


Abstract
Is there an ideal myocardial perfusion imaging protocol? In order to answer this question and choose a protocol for clinical use, one must understand the characteristics of the available radiopharmaceuticals, the protocol variables, and the advantages and disadvantages of each. After reading this article, the technologist should be able to list the ideal characteristics of a myocardial perfusion imaging agent, describe and compare the characteristics of myocardial perfusion imaging agents, discuss the relationship between coronary blood flow and myocardial uptake of various tracers, describe imaging protocols, and discuss the advantages and disadvantages of each protocol.
Scintigraphic evaluation of myocardial perfusion for the diagnosis of coronary artery disease is a valuable noninvasive diagnostic imaging modality. 201Tl was introduced as a myocardial perfusion imaging agent in the early 1970s and remained in common use until the mid-1980s, when 99mTc-labeled radiopharmaceuticals were developed and, for the most part, replaced thallium for evaluating myocardial perfusion abnormalities. The numbers of procedures performed have grown exponentially since the advent of 99mTc-labeled radiopharmaceuticals for myocardial perfusion imaging.
The development of new radiopharmaceuticals, a newer generation of advanced γ-cameras with SPECT capabilities, and PET has dramatically revolutionized myocardial perfusion imaging. It is only natural to expect that this evolutionary process would lead to the development of various imaging protocols dealing with many variables, such as those pertaining to γ-cameras, radiopharmaceuticals, reimbursement issues, hospital discharge policies, scheduling logistics for outpatient clinics, and patients' demographics and convenience.
The purpose of this review was to compare the salient features of the available protocols, the advantages and disadvantages of each protocol, and the kinetics of various radiotracers to gain a better understanding of the many and often competing imaging protocols. There is a plethora of literature dealing with numerous issues pertaining to every available protocol. Novices are often confused when deciding which protocol to use.
Following is a basic review of the physical properties, biodistribution, and kinetics of each radiotracer.
RADIOPHARMACEUTICALS
Ideally, a radiopharmaceutical for myocardial perfusion imaging should have the following characteristics: myocardial uptake directly proportional to blood flow, high extraction fraction, high target-to-background ratio, and good myocardial retention and photon flux for optimal imaging.
201Tl
201Tl is a cyclotron-produced potassium analog radioisotope with a half-life of 73 h. It produces γ-energy rays of 170 keV (∼10%) and 135 keV (∼3%). The photons resulting from electron capture have energies of 69–80 keV (abundance) and are the photons used for imaging. The first-pass myocardial extraction of 201Tl is ∼85%; however, only about 3%–5% of the total injected dose localizes in the myocardium when injected at peak exercise. The initial 201Tl uptake within the myocardium occurs through the active Na-K adenosine triphosphatase transport system. After the initial extraction, 201Tl redistributes within the myocardium. 201Tl has a relatively short myocardial retention. The injected dose is low (74–148 MBq [3–4 mCi]). The counting statistics are fair. The radiation dosimetry is not favorable because of the high total body absorbed dose, 0.68 rad (1).
99mTc-Sestamibi
Sestamibi is an isonitrile compound that, when labeled with 99mTc, has a half-life of 6 h. It produces γ-energy rays of 140 keV (abundance), which are ideal for imaging. 99mTc-Sestamibi is extracted from the coronary circulation in proportion to the coronary blood flow. The first-pass myocardial extraction fraction of 99mTc-sestamibi is 55%–68%. The myocardial extraction is lower than that of 201Tl but adequate. 99mTc-Sestamibi myocardial cellular retention occurs specifically within the mitochondria as a result of an electrostatic interaction. Myocardial retention is prolonged. The myocardial uptake of 99mTc-sestamibi is ∼1.2%–1.5% of the injected dose. Unlike 201Tl, 99mTc-sestamibi shows minimal redistribution. The injected dose of 99mTc-sestamibi is higher than that of 201Tl, resulting in better counting statistics for imaging. The radiation dosimetry is favorable, with a total body absorbed dose of 0.50 rad (1).
99mTc-Tetrofosmin
Tetrofosmin is a diphospine compound that, when labeled with 99mTc, has a half-life of 6 h and produces γ-energy rays of 140 keV. 99mTc-Tetrofosmin is taken up by the myocardium in proportion to the coronary blood flow. The first-pass myocardial extraction fraction is ∼54%. Approximately 1.2% of the injected dose localizes in the myocardium. The myocardial uptake, retention, and blood clearance of 99mTc-tetrofosmin are similar to those of 99mTc-sestamibi. There is little redistribution. The hepatic clearance of 99mTc-tetrofosmin is faster than that of 99mTc-sestamibi (1). As with 99mTc-sestamibi, the injected dose is higher than that of 201Tl, resulting in better counting statistics.
99mTc-Teboroxime
Teboroxime is a boronic acid–derived, neutral lipophilic compound that, when labeled with 99mTc, has a half-life of 6 h and produces γ-energy rays of 140 keV. Myocardial cell uptake is proportional to coronary blood flow. Being a neutral lipophilic compound, it passively diffuses across the myocardial cell membrane. The first-pass myocardial extraction fraction is high (>90%), and the washout is rapid. There is no redistribution. The injected dose is higher than that of other agents, resulting in good counting statistics for imaging. The radiation dosimetry is not favorable, with a total body absorbed dose of 0.83 rad (1). This imaging agent is not commercially available in the United States at this time. It is, however, approved by the U.S. Food and Drug Administration as a myocardial perfusion imaging agent.
99mTc-N-NOET
99mTc-N-NOET is a new myocardial perfusion imaging agent that is comparable to 201Tl. It is a neutral lipophilic agent. Biodistribution studies have demonstrated selective myocardial localization. Myocardial uptake is directly proportional to coronary blood flow. The first-pass myocardial extraction fraction is high. 99mTc-N-NOET redistributes like 201Tl, thus allowing initial stress and delayed rest imaging. Clearance of pulmonary activity is rapid. The image quality is good because of low background interference. The stress and rest images provide comparable information for the diagnosis of ischemia (2,3). This agent is not yet approved for routine use in the United States.
COMPARISON OF 201TL AND 99MTC-LABELED MYOCARDIAL PERFUSION IMAGING TRACER KINETICS
Following is a brief discussion of various tracer kinetic parameters for 201Tl and 99mTc-sestamibi showing how the 2 radiotracers differ. A detailed discussion of these parameters is beyond the scope of this article.
The myocellular uptake of 201Tl is dependent on Na-K adenosine triphosphatase. The myocardial uptake of 201Tl declines with Na-K pump inhibition from adenosine triphosphate depletion. The myocellular uptake of 99mTc-sestamibi reflects the mean plasma membrane potential. 99mTc-Sestamibi is retained within the mitochondria as a result of an electrostatic interaction. It declines to low levels with severe cell injury (4).
Myocardial transmicrovascular transport of 201Tl and 99mTc-sestamibi is variable at different blood flow levels. The capillary permeability for 201Tl is greater than that for 99mTc-sestamibi. The parenchymal cell permeability surface area for 99mTc-sestamibi is much higher than that for 201Tl (5).
The tracer kinetics of 201Tl and 99mTc-sestamibi across myocytes are affected by low-flow ischemia. During low-flow ischemia, the information provided by 201Tl or 99mTc-sestamibi SPECT imaging is dependent on myocardial perfusion and not on a cellular metabolic disorder (6).
RELATIONSHIP BETWEEN CORONARY BLOOD FLOW AND MYOCARDIAL UPTAKE OF VARIOUS RADIOTRACERS
The various kinetics and biodistributions of different radiotracers determine myocardial uptake, retention, redistribution, and washout. The relationship between coronary blood flow and the myocardial uptake of radiotracers is not linear. All commonly used radiopharmaceuticals show a plateau “roll-off” at higher blood flow levels. The radiotracers show a significant roll-off at coronary blood flow levels exceeding 2.5 mL/min/g. The roll-off is the smallest for 201Tl and is larger for 99mTc-sestamibi and 99mTc-tetrofosmin (7). A comparison of the first-pass myocardial extraction fractions of various technetium-labeled agents and thallium is shown in Table 1.
Comparison of First-Pass Myocardial Extraction Fractions of Various 99mTc-Labeled Agents and 201Tl
PHYSICAL AND BIOLOGIC COMPARISONS OF MYOCARDIAL PERFUSION IMAGING AGENTS
There are significant differences in the physical and biologic properties of 201Tl and 99mTc-labeled radiopharmaceuticals. Table 2 shows a comparison of various factors affecting the myocardial uptake of the radiotracers.
Physical and Biologic Comparisons of Myocardial Perfusion Imaging Agents
VARIOUS IMAGING PROTOCOLS
201Tl Imaging
Myocardial perfusion imaging with 201Tl was commonly used until 99mTc-labeled radiotracers became available. The most commonly used procedure involves administering ∼148 MBq (∼4 mCi) of 201Tl at peak exercise. Stress imaging is performed immediately after the 201Tl injection (beginning within 5–7 min of the injection). Delayed rest (redistribution) images are obtained at 3–4 h after injection. There are several variations of delayed imaging, which can be done at up to 24 h to assess viability. In addition, a 201Tl reinjection technique with an additional booster dose of 37–55.5 MBq (1.0–1.5 mCi) is used to assess myocardial viability.
Myocardial Perfusion Imaging with 99mTc-Labeled Radiopharmaceuticals (Sestamibi or Tetrofosmin)
Two-Day Protocol.
Two-day protocols are best in terms of taking advantage of the physical properties, pharmacokinetics, and acquisition, processing, and display parameters of 99mTc-labeled agents. Typical doses for 1- and 2-d protocols are shown in Table 3.
Doses of 99mTc-Labeled Agents for Myocardial Perfusion Scintigraphy*
The advantages of 2-d protocols are as follows: flexibility of scheduling stress–rest imaging; better patient flow; ability to image obese patients; higher dose; better gated rest–stress imaging; no cross talk or cross contamination; optimal defect contrast with minimal background activity; elimination of day 2 study if stress study is normal; and high accuracy for detecting coronary artery disease in patients with a low likelihood of coronary artery disease.
The disadvantages of 2-d protocols are as follows: the need for 2 d; inconvenience for patients; delay in diagnosis; and camera time relative to that used for dual-isotope simultaneous acquisition, which is not recommended because of energy window cross talk.
Imaging Protocol for 99mTc-Labeled Agents.
For stress imaging, 555 MBq–1.11 GBq (15–30 mCi) is injected at peak exercise. Gated SPECT is performed from 15 min to 2 h after injection, preferably within 15–30 min, to maximize stress myocardial defect contrast and minimize hepatobiliary and gastrointestinal interference.
For rest imaging, 555 MBq–1.11 GBq (15–30 mCi) is injected at rest. Gated SPECT is performed within 45–60 min after injection. A 60-min delay is optimal for adequate hepatobiliary clearance of the radiotracer.
Imaging too soon after injection will result in increased residual liver activity and increased counts in the adjacent inferior wall because of scatter and scaling. Waiting too long will decrease total myocardial count density and increase gastrointestinal interference. The optimal imaging window is when radiotracer activity has cleared from the liver and not concentrated in the gastrointestinal tract, that is, loops of bowel and the stomach (retrograde flow).
In the event that there is a significant splanchnic or bowel overlap with the inferior wall, various maneuvers, such as drinking water or milk or eating fatty food, can be tried to alleviate the problem before repeating delayed imaging.
One-Day Rest–Stress or Stress–Rest Protocol Performed with Sestamibi or Tetrofosmin.
The rest–stress sequence is significantly better than the stress–rest sequence in terms of detecting the reversibility of stress-induced perfusion deficits. With the stress–rest sequence, the rest activity obscures some of the stress defect, resulting in the degradation of image contrast and a reduction in the detection of true reversibility.
With the rest–stress sequence, there is a greater difference in counts between normal and abnormal areas of the myocardium on stress images. This difference results in better normalization of the abnormality on rest images. A 3- to 4-h delay between rest imaging and stress imaging allows radioactivity to decay by 29%–37%, thereby providing better image contrast (8,9). However, the American Society of Nuclear Cardiology guidelines (10) offer the option to proceed immediately from rest imaging to stress imaging during a 1-d protocol as long as the higher dose is 3.5–4.0 times the lower dose.
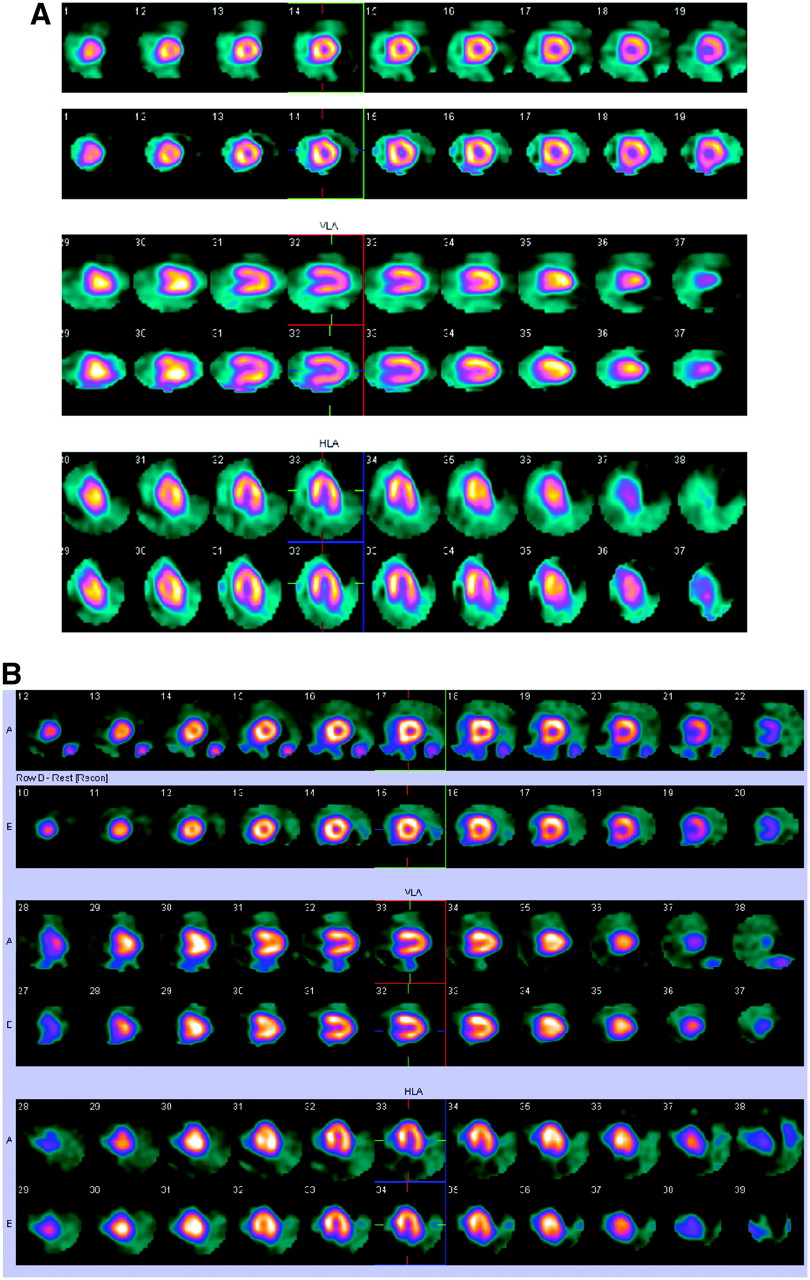
Images from a 2-d protocol and images from a 1-d (rest–stress) protocol are shown in Figure 1. Both studies are normal. The studies were obtained with the same camera. The images from the studies are very comparable in features and quality.

(a) Images obtained with 2-d 99mTc-sestamibi protocol. Findings are normal. (b) Images obtained with 1-d 99mTc-sestamibi protocol. Findings are normal.
One-Day Dual-Isotope Acquisition Protocol
A 1-d dual-isotope protocol with 201Tl and 99mTc-sestamibi can be performed with separate acquisition or simultaneous acquisition. In a separate acquisition of 201Tl rest images, the contribution of 201Tl to the 99mTc energy window is negligible (∼2.9%). Correction for cross contamination between the 2 energy windows is not required. The overall sensitivity and specificity for the detection of coronary artery disease are ∼90% (11,12).
Dual-Isotope Separate-Acquisition Protocol.
For the rest 201Tl–stress 99mTc protocol, 111–148 MBq (3–4 mCi) of 201Tl is injected in the upright position to decrease lung uptake. Rest 201Tl SPECT is performed after 10–15 min. When rest imaging is complete, the patient is sent for treadmill or pharmacologic stress testing. Next, 555 MBq–1.11 GBq (15–30 mCi) of the 99mTc-labeled agent is injected, and SPECT acquisition is begun at 15 min after injection.
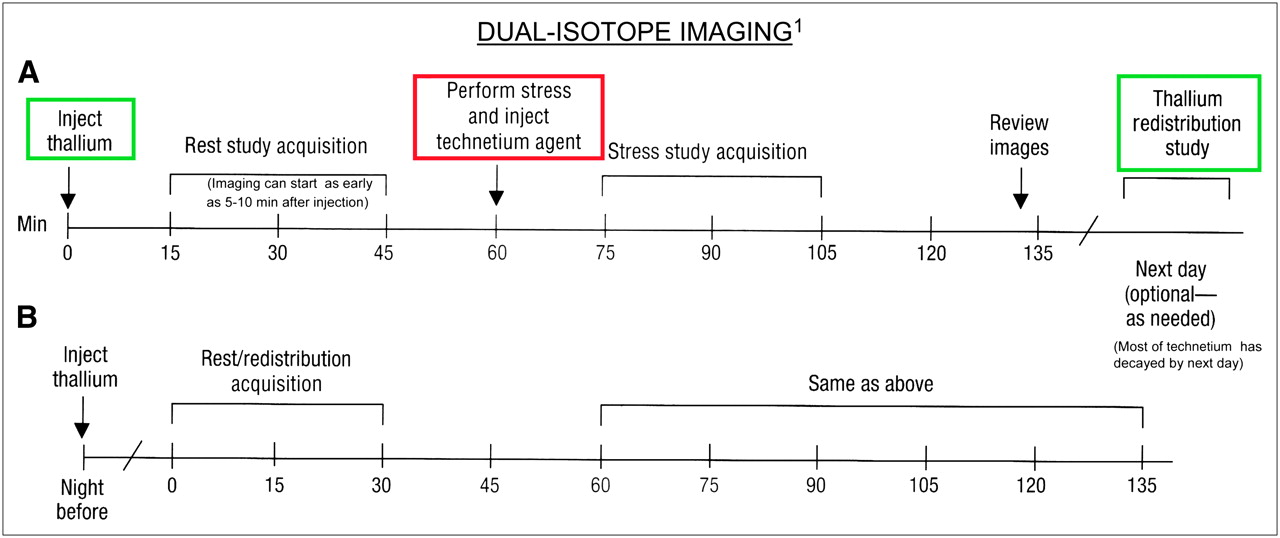
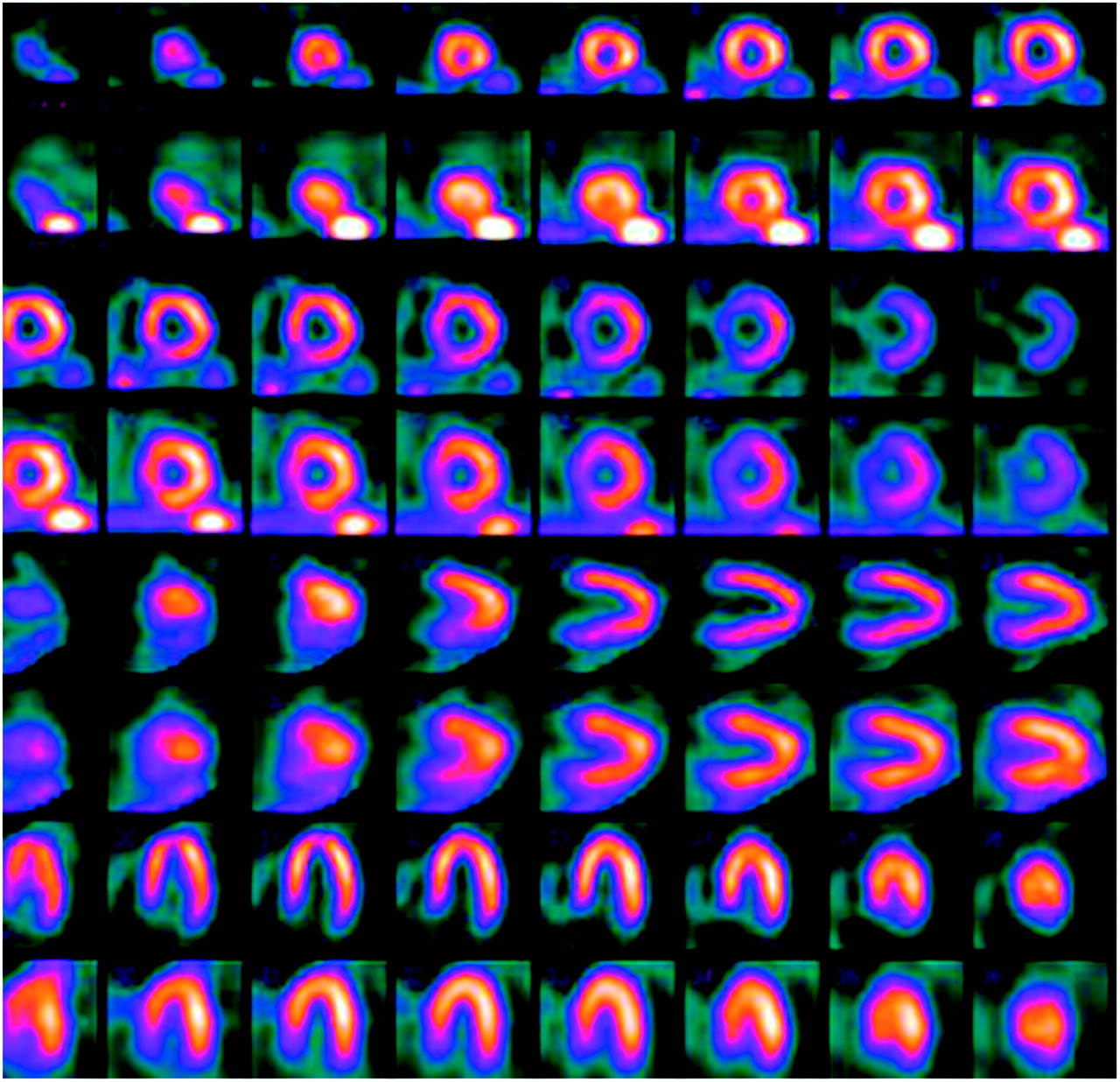
For viability assessment, the patient can be given a second injection of thallium and reimaged on the following morning; alternatively, thallium can be given the night before imaging begins. Figure 2 is a diagram of dual-isotope imaging protocol options. The images from a normal dual-isotope study are shown in Figure 3.
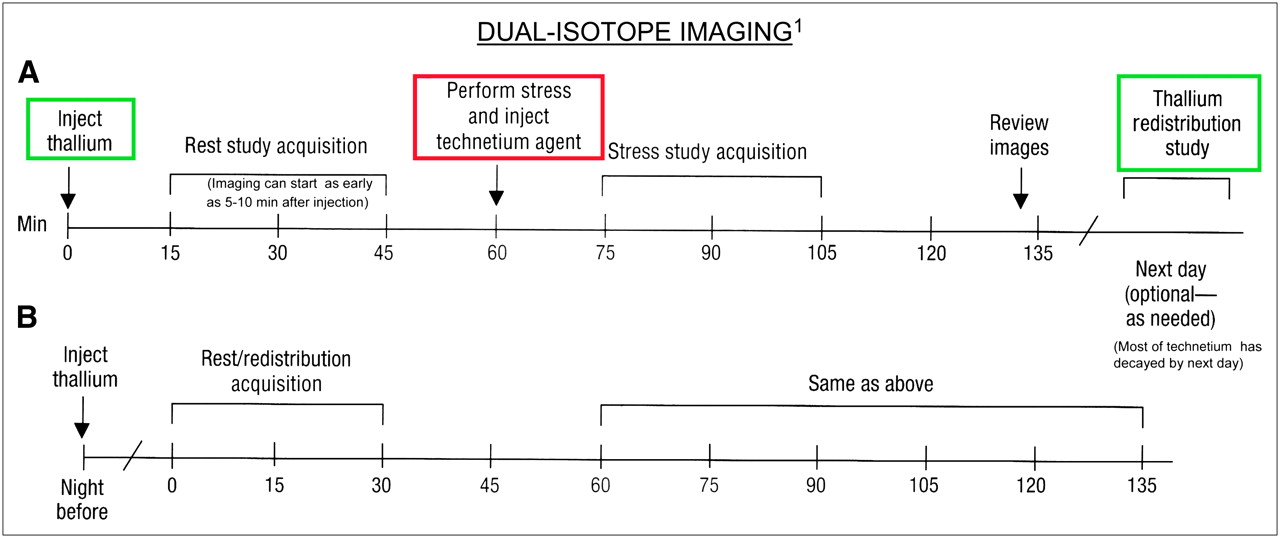
Dual-isotope imaging. Reprinted from Crawford ES, Husain SS. Nuclear Cardiac Imaging: Terminology and Technical Aspects. Reston, VA: Society of Nuclear Medicine; 2003;33.
Images obtained with 99mTc-sestamibi (top row of each pair of rows) and 201Tl (bottom row of each pair) in dual-isotope protocol. Findings are normal.
The advantages of the dual-isotope separate-acquisition protocol are as follows: a short duration of the entire study (<2 h); no need for cross talk correction; insignificant contribution of counts from 201Tl to the 99mTc window; minimization of the problem of cross contamination; optimal defect contrast; comparable rest and stress images; true rest study, which allows a better evaluation of reversible defects; viability assessment; favorable dosimetry; patient convenience; and sensitivity and specificity of ∼90%.
The disadvantages of the dual-isotope separate-acquisition protocol are as follows: comparison of stress–rest images obtained with 2 isotopes with different characteristics; variability in attenuation factors; differences in image resolution; greater Compton scatter of 201Tl than of 99mTc; greater myocardial wall thickness with 201Tl than with 99mTc because of increased scatter; less-than-optimal transient ischemic dilatation evaluation because of left ventricular cavity being larger with 99mTc; difficulty in evaluating minimal reversible defects; and low photon energy of 201Tl, a feature that is not ideal for obese patients.
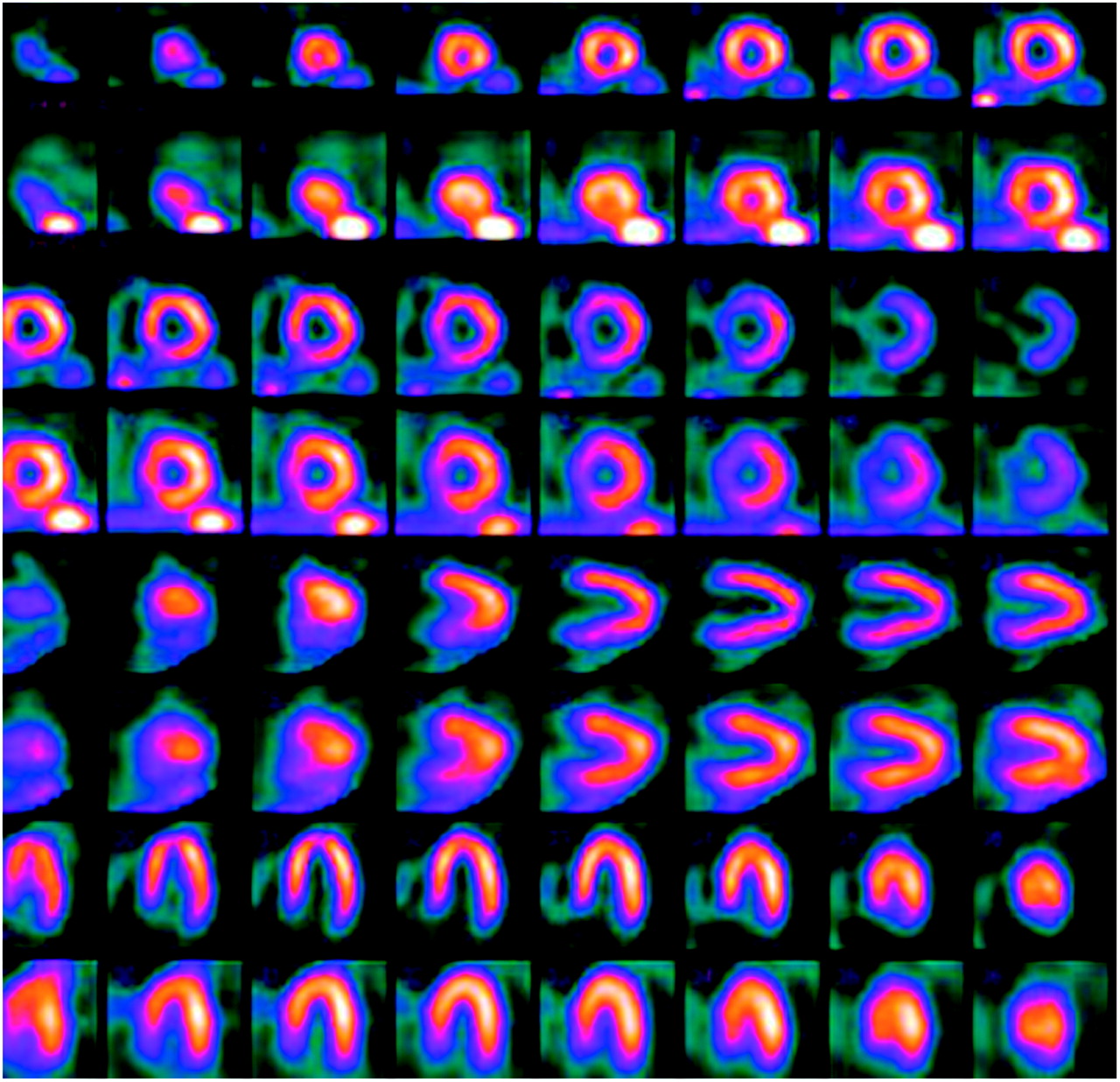
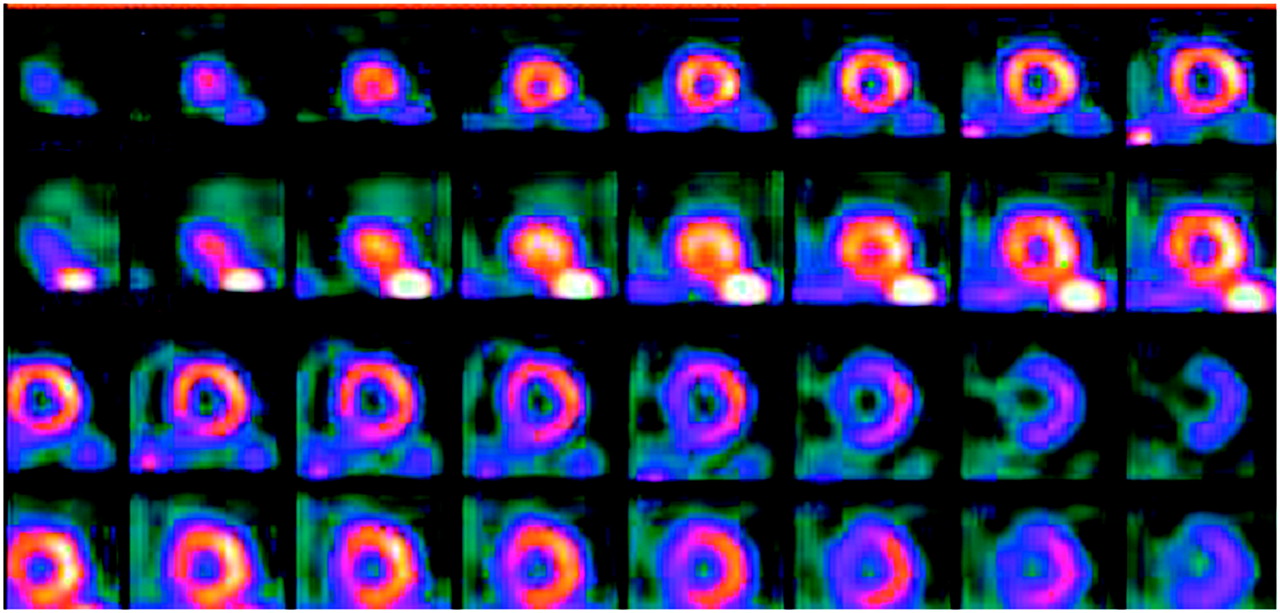
Figure 4 shows the normal cavity size difference between a 201Tl scan and a 99mTc-labeled agent scan. Myocardial wall thickness is greater with 201Tl than with 99mTc-labeled agents. This normal difference in cavity size is attributable to 201Tl scatter.

Normal cavity size difference between images obtained with 99mTc-sestamibi (top row of each pair of rows) and those obtained with 201Tl (bottom row of each pair) in dual-isotope protocol.
Dual-Isotope Simultaneous-Acquisition Protocol.
The dual-isotope simultaneous-acquisition protocol is based on the unproven assumption that the effect of cross talk between the energy windows of 201Tl and 99mTc is insignificant. Downscatter of high-energy 99mTc-sestamibi into the lower-energy 201Tl window results in an ∼20% reduction in defect contrast with 201Tl and in the overestimation of defect reversibility (12). Downscatter correction methods are not conclusive and have not been clinically validated.
For the simultaneous rest 201Tl–stress 99mTc-sestamibi SPECT protocol, 111 MBq (3.0 mCi) of 201Tl is injected at rest. The stress study is performed within 30 min. After the stress acquisition, 925 MBq (25 mCi) of 99mTc-sestamibi is injected at peak exercise, and dual SPECT studies are acquired within 30 min.
The advantages of the dual-isotope simultaneous-acquisition protocol are as follows: no need for 2 separate imaging sessions; reduced camera acquisition time; shorter study duration; fewer motion artifacts than with separate rest and stress acquisitions; and exact registration between images obtained with 201Tl and images obtained with 99mTc.
The disadvantages of the dual-isotope simultaneous-acquisition protocol involve cross talk and downscatter; the contribution of scattered and primary photons from the first radionuclide into the photopeak window of the second radionuclide results in a significant degradation of image quality, image resolution, and quantitation. This protocol is not recommended because of the problem of downscatter.
Dual-Isotope Cross Talk Correction Methods.
Several methods are available for correcting dual-isotope cross talk. Downscatter correction methods are not conclusive and have not been clinically validated. A detailed review of various methods is available in physics books dealing with this subject.
Moore's correction method corrects only for the contribution of 99mTc to the 201Tl primary 70-keV window. The 3-window transformation method involves 2 single-isotope acquisitions and 1 dual-isotope acquisition. Simultaneous cross talk correction by this method is slightly better than that by Moore's correction method. In the convolution cross talk correction method, convolution filters are derived from point response functions for 99mTc and 201Tl point sources. Acquisitions are done with 99mTc only, 201Tl only, and with a mixture of 99mTc and 201Tl. The average point response function is used in the creation of a filter.
CONCLUSION
There is no single best protocol that addresses all of the issues. From the standpoints of tracer kinetics, physical properties, and the laws of physics, the 2-d 99mTc-labeled agent myocardial perfusion imaging protocol is perhaps the best. The 1-d rest–stress 99mTc-labeled agent myocardial perfusion imaging protocol may be a better choice for some clinics. The 1-d dual-isotope separate-acquisition protocol is a good alternative. The dual-isotope simultaneous-acquisition protocol is a suboptimal choice until an approach for downscatter correction is conclusive and validated clinically.
Again, there is no single best protocol. Each protocol has advantages and disadvantages, which must be understood and taken into consideration when one is choosing a protocol. The staff members in each clinic need to determine which protocol will work best for them and consistently maintain it for better comparison when repeat studies are performed on the same patient.
Acknowledgments
The author acknowledges the contributions of Elpida S. Crawford, Nuclear Medicine Technology Program, School of Medicine and Biomedical Sciences, State University of New York at Buffalo, who kindly provided comments on this article and developed the continuing education questions.
Footnotes
-
↵* NOTE: FOR CE CREDIT, YOU CAN ACCESS THIS ACTIVITY THROUGH THE SNM WEB SITE (http://www.snm.org/ce_online) THROUGH MARCH 2008.
-
COPYRIGHT © 2007 by the Society of Nuclear Medicine, Inc.
References
- Received for publication November 7, 2006.
- Accepted for publication January 29, 2007.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
- Article
- Abstract
- RADIOPHARMACEUTICALS
- COMPARISON OF 201TL AND 99MTC-LABELED MYOCARDIAL PERFUSION IMAGING TRACER KINETICS
- RELATIONSHIP BETWEEN CORONARY BLOOD FLOW AND MYOCARDIAL UPTAKE OF VARIOUS RADIOTRACERS
- PHYSICAL AND BIOLOGIC COMPARISONS OF MYOCARDIAL PERFUSION IMAGING AGENTS
- VARIOUS IMAGING PROTOCOLS
- CONCLUSION
- Acknowledgments
- Footnotes
- References
- Figures & Data
- Info & Metrics