


Abstract
We present a patient with a large hiatal hernia resulting in duodenogastric reflux that was seen as abnormal activity below and behind the heart (retrocardiac) on SPECT images and on 99mTc-tetrofosmin cardiac SPECT raw-data projection images. Incidental findings such as extra- and retrocardiac activity in the thorax and abdomen should be included on all comprehensive cardiac SPECT reports.
Approximately only 4% of 99mTc-labeled perfusion agents such as 99mTc-tetrofosmin or sestamibi is localized in the heart. Because the rest of the pharmaceutical is excreted mainly to the duodenum via the hepatobiliary system, duodenogastric reflux can sometimes be detected on the raw-data images of cardiac SPECT studies (1–3). During acquisition of cardiac SPECT images using 99mTc-labeled perfusion agents such as 99mTc-tetrofosmin and sestamibi, the field of view covers the essential organs of the thorax and abdomen. The abdominal organs such as the upper gastrointestinal tract, liver, gallbladder, stomach, spleen, and small bowel are thus imaged, as on a 99mTc-diisopropyl iminodiacetic acid hepatobiliary scintigraphy study. Therefore, abnormalities in the abdominal organs such as the upper gastrointestinal tract, liver, gallbladder, and spleen can easily be detected.
Abnormal esophageal conditions such as postoperative esophageal carcinoma or Barrett's esophagus may constitute an abnormal area of retrocardiac activity (4,5). We present a patient with a large hiatal hernia that caused duodenogastric reflux to be exhibited on vertical and horizontal longitudinal SPECT images and on the raw-data projection images of a 2-d 99mTc-tetrofosmin cardiac SPECT study. Although the incidental findings in the extra- and retrocardiac regions of the thorax and abdomen did not affect the study, a comprehensive interpretation of any cardiac SPECT study should note these relevant findings.
CASE REPORT
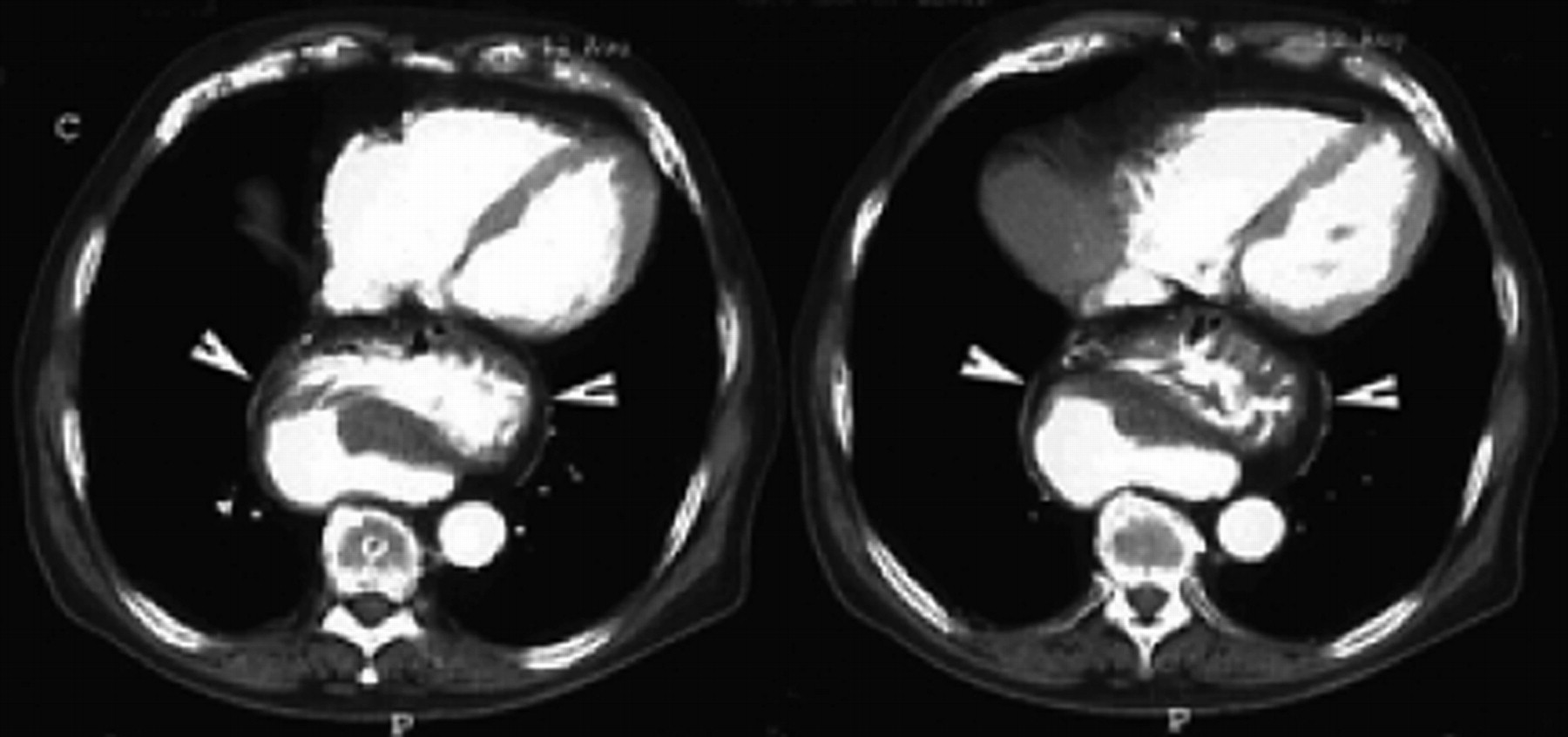
An 83-y-old male smoker with a history of cardiovascular disease and prostate cancer complained of atypical chest pain and was referred for a cardiac SPECT study. Two-day 99mTc-tetrofosmin cardiac gated images showed a fixed defect involving the apical and the apical anterior wall of the left ventricle, and the left ventricular ejection fraction was 54%. A rather large area of radioactivity was seen posterior to the basal heart on horizontal and vertical longitudinal SPECT images and was consistent with duodenogastric reflux on short-axis SPECT images (Fig. 1). Raw-data projection images showed duodenogastric reflux (Fig. 2A): a large area of abnormally increased activity in the area behind the heart (Fig. 2B). Concurrent CT of the chest showed a large intrathoracic hiatal hernia containing part of the stomach between the heart and the thoracic vertebrae, in the retrocardiac space (Fig. 3). The patient underwent an esophagogastroduodenoscopic examination, which showed a hiatal hernia, a small diverticulum in the lower third of the esophagus, and multiple linear superficial erosions in the gastric body and fundus.
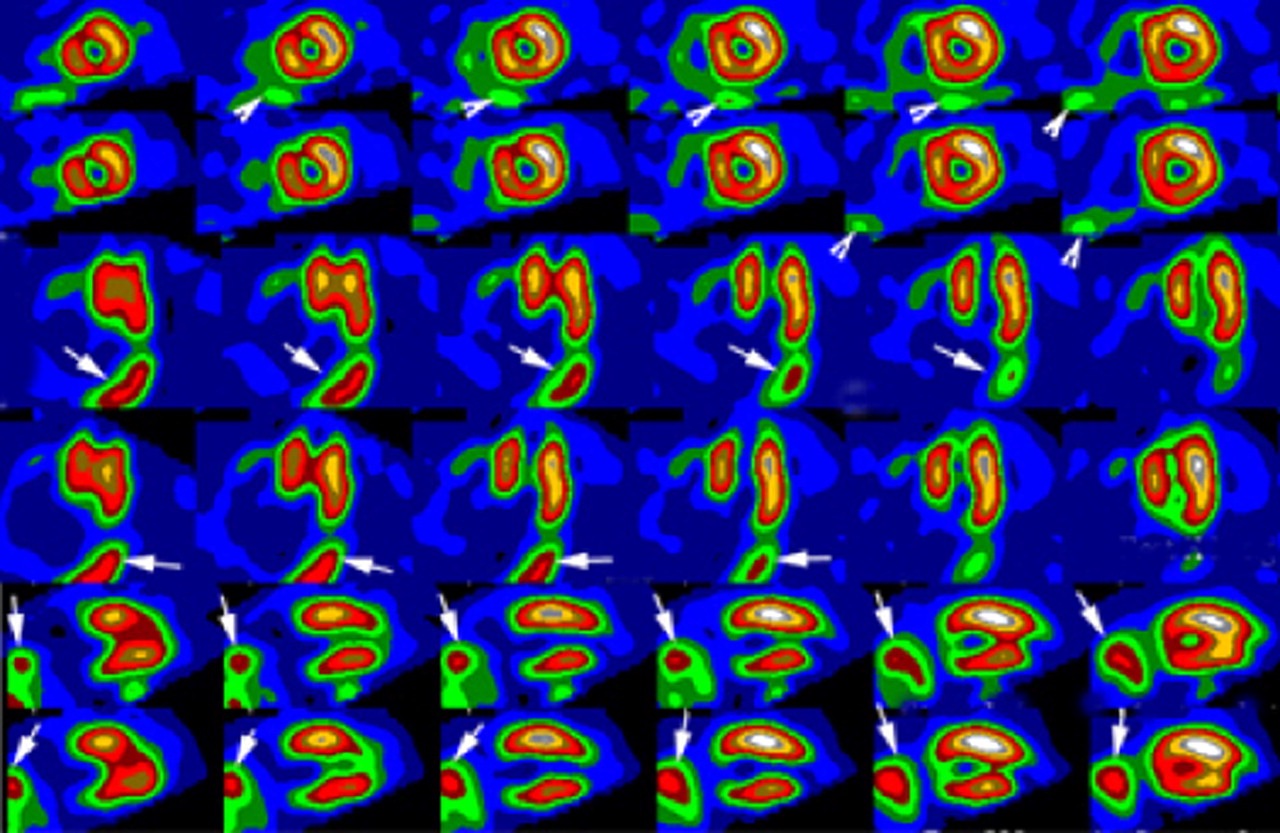
Two-day 99mTc-tetrofosmin SPECT images (top 2 rows, stress and rest short-axis slices; middle 2 rows, stress and rest horizontal slices; bottom 2 rows, stress and rest vertical slices) show absence of activity in apical wall and decreased activity in apical anterior wall. Increased activity in inferior to the inferior wall is noted on short-axis slices (arrowheads); large areas of activity (arrows) are noted in basal region on vertical and horizontal images.
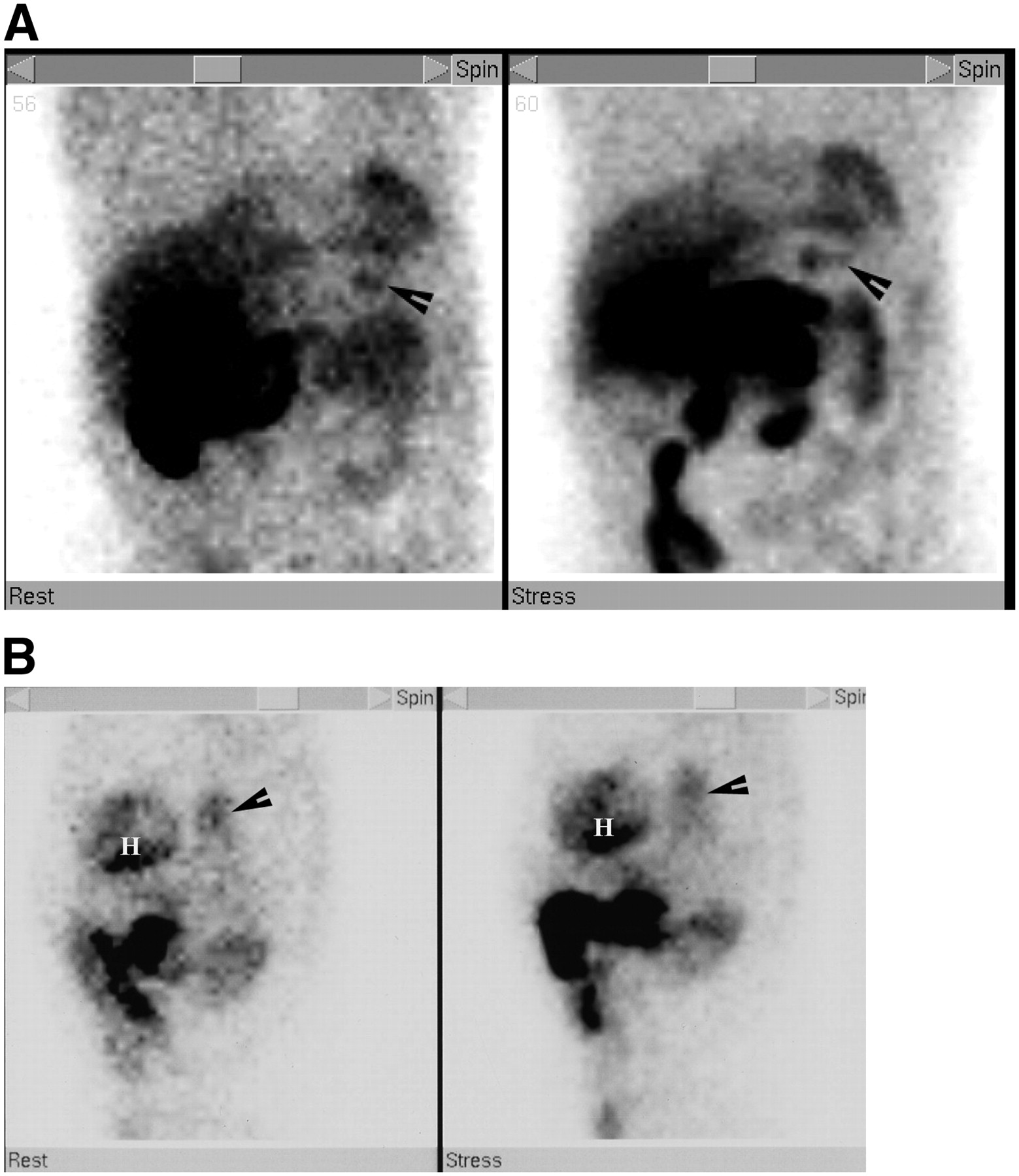
(A) Raw-data images in anterior projections at stress (right) and rest (left) on 2-d 99mTc-tetrofosmin SPECT study show duodenogastric reflux (arrowheads). (B) Raw-data images in left lateral projections on 2-d 99mTc-tetrofosmin SPECT study show extracardiac activity (arrows) in posterior aspect of heart (H) at rest (left) and stress (right).

Contrast-enhanced CT images of chest show large part of stomach and its omentum (arrowheads) between heart and thoracic vertebrae.
DISCUSSION
Postoperative esophageal carcinoma (1) or Barrett's esophagus (2) may cause extra- and retrocardiac activity on raw-data projection images on 99mTc-tetrofosmin cardiac SPECT studies. These findings are due to duodenogastroesophageal reflux. Because 99mTc-myocardial perfusion imaging agents such as 99mTc-tetrofosmin are excreted by the hepatobiliary system, duodenogastric reflux can be incidentally detected on a 99mTc-tetrofosmin cardiac SPECT study. The duodenogastric reflux demonstrated by our patient's SPECT study appeared to be due to a hiatal hernia, which exhibited duodenogastric reflux on short-axis SPECT images and bile regurgitation to the hiatal hernia on longitudinal SPECT images; these abnormalities were seen as retrocardiac activity on raw-data projection images (Fig. 2B). The large hiatal hernia was confirmed by CT of the chest as shown in Figure 3. Although the hiatal hernia could have been diagnosed on CT of the chest, CT images could not depict the presence or absence of duodenogastric reflux, which was visualized in this patient.
Cases of extracardiac activity posterior to the heart in hiatal hernia have been reported (6,7); however, in these reports, retrocardiac activity was described only on raw-data projection images; the reports did not describe retrocardiac activity or duodenogastric reflux on SPECT images. In our case report, we described 2 abnormal findings, namely duodenogastric reflux on short-axis SPECT images (Fig. 1) and retrocardiac activity from the hiatal hernia on long-axis images (Fig. 2B).
Interpretation of raw-data projection images on gated cardiac SPECT studies is essential both for quality control and for evaluating incidental abnormal findings in the thorax and abdomen. To further evaluate the possibility of a tumor or benign lesion in the thorax, other examinations such as chest radiography, chest CT, or upper gastrointestinal tract imaging may be helpful. Our patient's cardiac SPECT study concomitantly exhibited duodenogastric reflux and retrocardiac activity. The cause of the duodenogastric reflux appeared to be hiatal hernia, and the retrocardiac activity might have been either benign or malignant. The hiatal hernia seen on chest CT yielded the cause of the duodenogastric reflux and excluded the diagnosis of malignancy.
Footnotes
-
COPYRIGHT © 2007 by the Society of Nuclear Medicine, Inc.
References
- Received for publication February 26, 2007.
- Accepted for publication May 15, 2007.





{kind=link}
{kind=link}
{kind=link}