


Abstract
On the basis of previously unpublished observations, we hypothesized that prolonged use of proton pump inhibitors (PPIs) causes an increase in 99mTc-sestamibi uptake in the stomach wall, manifested as curvilinear activity surrounding the photopenic fundus of the stomach cavity. We prospectively evaluated the frequency of stomach wall uptake in patients undergoing myocardial perfusion SPECT who were taking PPIs or H2 antagonists. Methods: Patients (n = 138) who were scheduled for single-day rest/stress 99mTc-sestamibi SPECT were randomly selected. Poststress SPECT was performed 30 min after treadmill exercise or 45 min after dipyridamole infusion. The rest scan was obtained 45 min after tracer injection. All patients drank 473 mL of water 5–10 min after both the rest and the stress radiotracer injections. Patients were questioned regarding their use of PPIs and H2 antagonists. The significant use of either was defined as more than 2 wk of continuous therapy before cardiac SPECT. Masked observers assessed poststress planar projection images in endless-loop cinematic format for the following 3 patterns: stomach cavity uptake, attributable to duodenogastric reflux of tracer; stomach wall uptake; and no stomach uptake. A 2-tailed χ2 test with Yates correction was used to calculate statistically significant associations among variables. Results: Only patients with observed patterns of stomach wall uptake (n = 30) and no stomach wall uptake (n = 91) were included. Patients with stomach cavity uptake (n = 17) were excluded because the assessment of the adjacent stomach wall uptake was not possible. Of the patients included (n = 121), 30 were men and 91 were women. Sixty-seven patients were older than 60 y; 26 patients were taking PPIs. Of the 95 patients not taking PPIs, 14 were taking H2 antagonists. No patients were taking both medications. Stomach wall uptake was strongly associated with prolonged use of PPIs (χ2 = 51.9, P < 0.0001). No statistically significant association was noted among age, sex, or use of H2 antagonists (P = NS). Conclusion: Prolonged PPI therapy, but not H2 antagonist therapy, contributes to a significant increase in stomach wall activity, potentially resulting in Compton scatter or ramp filter artifacts affecting the inferior wall of the left ventricle. Stomach wall activity, unlike the stomach cavity activity, cannot be prevented by the ingestion of water before imaging. Therefore, it is important to elicit a history of prolonged PPI use to better anticipate the possibility of increased stomach wall activity, which can confound the image quality and interpretation.
Gated SPECT is the current widely used routine approach to myocardial perfusion imaging (1). However, myocardial perfusion imaging is affected by imaging artifacts, which lower the specificity of this technique in the diagnosis of coronary artery disease (CAD). Multiple factors can introduce artifacts in the 99mTc-sestamibi images. Numerous articles in the literature describe various artifacts on the 99mTc-sestamibi cardiac images (2–6). During our daily image review sessions, we observed that some of the patients had curvilinear activity in the stomach wall. This activity was mostly inferior or inferolateral to the heart and was responsible for false-positive or false-negative artifacts in the inferior wall of the left ventricle after image reconstruction. On further exploration, we found that most of these patients were taking proton pump inhibitors (PPIs) on a regular basis. Therefore, we hypothesized that PPIs were the cause of stomach wall activity.
MATERIALS AND METHODS
This was a prospective study performed at a single center. The study included only outpatients. In-hospital patients were excluded because of significant routine use of prophylactic in-hospital PPIs.
Patient Population
Patients (n = 138) who were willing to complete the routine questionnaire were randomly selected. Patients were asked if they had an indigestion, heart burn, or an acid reflux problem and if they were taking any medication related to this problem. Patients were specifically questioned regarding their use of PPIs and H2 antagonists. The significant use of either was defined as more than 2 wk of continuous therapy before cardiac SPECT. Of 138 patients, 17 patients had stomach cavity uptake and were excluded because the assessment of adjacent stomach wall uptake was not possible. Of the 121 patients included in the study, 30 were men and 91 were women between the ages of 24 and 90 y (average age ± SD, 62.4 ± 13.5 y). Twenty-six patients were taking PPIs. Of the 95 patients not taking PPIs, 14 were taking H2 antagonists. No patients were taking both medications.
Imaging Protocol
All patients underwent 1-d rest/stress 99mTc-sestamibi SPECT. During the 1-d rest/stress protocol, the patient ingested nothing (by mouth) for 4–6 h before the study, with no caffeine and no β-blockers or other related antihypertensive medications the night before. Patients received 296–444 MBq of 99mTc-sestamibi for the rest study and 1,184–1,776 MBq of 99mTc-sestamibi (3–4 times > the resting dose) for the stress study. The stress was either pharmacologic or treadmill exercise, using the standard or modified Bruce protocol. The electrocardiogram and blood pressure were monitored. For exercise, the tracer was injected at peak exercise, and exercise was continued for 90 s after injection. For pharmacologic stress, mostly dipyridamole was used; dobutamine was used in cases of asthma or chronic obstructive pulmonary disease. For dipyridamole stress, the tracer was injected at 3 min after dipyridamole infusion. For dobutamine stress, electrocardiograms and blood pressure were checked every minute. Dobutamine was infused at a rate of 10 μg/min for 3 min and then increased to 20 μg/min, 30 μg/min, and 40 μg/min for each consecutive 3-min interval. An atropine bolus (0.25 mg), administered intravenously, was given when needed. The tracer was injected at peak dobutamine infusion, and dobutamine infusion was continued for 90 s after tracer injection. Poststress SPECT was acquired 30 min after treadmill exercise or 45 min after dipyridamole or dobutamine infusion. All patients drank 473 mL of water 5–10 min after both rest and stress radiotracer injections, to remove any activity within the stomach.
Data Acquisition
Either a GE Ventri (30 stops; zoom, 1.0), a GE Optima (32 stops; zoom, 1.0), a GE MG Millennium (36 stops; zoom, 1.33), or a GE Maxxus XC/T (32 stops; zoom, 1.33) was used for image acquisition. Patients were supine with their arms above the head. For the rest study, a 64 × 64 matrix and 25 s/stop were used. For the stress study, a 64 × 64 matrix and 20 s/stop plus 8-frame electrocardiogram gating were used. The acquisition started at −45° (right anterior oblique) and rotated clockwise in a circular orbit. Gated rhythm acceptance was 100%. The collimator was low-energy, high-resolution.
Data Reconstruction
For image processing, Myovation (GE Healthcare) software was used. The reconstruction technique was ordered-subset expectation maximization.
Data Analysis
Two experienced nuclear medicine physicians assessed poststress planar projection images of emission stress and rest data without scatter correction in endless-loop cinematic format for the following 3 patterns: stomach cavity uptake, attributable to duodenogastric reflux of tracer; stomach wall uptake; and no stomach uptake.
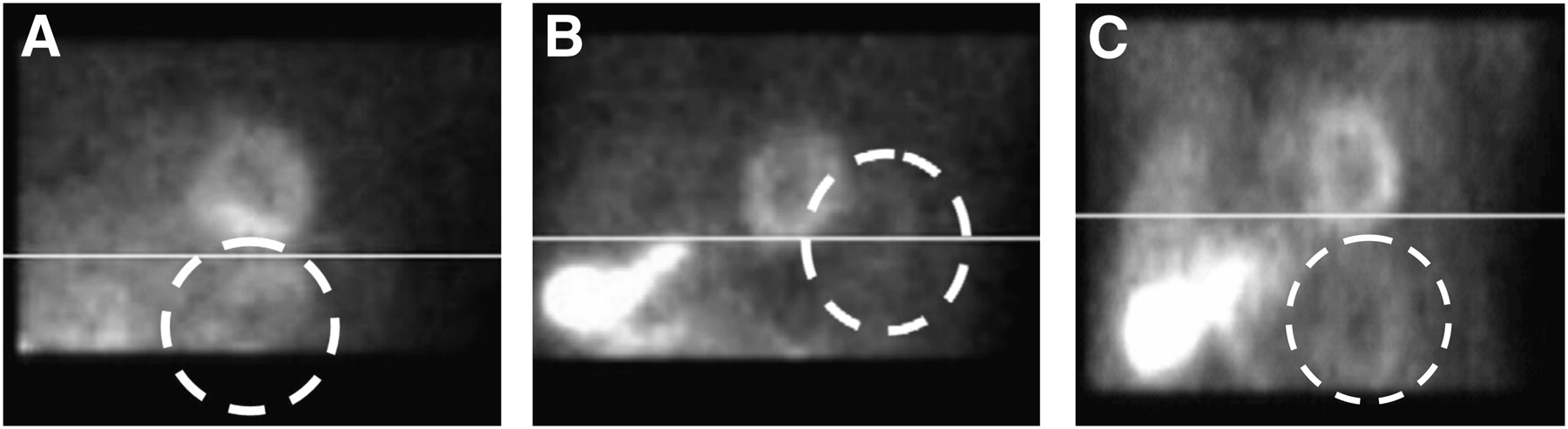
Poststress images only were analyzed because they had better quality than did the rest images (Fig. 1).
RESULTS
In our preliminary study, we found that there was a positive correlation between the use of PPIs and stomach wall uptake. A 2-tailed χ2 test with Yates correction was used to calculate any statistically significant association between stomach wall activity and the following variables: PPI use, H2 antagonist use, age, and sex.
Stomach wall uptake was strongly associated with prolonged use of PPIs (χ2 = 51.9, P < 0.0001) (Table 1). No statistically significant association was noted for the use of H2 antagonists (χ2 = 0.001, P < 0.97), age (χ2 = 0.142, P < 0.70), or sex (χ2 = 0.154, P < 0.69) (Tables 2, 3, and 4, respectively).
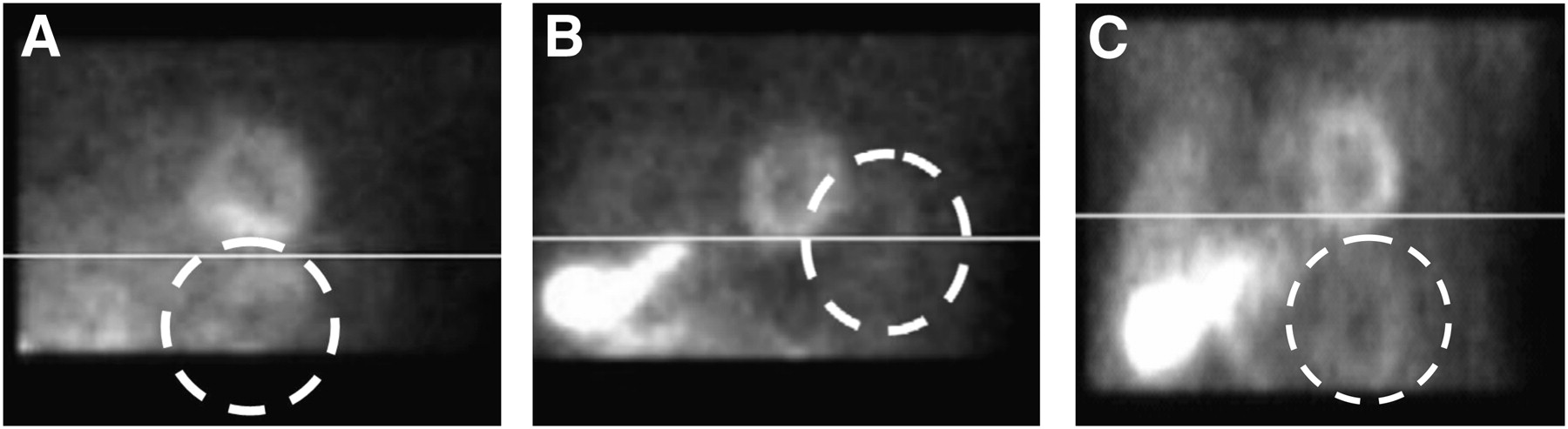
99mTc stress images showing curvilinear activity in stomach wall interfering with inferior wall of left ventricle (dashed circle). Reconstruction using different filters can induce artifacts.
Association Between Stomach Wall Uptake and PPIs (n = 121)
Association Between Stomach Wall Uptake and Antagonists (n = 87)
Association Between Stomach Wall Uptake and Age (n = 121)
Association Between Stomach Wall Uptake and Sex (n = 121)
DISCUSSION
CAD is the main cause of death in elderly patients. SPECT with 99mTc-labeled agents is extremely useful for the diagnosis and risk stratification of CAD (2). The first-pass myocardial extraction fraction of 99mTc-sestamibi is 55%−68%. 99mTc-sestamibi myocardial cellular retention occurs specifically within the mitochondria as a result of an electrostatic interaction (3). Myocardial retention is prolonged. The myocardial uptake of 99mTc-sestamibi is 1.2%−1.5% of the injected dose (3). 99mTc-sestamibi shows minimal redistribution. The radiation dosimetry is favorable, with an absorbed dose of 0.50 rad to the total body (3,4). The prognostic value of the study result is also good. Patients with stable chest pain syndromes and normal stress SPECT sestamibi findings have a low risk of death or nonfatal MI. Patients with abnormal findings have an intermediate to high risk for future cardiac events, depending on the degree of the abnormality (5).
Despite all of the advantages cited for the 99mTc-labeled myocardial perfusion tracer sestamibi, the tracer suffers from extracardiac localization, most commonly in the stomach, liver, bowel, and spleen (6). Interference from extracardiac radionuclide activity prevents the accurate interpretation of the true myocardial perfusion distribution (7,8). Compton scatter from the bowel degrades image quality in 99mTc-sestamibi myocardial perfusion imaging, artifactually increasing count density in the inferior myocardial wall (9). In contrast, subdiaphragmatic activity is in the x-plane of the heart; the ramp filter artifact may decrease the count density of the inferior wall (10). There have been several methods described within the literature to minimize the effect of extracardiac activity on the interpretation of the images. These techniques include delaying imaging; ingesting water, milk, or food; altering the patient's position; or using various prokinetic medications (6,11–20). In 1 study, researchers compared the efficacy of milk alone versus milk and water simultaneously (12). The authors concluded that administration of both whole milk and water to the patient at specific times improved the quality of attenuation-corrected myocardial perfusion SPECT images, thus facilitating the interpretation of the inferoposteroseptal myocardial wall. When SPECT is performed without attenuation correction, a glass of whole milk may suffice. Another study described the use of oral contrast and water to improve image variability and contrast by decreasing the infracardiac scatter (9). Another study demonstrated the advantages of a full stomach to reduce scatter artifact in the inferior wall, arising because of intestinal activity (15). Another article described the use of metoclopramide to increase gut mobility in an attempt to move the gut activity away from the heart. However, this approach ultimately showed no benefit (21).
We observed unusual curvilinear activity within the stomach wall. The sestamibi activity within the stomach wall differs from other extracardiac activities because it is not cleared by food or ingestion of water. To our knowledge, there has been only 1 study in the literature describing this activity. In that report, stomach wall uptake occurred in 1.6% of patients (n = 13); all of the patients had some kind of dyspepsia (22).
The mechanism of action of the PPIs on uptake of sestamibi within the stomach wall is not clear. Many of the proposed mechanisms for uptake of sestamibi within the cell are derived from studies of myocardial tissue. The fundamental mechanism of myocellular accumulation of sestamibi most probably involves passive diffusion across the sarcolemmal and mitochondrial membranes in response to transmembrane potentials (23–25). Sestamibi is a lipophilic cation, concentrated in the mitochondria (26). In the myocardium, limitation of the blood supply may result in decreased 99mTc-sestamibi uptake. Extraction, however, appears to be dependent on the transmembrane potential difference (23,24).
In patients with acid reflux disease, the blood flow is decreased, possibly causing less sestamibi uptake in the parietal cells. It is known that parietal cells have an abundant content of mitochondria, but gastric diseases associated with dyspepsia are more likely to cause a decrease in these cells. Thus, neither of these mechanisms supports the sestamibi uptake and retention in the parietal cells.
PPIs act by irreversibly blocking the hydrogen/potassium adenosine triphosphatase enzyme system (H+/K+ ATPase) or more commonly just the gastric proton pump of the gastric parietal cell at the secretory surface of the cell (27,28). The proton pump is the terminal stage in gastric acid secretion, being directly responsible for secreting H+ ions into the gastric lumen, making it an ideal target for the inhibition of acid secretion. Targeting the terminal step in acid production and the irreversible nature of the inhibition result in a class of drugs that are significantly more effective than H2 antagonists, reducing gastric acid secretion by up to 99%. The preliminary thinking beyond this process is that sestamibi is also taken up by gastric parietal cells because of abundant mitochondria. Inhibition of the H+/K+ ATPase pump reduces the secretion of sestamibi from the gastric wall into the gastric lumen in a manner similar to the reduction of acid secretion.
Stomach wall activity, because of its proximity to the inferior myocardial wall, could in some circumstances lead to either false-negative or false-positive myocardial perfusion SPECT findings due to either Compton scatter or ramp filter artifacts. In the case of Compton scatter, this linear tubular activity also could be superimposed (i.e., scattered) onto the myocardial activity, masking a true inferior perfusion defect and giving the nuclear medicine physician the illusion that the inferior wall activity is normal. This phenomenon has been described using the 2-d stress/rest protocol as well (22). The study by Côté and Dumont also has explained the possible use of a full stomach to minimize stomach wall activity. These authors noticed that the sestamibi activity of the gastric wall was diminished significantly with food or a soft drink, probably by an effect of partial volume. This reduction in sestamibi activity significantly improved the quality of the images, but stomach wall activity did not disappear. We question if this gastric wall activity could be minimized or eliminated by stopping the PPIs for a few weeks before scheduling the patient for myocardial perfusion scanning.
CONCLUSION
Stomach wall activity is completely different from the well-known stomach cavity activity frequently observed secondary to enterogastric reflux of sestamibi. The patients in our study who showed significant stomach wall activity had acid reflux disease of a chronic nature and were taking PPIs. Prolonged PPI therapy, but not H2 antagonist therapy, contributes to a significant increase in stomach wall activity, potentially resulting in Compton scatter or ramp filter artifacts affecting the inferior wall of the left ventricle. Stomach wall activity, unlike the stomach cavity activity, cannot be prevented by the ingestion of water before imaging. Other investigators have reported a possible role of a full stomach in diminishing this activity. Therefore, it is important to elicit a history of prolonged PPI use to better anticipate the possibility of increased stomach wall activity, which can confound the image quality and interpretation. The mechanisms explaining this stomach wall activity remain speculative.
Footnotes
-
COPYRIGHT © 2009 by the Society of Nuclear Medicine, Inc.
References
- Received for publication May 5, 2009.
- Accepted for publication October 16, 2009.





{kind=link}