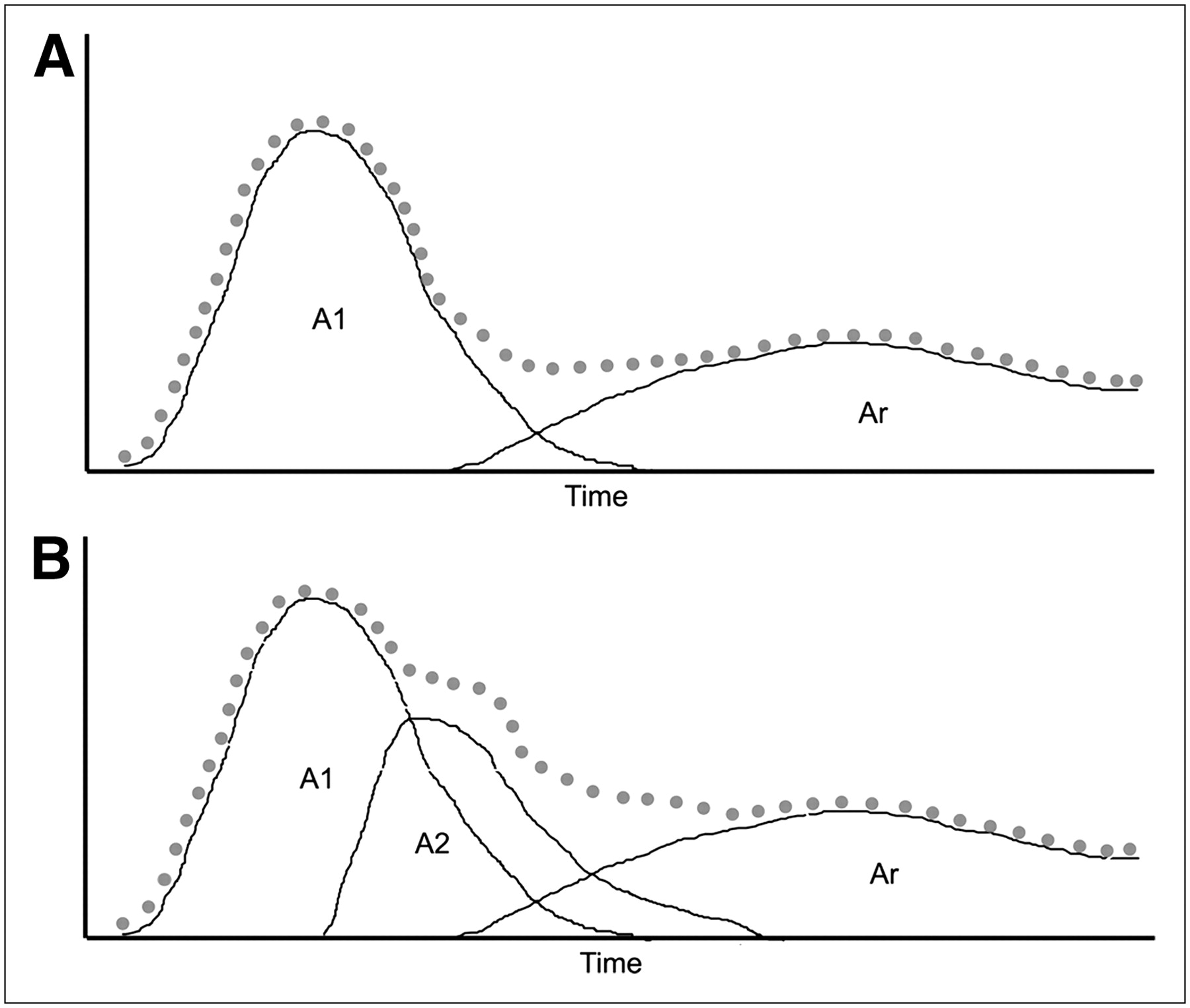
- FIGURE 13.
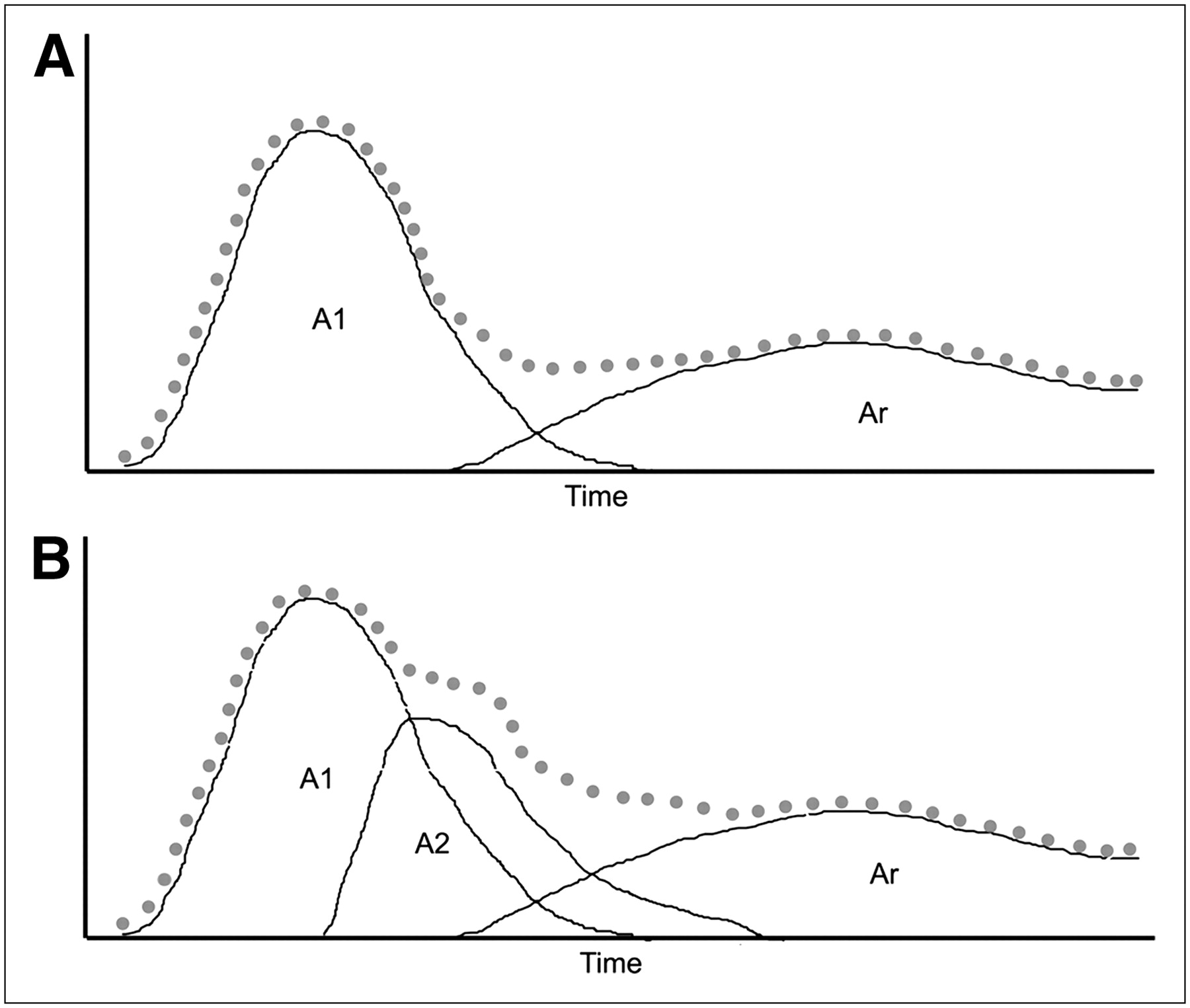
(A) Schematic of normal L-R shunt study. Dotted line reflects activity detected in lung ROI. γ-variate analysis deconstructs data into curves representing initial pass of activity through lungs, A1, and recirculated activity, Ar, after activity has circulated through body, back to heart, and onward through lungs again. (B) In setting of L-R shunt, there is reappearance of activity in lungs shortly after first pass, long before recirculation through body. This is detected as “bump” in downslope of time–activity curve. Magnitude of shunt is proportional to area under curve A2.
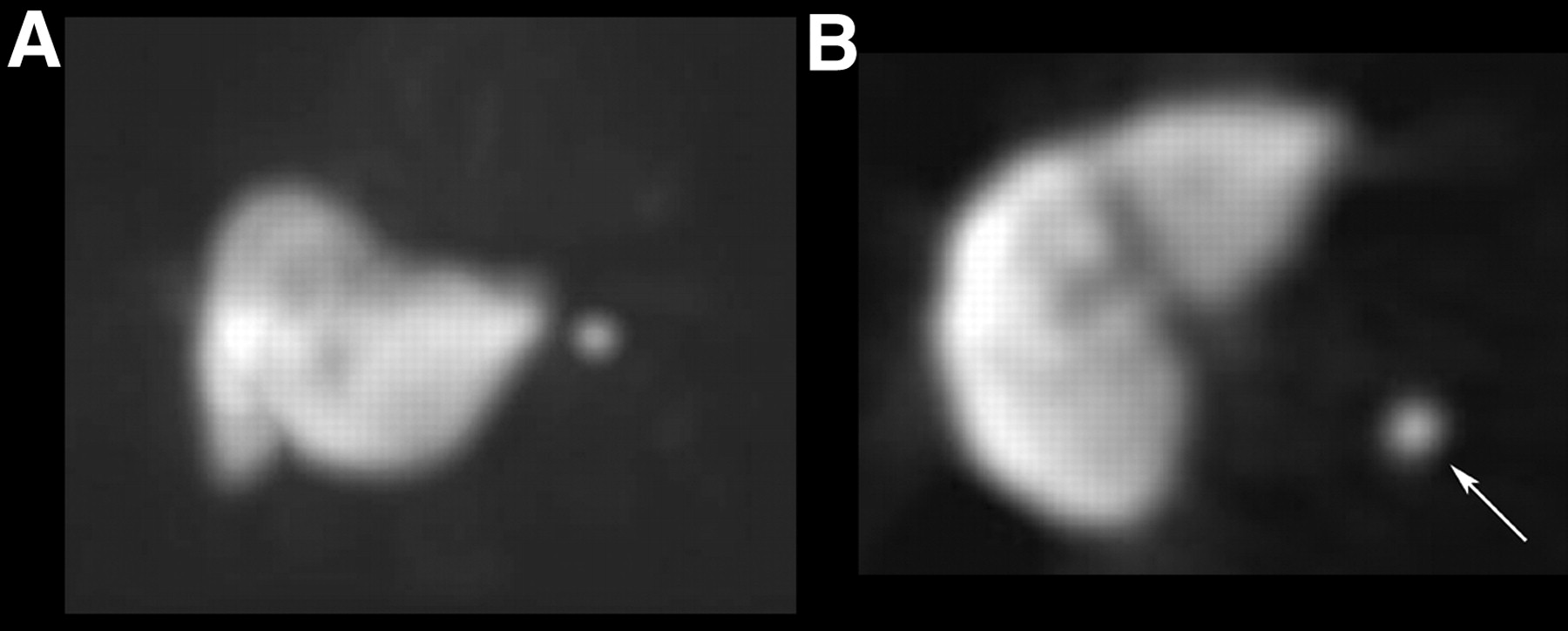
- FIGURE 14.
Heat-damaged RBC study assessing for presence of splenules in patient with ITP. Anterior MIP image (A) and transaxial image (B) from SPECT acquisition demonstrate small but intense focus of uptake in splenic bed (arrow), consistent with splenule. MIP = maximum intensity projection.
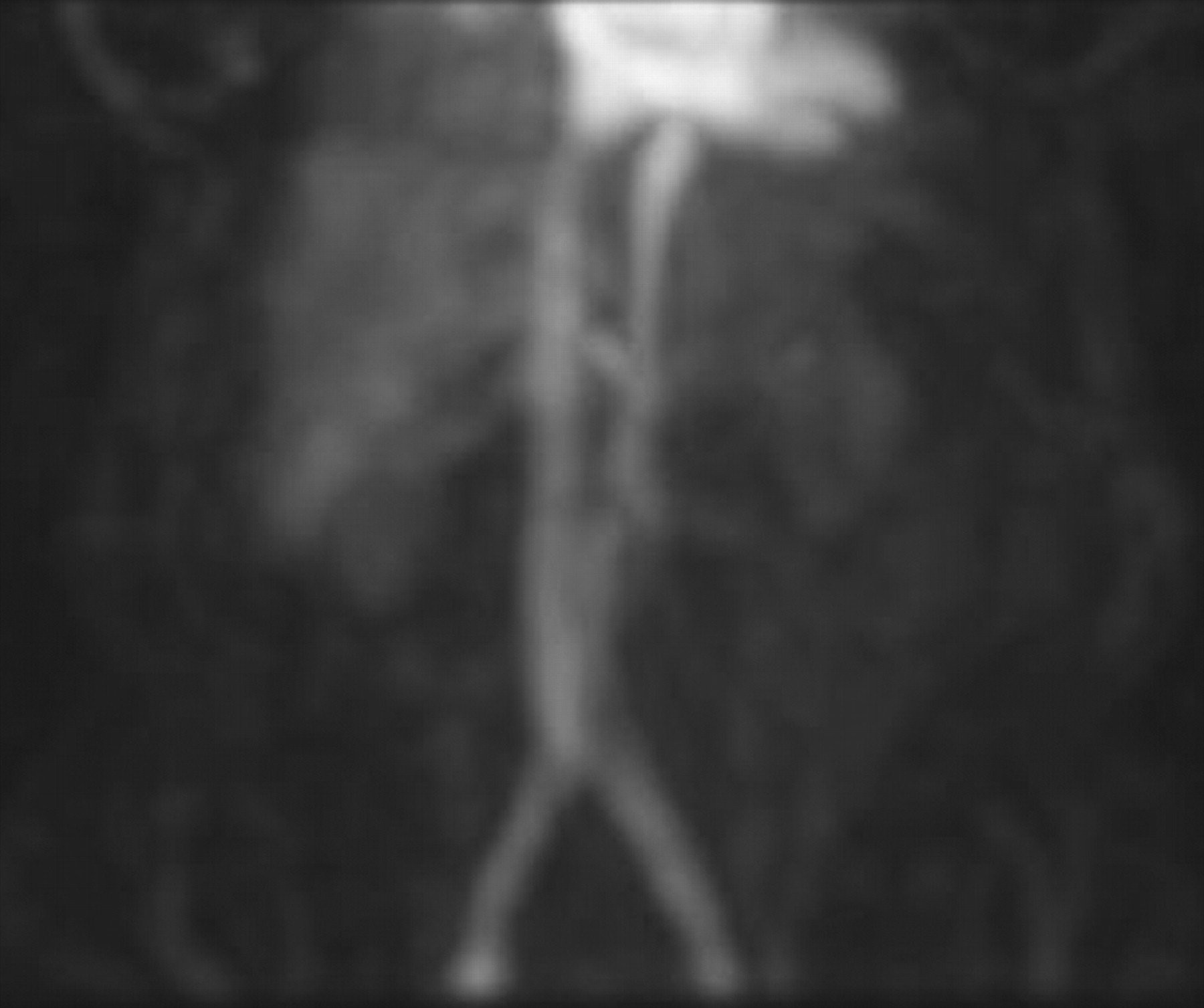
- FIGURE 15.
Anterior MIP image demonstrates no concentration of heat-damaged RBCs within accessory splenic tissue. This negative study depicts distribution of damaged RBCs throughout blood pool when there is no significant functioning splenic tissue to sequester them. MIP = maximum intensity projection.
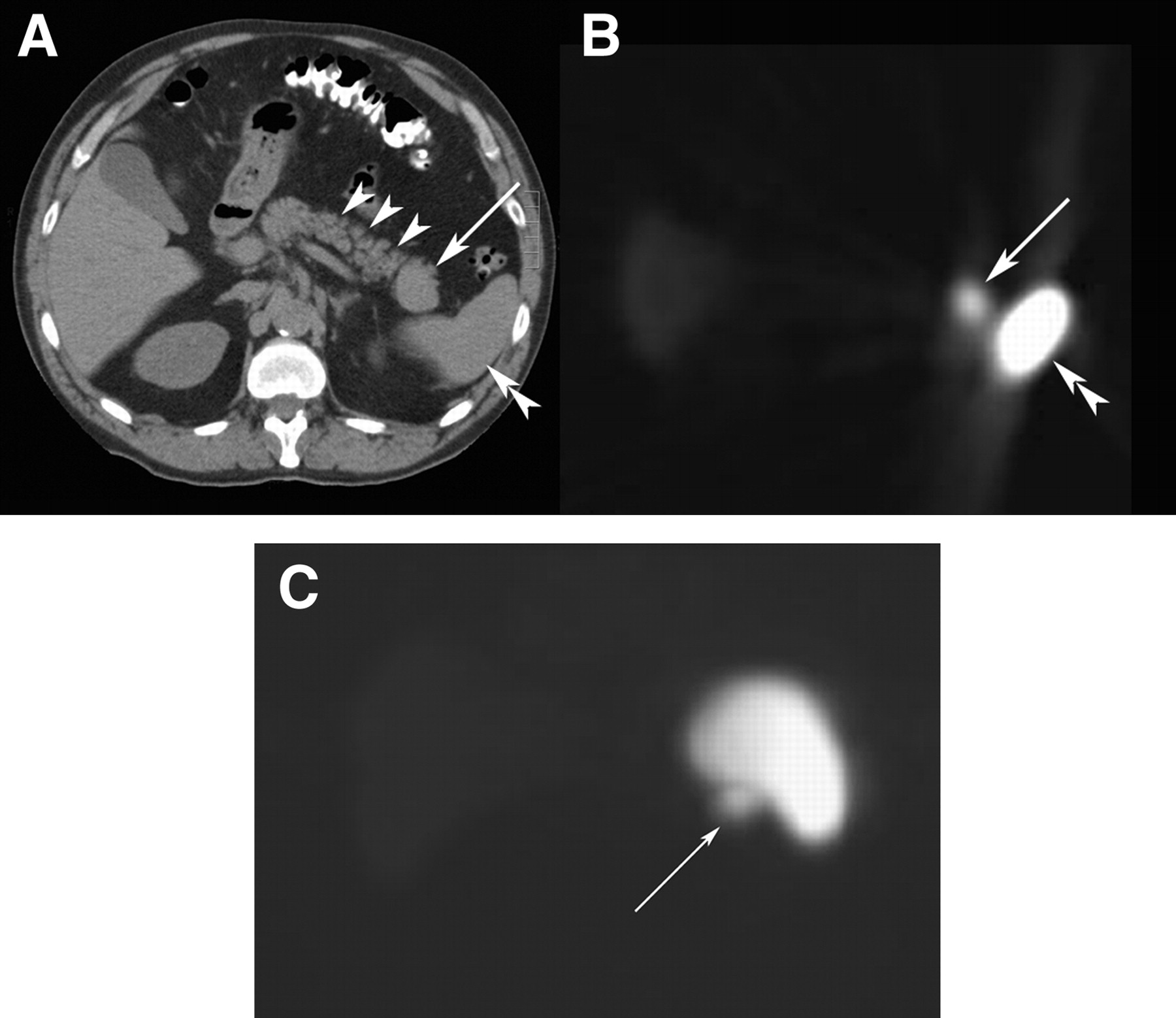
- FIGURE 16.
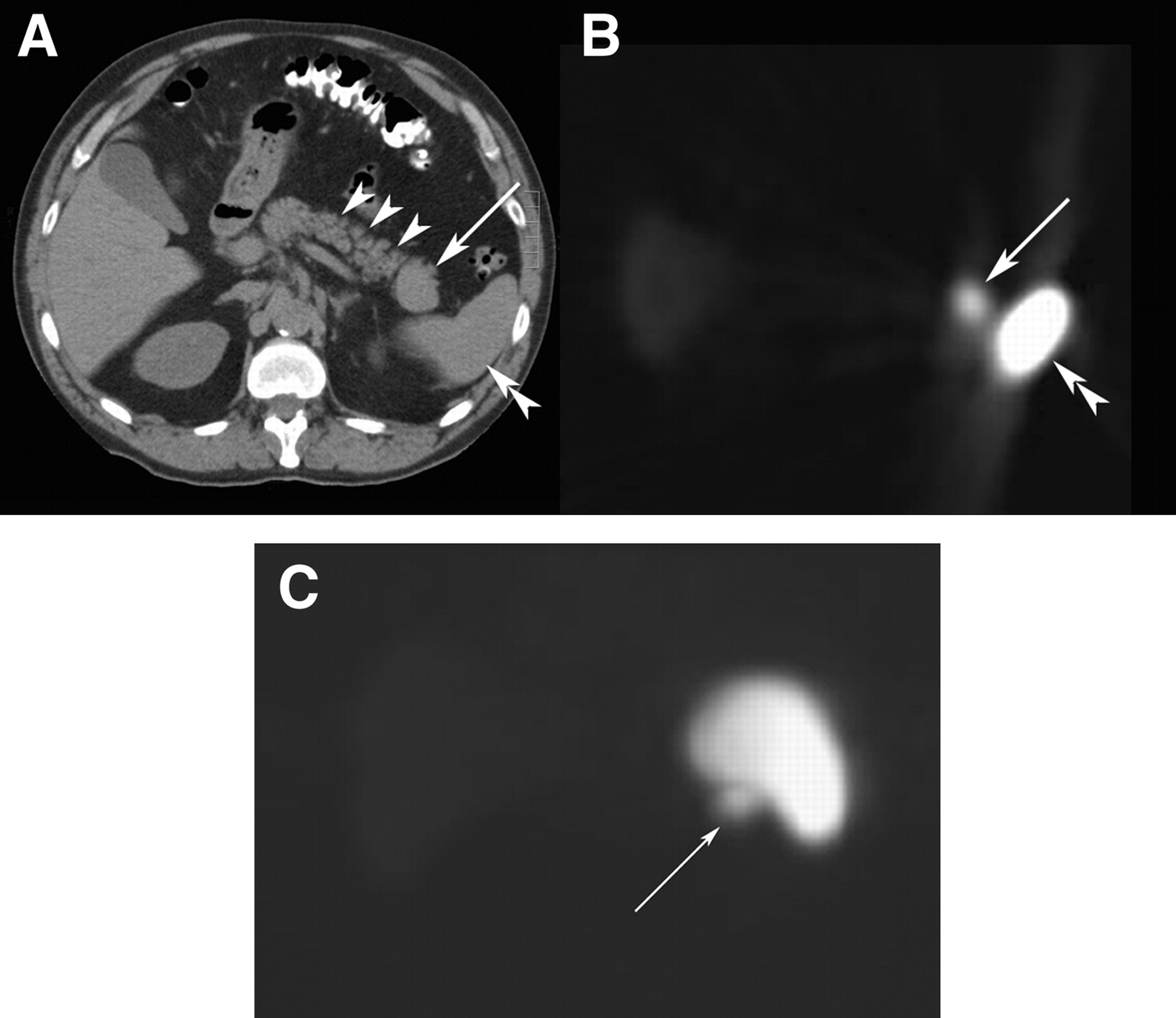
CT scan (A) revealed mass (arrow) near tail of pancreas (arrowheads) and spleen (double arrowhead). (B) Corresponding transaxial slice from heat-damaged RBC SPECT study demonstrates intense uptake in mass (arrow), confirming it is simply an accessory spleen. (C) Anterior MIP image further depicts uptake in mass (arrow) near splenic hilum. There is also intense normal uptake in spleen and faint uptake in liver. MIP = maximum intensity projection.















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}